

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Retinal detachment
Ähnlich wie Retinal detachment (20)
Mehr von MEDICS india
Mehr von MEDICS india (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Retinal detachment
- 1. RETINA – RETINAL DETACHMENT 11 th June 2020 May 2020AL KERATITIS DR M SAQUIB MBBS,MS , FSCEH DELHI,FHVDESAI PUNE, EX REGISTRARA JNMCH,AMU CONSULTANT OPHTHALMOLOGIST HOD D/O OPHTHALMOLOGY G.S .MEDICAL COLLEGE Founder sec: MEDICS India , Mail-dms2k5@gmail.com , 9634123800
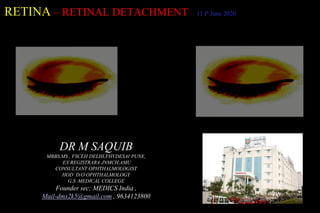
- 2. • Seperation of Neurosensory Retina from the Retinal Pigment Epithelium ,with the accumulation of sub retinal fluid condition ..Retinal Detachment • vitreous liquid leaks through retinal tear and accumulates underneath retina retina can peel away from underlying layer of blood vessels • Firmly Adherent To The Underlying Bruch’s Membrane of choroid • And Loosely Arranged To The Layer Of Rods And Cones • The Potential Space Between RPE And The Sensory Retina Is Called Subretinal Space
- 3. • Rhegmatogenous RD • Tractional RD • Exudative RD
- 4. Rhegmatogenous RD • 1: 10000 • Both Eye eventually involved 10% • 45-65 years • Early Age if Predisposed
- 5. For asymptomatic patients who are at risk for retinal detachment, a dilated fundus examination should be performed at the first examination and periodically thereafter. Common risk factors include • Aging - More Common In People Older Than 40 • Previous Retinal Detachment In One Eye • Family History Of Retinal Detachment • Extreme Nearsightedness • Previous Eye Surgery • Previous Severe Eye Injury Or Trauma • Capsulotomy (Especially The 6 Months Following The Procedure) • Proliferative Retinopathies (Proliferative Stage Diabetes, Sickle Cell, Branch Retinal Vein Occlusion) • Lattice Degeneration • Open-angle Glaucoma In Myopic Patients Treated With Strong Miotic Agents
- 6. High myopia—the thin, stretched retina of high myopic eyes is at risk for tears (greater than 5 diopters 2% risk, greater than 10 diopters, 5% risk).
- 9. Pathogenesis • POSTRIOR VITREOUS DETACHMENT : Separation of Cortical Vitreous from Internal Limiting Membrane of the Neurosensory Retina posterior to the vitreous base .
- 11. Primary prevention • Risk factors for retinal detachment should have serial dilated fundus examinations with scleral depression, often yearly. • Protective eyewear is recommended for individuals with high myopia that participate in contact sports. • Patients undergoing cataract surgery should be counseled about the importance of reporting symptoms of retinal tears and detachments.
- 12. History • New onset significant photopsias and/or persistent new floaters should be suspected of having a retinal tear, which could lead to a retinal detachment. • A patient with constant fixed or slowly progressive visual field loss should be suspected of having a detachment until proven otherwise. • onset of symptoms, presence and duration of decreased central visual acuity, prior trauma, prior surgery, Haemorrhage, and a complete past medical history and review of systems.
- 14. Symptoms • Photopsia – Flashes of Light ,Vitro-Retinal irriation • Floaters : bits of debris in field of vision that look like spots, hairs or strings • Shadow Encroaching to field of vision / Curtain like effect . • Sudden Painless loss of vision
- 15. External Examination Signs • Intraocular Pressure-Slighty lower • Marcus Gunn pupil –RAPD • Distant direct Ophthalmoscopy –No Red Reflex , Greyish Reflex • Ophthalmoscopy – Direct /Indirect with Indentation • Visual Field Charting – Relative to Absolute scotoma • ERG –Abnormal to Absent • Ultrasonography - Role in Dense cataracts ,Vitreous haemorhage , Hazy media
- 16. Ophthalmoscopy • Freshly Detached Retina – Grey Reflex , convex configuration , Oscillate with movement of eye Bullous RD , Funnel RD ,Total TRTD • Retinal Break- Periphery , Upper-Temporal • Vitreous pigments : Anterior vitreous ( tobacco dusting /shaffer sign ) with PVD • Old Retinal Detachment
- 17. Clinical Diagnosis Clinical diagnosis • Rhegmatogenous Retinal Detachment Has A Corrugated Appearance And Undulates With Eye Movements. • Tractional Detachments Have Smooth Concave Surfaces With Minimal Shifting With Eye Movements. • Serous Detachments Show A Smooth Retinal Surface And Shifting Fluid Depending On Patient Positioning. • In The Vast Majority Of Cases, A Retinal Break Will Be Identified With Proper Examination, Thus Confirming A Rhegmatogenous Retinal Detachment. • Without Visualization Of A Retinal Break, The Diagnosis Of Rhegmatogenous Retinal Detachment Should Be Questioned,
- 19. Differential Diagnosis • Retinal Detachment Includes Retinoschisis, Choroidal Mass. Rhegmatogenous Retinal Detachment Is Most Often Confused With Retinoschisis And Serous Retinal Detachment. Retinoschsis Can Be Distinguished From Retinal Detachment By Appearance On Ultrasound,
- 21. COMPLICATION • Longstanding RD • Proliferative Vitroretinopathy (PVR) • Complicated cataract Uveitis
- 22. TREATMENT • Principles : Sealing of Retinal Breaks Reducing the Vitreous Traction on Retina Flattening of Retina by SRF Drainage Tamponade ( External/Internal )
- 23. • 1.SEALING OF RETINAL BREAK – Aseptic Chorioretinitis Cryocoagulation/Photocoagulation / Diathermy • 2.Drainage of SRF – Apposition between sensory Retina and RPE .Fine needle through the sclera and choroid into subretinal space .Not required in all cases
- 24. 3.Maintenance Of Chorioretinal Apposition • Pneumatic retinopexy Injection of an intraocular gas bubble along with retinopexy using cryotherapy or laser., An important part in the successful repair of retinal detachment with pneumatic retinopexy involves head positioning so that the gas bubble tamponades the retinal tear. Pneumatic retinopexy is typically only used with retinal detachments due to retinal tears in the superior eight clock hours and involving a single break less than one clock hour. • Scleral buckles are silicone bands permanently placed around the outside of the globe under the extraocular rectus muscles to relieve any traction and support retinal tears. Scleral buckling is combined with retinopexy, typically cryotherapy. oldest ,excellent results .
- 25. • Pars plana vitrectomy /Endolaser Photocoagulation and Internal Tamponade with 20 gauge, 23 gauge, 25 gauge, or 27 gauge instruments involves removal of the vitreous by way of cutting the vitreous strands with a vitrectomy machine/handpiece and flattening of the retina through a direct intraocular process. • Indication- Complicated primary RD , Primary vitrectomy in Buckling case , Tractional RD • Steps- Pars plana vitrectomy 3 port –internal Drainage of SRF –Retina flattening by Injecting Silicone Oil /Perfluorocarbon liquid – Endolase – Internal tamponade ( Silicone oil or exchanged with gas like Sulfur Hexafluoride or Perfluoropropane) •
- 26. Prophylaxis • Retinal Break Laser or Cryo • Lattice degeneration “ “ • Myopia • Aphakia • RD in fellow Eye • Family History
- 27. TRACTION RETINAL DETACHMENT • Progressive contraction of fibrovascular membrane over large areas of vitroretinal adhesions .
- 29. Causes • Proliferative Diabetic Retinopathy (PDR) • Retinopathy Of Prematurity • Retinal Vein Occlusion • Proliferative retinopathy in Eale’s disease • Trauma ( Penetrating Posterior Segment ) • Sickling Hemoglobinopathies • Idiopathic Vasculitis
- 30. Presentation • Vitreoretinal Bands • Retinal mobility Reduced/ No shifting Fluid • NO Photopsia ,Floaters • No Vitreoretinal Traction is insidious and not associated with Acute PVD • DOV • Slow visual Field Defect
- 31. Signs • I.O : RD with Concave configuration • Sub Retinal Fluid –Shallow , Immobile • RD rarely extend to Ora serrata . • No Retinal Break
- 32. Treatment • Systemic cause • Vision threatening -0 Pars Plana VitrectomyPars Plana Vitrectomy to cut vitreoretinal Tractional Bands and Internal Tamponade with Long Acting Gas or Silicone Oil • Prognosis-Poor •
- 33. EXUDATIVE( Serous,Solid ) RETINAL DETACHMENT • Seperation of Neurosensory Retina from Retinal Pigment epithelium with the accumulation of Subretinal fluid or Neoplasm, SRF is derived from Retinal or Choroidal Vessels .
- 34. Causes • OCULAR • Inflammation : Posterior scleritis,Orbital cellulitis ,Sympathetic ophthalmia Harada’s Disease • Congenital Abnormalties– Choroidal Coloboma ,Familial Exudative Vitreoretinopathy( FEVR),Optic Pit • Vascular Disease- Central serous retinopathy ,Coat’s Retinopathy • Malignant- Choroidal Tumoour,Exophytic Retinoblastoma ,Haemangioma • Sudden Hypotony – Post Operative • Uveal Effusion Syndrome- Bilateral Detachment of Peripheral Choroid • Choroidal Neovascularisation
- 35. Systemic • Toxaemia of Pregnancy • Renal Hypertension • Blood dyscrasias • Polyarteritis Nodosa
- 36. Presentation • No Photopsia ( No Vitro Retinal Traction ) • No Retinal Break • Floaters - +/- If Vitritis is present • Visual Field Defect – Sudden ,Progressive • Simultaneous Bilateral Involvement
- 37. Signs • IO – Covex configuartion , Smooth Surface • SRF -Deep , Mobile – Shifting Fluid • Cause of RD may be apparent • Scattered Subretinal Pigment Clumps may be seen after Resolution ( Leopard Spots )
- 38. • For Rhegmatogenous Detachments, All Retinal Breaks Should Be Identified, Treated And Closed. Techniques For Repair Include Pneumatic Retinopexy, Scleral Buckle Or Vitrectomy, Or Combinations Of These Techiques.
- 39. In tractional detachments, tractional elements (usually epiretinal or subretinal membranes) must be relieved. This is typically accomplished with pars plana vitrectomy, but may be combined with scleral buckling as an adjunct. • serous detachments, management is nonsurgical. Any inflammatory disease or underlying mass should be identified and treated if possible.