ECTOPIC PREGNANCY.pptx
•Als PPTX, PDF herunterladen•
1 gefällt mir•52 views

Ectopic pregnancy: definition, sites of implantation, causes, clinical features, signs and symptoms, investigations, management.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie ECTOPIC PREGNANCY.pptx
Ähnlich wie ECTOPIC PREGNANCY.pptx (20)
Mehr von Sharda School of Nursing Science and Research, Sharda University
Mehr von Sharda School of Nursing Science and Research, Sharda University (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
ECTOPIC PREGNANCY.pptx
- 1. BY: MS. HAOKIP SENIOR TUTOR/LECTURER OBG NURSING SSNSR, SU
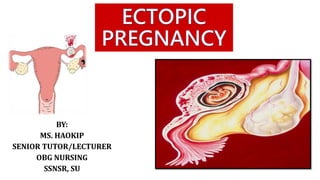
- 2. Pregnancy begins with a fertilized egg. Normally, the fertilized egg attaches to the lining of the uterus. An ectopic pregnancy occurs when a fertilized egg implants and grows outside the main cavity of the uterus. An ectopic pregnancy most often occurs in a fallopian tube, which carries eggs from the ovaries to the uterus. This type of ectopic pregnancy is called a tubal pregnancy. Sometimes, an ectopic pregnancy occurs in other areas of the body, such as the ovary, abdominal cavity or the lower part of the uterus (cervix), which connects to the vagina.
- 3. Incidence: 1-2% of pregnancies are Ectopic, but they account for up to 10 percent of maternal pregnancy- related deaths.
- 5. Exact cause is not known, it is believed that the following conditions can cause ectopic pregnancy: Hormonal factors. Damaged fallopian tubes by either previous injury or surgery. Genetic abnormalities. Abnormal development of fallopian tubes or other reproductive organs
- 6. CONTD… The risk factors include: Previous ectopic pregnancy. Sexually transmitted infections such as gonorrhea or chlamydia. Undergone fertility treatment. In rare cases, when IUDs are used for birth control. Smoking
- 10. A thorough history collection and physical examination. Lab. Investigations includes: Pregnancy Test (hCG) TVS CBC including blood grouping CT scan MRI
- 13. Expectant Management The term ‘expectant management’ is usually defined as watchful waiting or close monitoring by medical professionals instead of immediate treatment. Research has shown that, in patients with an ectopic pregnancy who are properly assessed and their pregnancy hormone level (beta hCG) is dropping, up to 50% of these pregnancies will end naturally and there will be no need for an operation or a drug to treat the condition
- 14. Expectant management would then be considered for treatment when: The hormone being made by the pregnancy (beta hCG) is low. General health appears to be stable. Pain levels are considered to be acceptable. An ultrasound scan shows a small ectopic pregnancy with no worrying bleeding into the abdomen
- 16. Pre-requisites for medical management of Ectopic Pregnancy Asymptomatic women with unruptured EP who are clinically stable, have normal baseline blood investigations (blood counts, liver and kidney function tests) and are willing for regular follow- up for 4–6 weeks, can be offered medical management. High serum hCG levels (> 3500 mIU / ml), ectopic mass size > 3.5 cm and / or presence of cardiac activity in EP are relative contraindications to medical management. Should not be offer to those significant bleeding cases.
- 17. Two protocols are currently used for medical treatment of EP: “Single Dose” MTX therapy at a dose of 50mg/m2 of body surface area and “Multidose” regimen consisting of 1mg / kg of MTX alternating with 0.1mg / kg of Leucovorin for upto 4 doses of each agent. Both regimens are found to be effective. MTX can be given on outpatient basis and intramuscular injection is the preferred route. Multidose regimen is preferred in women with high serum hCG levels or those with presence of cardiac activity on ultrasound. Further doses of MTX may be repeated depending upon the response to treatment.
- 20. Laparoscopy Salpingostomy and Salpingectomy are two laparoscopic surgeries used to treat some ectopic pregnancies. In these procedure, a small incision is made in the abdomen, near or in the navel. In a salpingostomy, the ectopic pregnancy is removed and the tube left to heal on its own. In a salpingectomy, the ectopic pregnancy and the tube are both removed
- 21. NURSING MANAGEMENT ASSESSMENT PRE & POST OP CARE INTERVENTIONS EDUCATION
- 22. ANY DOUBTS???