5 prevention of periodontal disease
•Als PPT, PDF herunterladen•
10 gefällt mir•2,702 views

5 prevention of periodontal disease

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie 5 prevention of periodontal disease
Ähnlich wie 5 prevention of periodontal disease (20)
Mehr von Lama K Banna
Mehr von Lama K Banna (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
5 prevention of periodontal disease
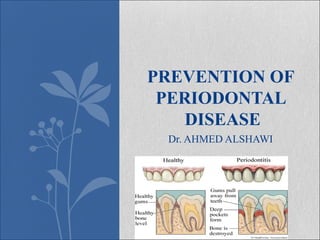
- 1. Dr. AHMED ALSHAWI PREVENTION OF PERIODONTAL DISEASE
- 2. eriodontal disease is the affection of the periodontium or the supporting tissues of the teeth. t may range in the same mouth from mild inflammation of the gingival margin (marginal gingivitis) to a severe destruction of the periodontal ligaments and the supporting alveolar bone. pidemiological surveys and clinical studies demonstrate a direct association between the prevalence and severity of periodontal diseases and the accumulation of bacterial plaque and debris. Personal care results in the resolution of the inflammation
- 3. ormal gingiva has been defined as pink, firm, stippled , with well-formed papillae and gingival sulci (crevices) shallow in depth and without exudate. Three areas are distinguished clinically in the gingiva, namely the interdental papilla , the gingival margin which forms the soft tissue wall of the gingival crevice/and the attached gingiva which is firmly bound down to the underlying cementum and alveolar bone.
- 4. he initiating factor leading to periodontal disease is the bacterial component of the plaque around the teeth or overlying the calculus on the teeth. he prevention of plaque accumulation or its regular removal is the best method of avoiding periodontal disease, and therefore the most important preventive measure is the effective use of the toothbrush and other devices when necessary. Today, only the mechanical action of the brush has been regularly shown to remove the bacterial and other soft deposits. There is sufficient evidence from Controlled clinical studies to suggest that keeping the teeth clean is an effective means of controlling periodontal disease.
- 5. hen the gingiva is inflamed , there is increased hyperemia, which shows as a deepening of the normal pink color to red, this is usually associated with bleeding either on brushing or spontaneously. The gingival margin and the interdental papillae are usually swollen and edematous. his results in shiny appearance of the surface with loss of stippling. Mild gingivitis is very prevalent among children often being limited to loss of stippling, swelling and slight redness.
- 6. n more advanced cases, however, marked redness with frequent bleeding may occur accompanied sometimes by soreness and etching, where inflammation has been present for a long period there may be an over growth of connective tissue specially in the anterior region where the gingivae become rough and irregularly enlarged. In more severe cases, destruction of the periodontal ligaments will occur, this may be accompanied by resorption of the alveolar bone, pocket formation, loosening and tooth migration. t puberty there is sometimes a pronounced gingivitis showing more swelling and discoloration than usual but after a time this may tend to improve although frequently treatment is also required.
- 8. Causes Of Periodontal Disease: hese may be conveniently divided into local and systemic predisposing though naturally. Any particular patient may be affected by more than one etiological factor. Local factors:
- 10. Local factors: 1. The consistency of the diet: is considered important on the basis of functional stimulation derived from mastication which is an essential requirement for the normal metabolic activity of the gingiva and underlying tissues. Soft foods are detrimental to the periodontium, first because they do not afford functional stimulation, and second , they faster accumulation of irritating food debris at the gingival margin. Bacterial activity in the food debris around the teeth and gums can cause damage to the underlying gingival tissues and initiate gingivitis.
- 11. Local factors: 2. Calculus: Although important in the adult is hardly an etiological factor in children since relatively few exhibit it .
- 12. Local factors: 3. The process of shedding of deciduous teeth and eruption of permanent teeth : are probably responsible for much of the gingivitis seen during the mixed dentition period. The child will avoid chewing on a loose or painful tooth allowing deposits to be left on and around the affected site.
- 13. Local factors: 4. Untreated caries: especially in cases of interproximal and cervical caries duedue to increased impaction or lodgment of food debristo increased impaction or lodgment of food debris. Poorly contoured restorations and overhanging cervical edges are also a cause of periodontal disease.
- 14. Local factors: 5. Occlusal abnormalities e.g. crowding of teeth, open bite, proclined maxillary incisors, and incompetent lips, are common cause of gingivitis by interfering with normal function and allowing food stagnation. Early extraction of a first permanent molar will prevent the normal cleansing effect of mastication and allow food stagnation around the tooth opposite the space.
- 15. Local factors: 6. Prosthetic and orthodontic appliances : constitute a significant local irritating factor particularly when poorly fitting or incorrectly designed.
- 17. Systemic factors: 1. Endocrinal disorders: Diabetes often permits an increased inflammatory gingival response, particularly if there is neglected oral hygiene. At puberty there are often hormonal changes and temporary upset in the gingival condition characterized by a rather swollen hemorrhagic appearance.
- 18. Systemic factors: 2. Drugs: The administration of certain drugs on long term basis may give rise to gingival alterations. The anticonvulsant drug "Dilantin" (Phenytoin ) causes characteristic gingival hyperplasia starting at the interdental papillae and spreading over other areas too, occasionally completely covering the teeth. In some cases the gum is rather firm and shows little tendency to bleed , in others a superadded gingivitis is present as well.
- 19. Systemic factors: 3. During acute fevers : such as typhoid and measles, deterioration of the gingiva may occur due to the concomitant poor oral hygiene butbut an improvement should be shown on recovery from the fever.
- 20. Systemic factors: 4. Blood dyscrasias, such as agranulocytosis, leukemia and purpura often exhibit gingival changes and these may even be the first symptoms experienced by thefirst symptoms experienced by the patient.patient.
- 21. Systemic factors: 5. Avitaminosis may affect the gingiva; particularly the lack of vitamin C, which gives rise to scurvy .
- 23. Preventive Measures: 1. Dental prophylaxis: It is more important in the control of periodontal disease than it is in the control of caries. This is because deposits of calculus are highly conductive to periodontal disease and cannot be removed by the patient in the course of home care. Patients with a tendency to gingivitis must be observed until it is known in how many months the accumulation of hard deposits upon the teeth will pass beyond the control of home care. Many periodontal patients must receive dental prophylaxis every 3 months or every 4 months, in addition to whatever more extensive treatment may be necessary at the hand of the dentist. Posterior bite-wing X-ray films should be taken at annual intervals and studied for any alveolar bone loss. If calculus forms in a child's mouth, a thorough prophylaxis should be carried out and repeated at intervals; in addition, the child's brushing habits should be checked to try to prevent any recurrence.
- 24. Preventive Measures: 2. Good oral hygiene: The stressing, from an early age, on the importance of good oral hygiene in assisting the natural cleansing action of the mouth is valuable; in addition, it should be recommended that children eat some hard, fibrous and fresh foods in addition to the rather soft diet prevalent today. It must be stressed also that the toothbrush is really a mouth brush and the care of the gingivae is just as important as that of the teeth.
- 25. Preventive Measures: 3. Tooth brushing: It is the most commonly recommended measure for the removal of food debris and plaque from the teeth mechanically. On the basis of the motion, methods of brushing are different, from vertical, horizontal, roll, circular to scrub method , None of them has been shown to be superior to others. The thoroughness of plaque and debris removal depends upon the careful and correct application of any brushing method rather than the applied methods itself. The roll technique mentioned before can be suggested, other techniques are beneficial particularly when periodontal disease is existing; these are:
- 26. Brushing Methods A. Charter's method: The end of the bristles is placed in contact with the enamel of the tooth surface and the gingival tissue with the bristles pointing occlusally at an angle of 45 degree . Much lateral and downward pressure is then placed upon the brush and the brush is vibrated gently back and forth a millimeter or so. This gentle vibratory procedure forces the ends of the bristles between the teeth and cleans the interproximal tooth surfaces very well. This technique also massages the interdental tissues as well.
- 27. Brushing Methods B. Stiliman's method: • The brush is placed in approximately the same position as required for the beginning stroke of the roll method, except that it is nearer the crowns of the teeth. • The handle is vibrated gently in a rapid but slight mesiodistal movement. This technique forces the bristles into the interproximal spaces and handle the teeth in that area very well. It also adequately massages the gingival tissues. • As a final step of brushing, it is recommended to brush the dorsum of the tongue with brush. • This will increase its circulation and removes bacteria and waste products .
- 28. Preventive Measures: 4. Devices for entering individual crevices: Dental floss, tooth picks, rubber tips etc. are sometimes recommended for cleaning areas inaccessible to the toothbrush. They are beneficial in massaging the gingival tissues and cleaning the interproximal spaces. (The uses of these devices are discussed before).
- 29. Preventive Measures: 5. Oral irrigation: (discussed before).
- 30. Preventive Measures: 6. Early -treatment of carious cavities: To avoid gingival inflammation, caries should be treated as soon as a cavity is spotted. There is no urgent "big cavity" to cause wary and non-urgent "little cavity" warrants no such interest. Caries is caries in both conditions. Cervical cavities and interproximal cavities cause irritation of the neighboring gingival tissue, whereas an open occlusal cavity causes decreased function of the same side and results in the accumulation of debris. • The use of bite-wing films in the early detection of interproximal lesions is advisable because such early cavities may be missed on clinical examination only. • New restorations should be carefully inserted, contoured and polished to avoid food impaction and gingival damage. Old restorations should be checked for . improper contact, overhanging margins and defect at the tooth restoration junctional line.
- 31. Preventive Measures: 7. Disorders of occlusion: Early diagnosis of occlusal disorders and early treatment by preventive or interceptive measures will save the gingiva .
- 32. Preventive Measures: 8. Mouth breathing: This should be treated either by clearing the air passages (oro-nasal part) by surgical or medical specialists, or by orthodontic means as oral screen.
- 33. Preventive Measures: 9. Systemic diseases: Such as blood dyscrasias, endocrine disorders and vitamin deficiencies will need medical attention in addition to local treatment. Proper oral hygiene will add to the health of oral and periodontal tissues.