1. 1
Economic Causes of Obesity:
Cross-country analysis
Kate Bray
A project presented in part requirement of the degree of Bachelor of Arts with
honours in Economics of the University of the West of England, Bristol
Academic year of presentation: 2010/2011
Bristol Business School
2. 2
Abstract
This dissertation provides a broad summary of the previous economic literature on obesity.
The literature, both theoretical and empirical, aims to explain the rise in obesity in recent
years and to identify the factors contributing towards the epidemic. The dissertation then aims
to analyse some of the factors thought to contribute towards obesity rates and to then use
econometric models to perform cross-sectional analysis of the significance of these factors,
differentiating between males and females. An understanding of the causes of obesity allows
economic policymakers to develop future policies which could help reverse the trend in rising
obesity rates around the world.
3. 3
CONTENTS
4 Introduction
5-9 Literature Review
10-16 Method
Rationale for choosing variables
Data collection
17-23 Regression Analysis (1)
24 Correlation Analysis
25 Correlation Matrix
26-31 Regression Analysis (2)
32-33 Physical Activity Model
34-36 Case Studies
US and Canada Comparison
Samoan Women
Japan
37-38 Evaluation
39 Conclusion
40-44 Acknowledgements & References
45–60 Appendix
4. 4
INTRODUCTION
“To say that obesity is caused by merely consuming too many calories is like saying that the
only cause of the American Revolution was the Boston Tea Party.” – Adelle Davis.
This dissertation aims to undertake econometric analysis into the varying degrees of
significance of factors affecting obesity rates in adult males and females, across 55 countries
worldwide: 26 European, 5 African, 2 South-East Asian, 7 Western Pacific, 5 Eastern
Mediterranean, 3 South American, 1 central American and 6 North American countries.
Several economic factors affect the amount of food we eat and the amount of physical
activity we take part in and ultimately our weight. The worldwide accepted definition of
obesity is people who have a body mass index (BMI) ≥30. The BMI is calculated by dividing
body weight (kg) by height (m) and squaring that number. The worldwide obesity problem is
a great cause of concern and, over the past few decades, obesity rates have been climbing at
an alarming rate. The cost to governments has been billions of pounds a year in health costs.
The World Health Organization (WHO) reported in 2003 there were at least 300 million
obese people worldwide. Obesity leads to detrimental changes in people‟s metabolism and an
increase in blood pressure and cholesterol. It can also increase the risk of heart disease,
strokes and cancer (WHO,2003). Obese people suffer serious chronic diseases, reduced
quality of life, shortened life expectancies and lowered levels of labour productivity, each of
which impedes a country's growth and development. (Gardner & Halweil, 2000). The obesity
problem used to be generally limited to the high-income countries of the world but in recent
years the problem has spread to developing countries. Therefore, if we can find out more
about the causes of obesity, then we should be closer to finding a solution, or at least
minimizing the problem.
Owing to the high costs of obesity, and the fact that the majority of these costs are financed
by the taxpayer, it is hardly surprising that the relationship between economic variables and
obesity has attracted so much academic attention in recent years.
5. 5
LITERATURE REVIEW
There have been plenty of theoretical and empirical studies on economic factors affecting
obesity rates but there have not been many studies based on econometric models. They have
been based more on case studies and quite often focusing on the US alone. This is probably
because the US currently has the highest obesity rates in the world. Since the late 1970s, the
number of obese adults in the US has grown by over 50%. A study by Chou et al. (2004) uses
micro-level data from the 1984- 99 Behavioural Risk Factor Surveillance System (BRFSS) to
discover which variables are most significant in explaining the rising trend in obesity. The
variables used are: per capita number of fast-food restaurants; per capita number of full-
service restaurants; price of a meal in each type of restaurant; price of food consumed at
home; price of cigarettes; clean indoor air laws; hours of work per week and hourly wage
rates by gender, race, years of formal schooling completed and marital status. They claim that
the growth in all types of restaurant is a response to increasing scarcity and value of
household or nonmarket time. This indicates there are positive effects of increased labour
market attachment on obesity levels. Rashad et al. (2006) also examined the effects of
relative prices on obesity.
The strong negative correlation over time between smoking rates and obesity has led some to
suggest that the reduction in smoking is increasing obesity levels. Chou et al. support this
conclusion by finding that higher cigarette prices have led to increased body weight.
However, Gruber & Frakes (2006) found no evidence to support this conclusion. They used
the cigarette tax instead of the cigarette price and found a negative effect of cigarette taxes on
body weight. Chou et al. used more variables in their analysis and therefore their conclusions
are more likely to be correct.
Schroder et al. (2007), conduct regression analysis to assess whether alcohol consumption
affects abdominal obesity. They find that high alcohol consumption (consuming more than 3
drinks per sitting) was significantly associated with the risk of abdominal obesity. However,
Kleiner et al. (2004) conducted a study of weight-management patients and found that as
BMI increased, rates of alcohol consumption decreased. This is owing to the theory that
overeating may be a substitute for alcohol for „brain reward sites‟, meaning food addiction
can be replaced by alcohol addiction and vice versa, which results in a negative correlation
between alcohol consumption and obesity.
6. 6
Much of the economic literature has focused on what has upset the balance between energy
intake and energy expenditure in recent decades. Finkelstein et al. (2005) reported that
technological advancement is the factor primarily responsible for the obesity epidemic. They
also report that lower food prices are also a contributing factor. From the law of demand, a
decrease in the price of food will cause consumption to increase. Ceteris paribus, if the price
of calorie-dense foods falls faster than the price of less calorie-dense foods, e.g. vegetables,
then individuals will shift their consumption to the cheaper alternatives. Finkelstein et al.
used primary historical material to demonstrate the changing patterns of obesity over the last
few decades. Because the majority of the population were more likely to suffer from weight
deficits in the past, increased BMI was typically associated with better health. This was the
case until obesity rates began to soar and so identifying economic factors that changed around
this time may help identify underlying causes of obesity.
Philipson & Lakdawalla (2002) argued that technological advancement is responsible for the
obesity epidemic largely because of its minimizing effect on energy expenditure in the
workplace. They found that 40% of the rise in obesity was due to expansion in the supply of
food through agricultural innovation, which lowered food prices, whereas 60% was due to
demand factors through more sedentary lifestyles. Exercise from household work has also
been reduced due to labour-saving machines, e.g. vacuum cleaners. Overall physical activity
has declined because the rise in recreational exercising does not compensate for the loss in
work-related exercise.
There is an abundance of literature relating to the impact of television viewing on obesity in
children and adolescents. However, there is less literature on the subject regarding adults. The
reason for television viewing affecting obesity is partially due to its potential as a stimulus for
eating. Gore et al. (2003) found that snacking, but not necessarily eating whole meals,
increased while watching television and the resulting overall caloric intake rose. However,
Lincoln (1972) performed a questionnaire study of food and beverage intake among 867 men
in the US and failed to find a direct relationship between overeating and obesity.
Tucker & Friedman (1989) studied 6138 adult males and found that those who viewed
television for more than three hours a day were twice as likely to be obese as those who
viewed less than one hour of television a day. They adjusted for age, smoking status, length
of working week, measured physical fitness and reported weekly hours of exercise. Physical
fitness confused the relationship between TV viewing and obesity but all the other variables
7. 7
behaved as expected. There have been no studies on the impacts of television viewing on
female adults. Physical activity has been shown to be a relevant factor contributing towards
obesity rates. Frank et al (2004) collected data from a travel survey in Georgia and found that
each additional kilometre walked per day was associated with a 4.8% reduction in the
likelihood of obesity.
Hinde & Dixon (2005) examine the impacts of car reliance in Australia on obesity levels.
They put emphasis on the social trends and processes behind the increasing reliance on
driving and the obesity epidemic.
Young & Nestle (2002) found evidence that portion sizes of nearly all food eaten outside the
home in the US have increased over time. Neilsen & Popkin (2003) found that the largest
increases were in French fries and sweetened beverages. However, there has been little
evidence relating to European countries of increased portion sizes. Neilsen and Popkin also
found that the increase in energy intake has been accompanied by changes in eating patterns;
snacking has become more popular over time.
There have been quite a few studies that try to link income and education to obesity rates on
an individual country level, but there has been little study of obesity rates across countries.
Wardle et al. (2002) investigated socioeconomic predictors of obesity in men and women.
Data from the 1996 Health Survey for England were used to compare ratios for obesity by
education, occupation while controlling for age, marital status and ethnicity. It was found that
obesity risk was greater among men and women with fewer years of education and poorer
economic circumstances, and of women, but not men, of lower occupational status. More
educated people are more knowledgeable about dieting. They are also more likely to be able
to afford the foods and programmes that supplement dieting. Nayga (2000) also found the
effects of increased schooling on obesity are due to increased health knowledge.
Eleuteri (2004) uses panel data to analyse obesity and income within the OECD. The paper
analyses the relationship between calorie intake, health spending, the percentage of the
population over 65 and obesity. The analysis shows that caloric intake is not the cause of
increased obesity in OECD countries. The results show that income has a positive impact on
obesity rates. In contrast, Cutler et al. (2003) run regressions using OECD countries data and
find that real income is unrelated to obesity.
8. 8
Poverty is associated with lower food expenditures, lower fruit and vegetable consumption
and lower quality diets. One aspect of poverty is limited access to physical activity. Lower
income areas have fewer supermarkets selling fresh fruit and vegetables and have fewer parks
and playing fields for exercise. Rashad (2003) finds that across countries, more developed
nations have higher obesity rates, in other words GDP per capita and obesity rates are
positively correlated. However, within a country, those with higher incomes tend to have
lower rates of obesity. Incomes on a global level have risen in the past two decades which is
contradictory to the inverse relationship between income and obesity found by many
researchers.
Engel‟s Law states that, as incomes rise, the share of income spent on food decreases. (Engel,
1857). People in higher income nations consume more added sugars and fats than people in
lower income nations. Conversely, Drewnowski & Spectar (2004) and Drewnowski (2003)
find that the highest rates of obesity occur amongst populations with the highest poverty rates
and the least education. They find that there is an inverse relationship between energy density
(MJ/kg) and energy cost ($/MJ). This means that energy-dense foods, composed of refined
grains, added sugars and fats, are the cheapest option for the consumer. The lowering of
energy costs through technological advancement has been most rife for foods containing
added sugars and fat.
There has been research on whether obesity is a cause of unemployment but little work has
been done on whether unemployment contributes towards the likelihood of obesity. Ruhm
(2000) showed that obesity becomes more prevalent during macroeconomic upturns when
there is low unemployment because higher time costs lead to reductions in healthy activities
such as exercise.
Ewing et al. (2003) attributes part of the rise in obesity to the degree of urban sprawl. Urban
sprawl is defined as the process through which the spread of development across the
landscape far outpaces population growth. The urban sprawl variable can be used to measure
how conducive a city is to exercise. Vandegrift & Yoked (2004) use US state-level data from
the 1990s on obesity to show that states that increased the amount of developed land (holding
population constant) had higher obesity rates. Conversely, Eid et al. (2008) find no evidence
that urban sprawl causes obesity. They find that individuals, who are more likely to be obese,
choose to live in more sprawling neighbourhoods and argue that other studies have failed to
control for this factor.
9. 9
There is an abundance of literature on the causes of childhood obesity, which can sometimes
be linked to causes of adult obesity. Higher wages for women have led to a dramatic increase
in female labour force participation which could be one of the reasons for rising obesity rates
in children. Anderson et al. (2003) found evidence that increases in maternal employment
influenced the rise in childhood obesity; they suggest that children of working mothers eat
home-cooked meals less frequently. However, this increase in the female labour force
occurred long before the rise in obesity began, so it might not be an influential factor. Cutler
et al. (2003) find that female labour force participation rates are unrelated to adult obesity.
More research must be done in order to determine what percentage of males and females do
the majority of the household cooking.
In the non-economic literature, rises in obesity levels have been blamed on biological factors
like genetics and behavioural factors like addiction and time preference. The theory that there
is a large genetic component to obesity is refuted by Philipson (2001), who argues that,
although genetics may explain cross-sectional differences, it cannot explain a change over
time in the amount of obesity. Such a change would be much slower than observed if it were
a genetic phenomenon. An increase in the rate of time preference can cause a rise in obesity.
Time preference is defined as the rate at which people are willing to trade current utility for
future benefit. A high rate of time preference means people will be more likely to increase
their calorie intake now and forego exercise for future health benefits.
Bray & Popkin (1998) followed adolescents and adults in China and found that the increase
in dietary fat intake was significantly related to an increase in BMI. However, Willet (1998)
found that dietary fat intake does not seem to be the primary cause of high obesity rates.
Comparisons of obesity between rich and poor countries have been used to support a causal
association between dietary fat intake and body fat, but these are negated by stark differences
in physical activity and food availability.
Explanations for the rising obesity epidemic are still not yet fully understood. The literature
examines many factors which contribute to rising obesity but it is unclear which factors are
the most dominant in contributing to weight gain. In order to determine the best policies for
governments to combat the obesity epidemic, more research needs to be undertaken.
Econometric analysis would be the optimal method for determining the significance of the
variables.
10. 10
METHOD
The Model
OBg,c = a + bGDPc + cEDc + dUNEMPc + eFATc + fALCc + gCARc +….+µg,c
OB = obesity rate (% of total population)
g = m (male), f (female)
c = 1,2,…,N (country)
a = intercept
GDP = real GDP per head (measured in thousands of constant 2000 US$)
ED = secondary school enrolment (% net)
UNEMP = unemployment (% of total labour force)
FAT = daily fat supply, grams per head
ALC = alcohol consumption per head (litres of pure alcohol)
CAR = passenger cars per 1000 people
TV = television viewing time (hours per person)
SMO = smoking prevalence (% of population ages 15+)
BM = Big Mac Index ($)
BM2 = Big Mac Index relative to income ($)
µ = error term
Rationale for choosing variables
The dependent variables are male obesity and female obesity (% of the population). The
reason for distinguishing obesity by sex is to test whether there is a difference in the causes of
obesity in males and females. This could be useful in analysing the significance of economic
variables affecting obesity rates and to what extent biological factors must be considered.
The first independent variable is GDP per head measured in thousands of constant 2000 US$
(EarthTrends, 2011). Figures for GDP are converted from domestic currencies into dollars,
using 2000 official exchange rates. Constant figures are adjusted for inflation, so that the
countries can be compared with each other, despite the fact that the figures are for different
11. 11
years. The reason for including GDP is because the amount of wealth and disposable income
people have will affect their consumption and lifestyle choices, which influence a person‟s
weight.
The next independent variable is secondary school enrolment (% net)1
(World Bank, 2011).
The reason for including this is because education influences health and dietary knowledge.
The general consensus is that the more educated people are, the less likely they are to eat
unhealthy foods and become obese.
Unemployment as a percentage of the total labour force2
(World Bank, 2011) has been
included for a number of reasons. Unemployment can have psychological effects, including
anxiety and depression. Often, one of the side-effects of anxiety or depression is an increase
in calorie consumption. Unemployment can also suggest very low income, especially if one is
living on the „dole‟. Some argue that low income leads to eating more fattening foods, as they
cost less to purchase. However, others argue that low income leads to less overall calorie
consumption and hence a smaller risk of obesity.
Daily fat supply per head measured in grams (FAOSTAT, 2011) has been included owing to
the well-known fact that consumption of fatty foods has a direct positive effect on peoples
weight.
The next independent variable is recorded adult (15+ years) alcohol consumption per head
(WHO, 2011), measured in litres of pure alcohol. Alcohol is a highly calorific substance,
which can contribute to weight gain.
The number of passenger cars3
per 1000 people (World Bank, 2011) has been included
because studies have shown that increased exercise decreases the risk of obesity and the more
that people use motor vehicles to transport themselves instead of walking, the less exercise
they will get.
1
The net enrolment ratio is the ratio of children of official school age, based on the International Standard
Classification of Education 1997, who are enrolled in school to the population of corresponding official school
age. Secondary education completes the provision of basic education that began at the primary level, and aims
at laying the foundations for lifelong learning and human development, by offering more subject or skill-
orientated instruction using more specialized teachers (World Bank, 2011).
2
This measures the percentage of the total labour force that is without work but is available for and seeking
employment (World Bank, 2011).
3
Passenger cars refers to road motor vehicles, other than two-wheelers, intended for the carriage of
passengers and designed to seat no more than nine people (including the driver) (World Bank, 2011).
12. 12
Television viewing time (IP Network, 2011) has been included because the more hours of
television watched per person per day, the more sedentary their lifestyle and hence the greater
the likelihood of being obese.
Smoking prevalence in adults (WHO, 2011) has been included because people often
substitute food for smoking and vice versa. Obesity rates and cigarette consumption have
been known to have a negative correlation.
The Big Mac Index provides a variable for fast-food prices. It is an index of PPP exchange
rates based solely on the prices of the Big Mac Sandwich in McDonald‟s restaurants around
the world. It is published by The Economist once a year. The Big Mac Index has been
included as it is an approximate measure of relative food costs in different countries.
Countries with lower indexes have a higher obesity rate than countries with high indexes.
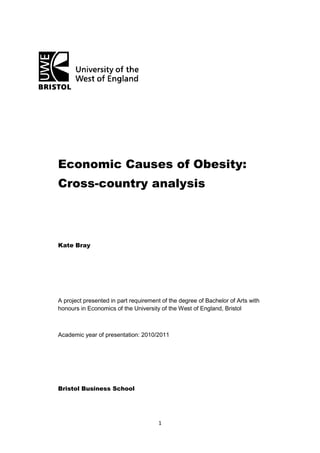
Graph 1a. Scatter plot of male obesity versus real GDP per head
13. 13
Graph 1b. Scatter plot of female obesity versus real GDP per head
Data Collection
When collecting worldwide data from various internet sources, various problems may be
encountered. Data were collected mainly from the international agency, the World Bank. The
main problem during data collection for this model was that nearly all of the data sets were
incomplete or not available for the specific years needed for this model. The success of any
econometric analysis relies on the availability of appropriate data. Owing to the
nonexperimental nature of the data used in this analysis, there was no choice but to depend on
the available data. Therefore, the results from this research can only be as good as the quality
of the data.
Television viewing time per person and smoking prevalence data were not available for
countries worldwide, only for European countries. Therefore, a regression is run for 53
countries to investigate the relationship between obesity and income. Another regression
14. 14
follows, which is restricted to 20 countries; this includes all of the variables except for
smoking and TV viewing. The next regression includes all of the variables but is restricted to
even fewer countries (20), as a result of only European data being available.
Regression
Regression measures the strength of the relationship between one dependent variable and a
series of other changing variables. Regressions are assumed to measure causal relationships
whereas correlations don‟t presume any causality. They merely measure whether two
variables tend to vary in a systematic linear fashion with each other.
In Table 1 are the regression results from exploring the relationship between obesity rates and
GDP (income). The intercepts have been excluded from the tables because they are not of
direct concern. Model (1) checks for a linear monotonic relationship; monotonic meaning
always rising or falling, but never both (as with a parabola). Model (2) has a dummy variable
to control for the outlier, Samoa. The outliers can be seen clearly from the scatter plots in
graphs 1a and 1b. Model (3) includes the logarithm of GDP (LNGDP). This is to check for a
monotonic relationship exhibiting diminishing returns. The gradient of the fitted relationship
between income and obesity is measured by multiplying the coefficient of LNGDP by the
derivative of LNGDP (=1/GDP). Models (4) and (5) have dummy variables for the outliers
USA and Luxembourg. Luxembourg is an outlier because of its very high GDP per head; it
does not have an unusual obesity rate.
To make the coefficients of GDP more manageable to work with, GDP was divided by 1000,
so that it measures income in thousands of constant US $.
17. 17
REGRESSION ANALYSIS
R² is the proportion of variation in the dependent variable explained by the regression model.
The values of R² range from 0 to 1. Small values indicate that the model does not fit the data
well. In Tables 1a and 1b, the values of R² increase as each independent variable is added.
For both male and female obesity, model (5) has the best R² and adjusted R². The model for
males fits the obesity data slightly better than does the model for females. It is quite rare to
get a high R² value in cross-country studies in the social sciences. This may be due to the
individual characteristics of different countries, many omitted factors, poor data etc.
A variable for GDP² was added to try to see if the data would fit a parabola but this was
unsuccessful. This suggests that the relationship between income and obesity is linear. If the
data fitted a parabola, this would mean that income and obesity would be positively related
but at a certain level of income, there would be a turning point and they would become
negatively related.
The negative coefficients show an inverse relationship between income and obesity. This is
rather surprising because there have been various studies (Vandegrift & Yoked, 2003), which
have shown large increases in obesity at the same time as rising incomes and economic
growth.
If Obesity = a + bGDP + cLNGDP, the partial derivative of Obesity with regard to GDP is
b+c/GDP, which varies with GDP. By interpreting the combined derivative, we can see the
relationship between Obesity and GDP.
The gradient for low-income countries is positive and that for high-income countries is
negative. This means in low-income countries, the richer the person, the more likely he or she
is to be obese, and in high-income countries, the richer the person, the less likely he or she is
to be obese. This is consistent with the findings of Rashad (2003), as mentioned in the
literature review. From the original data, for example, the gradients for Zimbabwe are +16.76
for males and +14.19 for females and those for Switzerland are -0.4333 for males and -0.622
for females. This is consistent with the theory because Zimbabwe has very low GDP, whereas
Switzerland has very high GDP.
The turning point at which the gradient changes from positive to negative is GDP = 11.447
for males and GDP = 7.927 for females. In countries with a GDP lower than 7.927, the higher
the GDP, the higher the obesity rate for both males and females. In countries with a GDP
18. 18
between 7.927 and 11.447, female obesity will fall as GDP increases but male obesity will
continue to rise. In countries with a GDP greater than 11.447, both male and female obesity
rates will fall as GDP rises.
One important assumption of the linear regression model is that the variance of the error term
is a constant σ². This is the assumption of homoscedasticity, or equal variance. Increasing
heteroscedasticity could occur because of greater variation in obesity in richer countries than
in poorer countries. Alternatively, there may be better data on obesity in richer countries,
which would cause decreasing heteroscedasticity. To test for heteroscedasticity, the squared
residuals are regressed on the squared fitted values. If the null hypothesis of homoscedasticity
is true, the coefficient will be close to zero (Flegg, 2004). The coefficients for males and
females, respectively, are -0.016 and -0.012. Neither of these values is significant, which
means that there is no problem of heteroscedasticity in the model.
The presence of outliers causes a lack of normality, shown by large residuals. The error term,
µ, represents the influence on the dependent variable of a large number of independent
variables that are not individually included in the model. It is hoped that the influence of
these omitted variables is small and random (Gujarati, 2004, p.109). To account for the
outliers, dummy variables have been included in the model. If outliers are present, the results
can be skewed.
To test for normality, we can look at histograms of the residuals in Graphs 2a and 2b. A
histogram of the residuals allows us to visually assess the assumption that the errors in the
dependent variable are normally distributed.
20. 20
Graph 2b. Histogram of residuals (female obesity)
The histogram of residuals for male obesity in Graph 2a follows the normal curve more or
less but it shows an outlier. A symmetric bell-shaped histogram which is evenly distributed
around zero indicates that the normality assumption is likely to be true (Gujarati, 2004,
p.147). In both histograms, the residuals are positively skewed. This suggests that the
model‟s underlying assumptions might have been violated.
To further check that the data are normally distributed, we can look at the Shapiro-Wilk
statistic. This is 0.958 for male obesity and 0.897 for female obesity. Both these figures are
significant at the 5% level; hence the residuals are normally distributed, so the t-ratios can be
trusted.
The “residuals” are defined as the differences between the observed (actual) values of obesity
and the predicted values. Because the Shapiro-Wilk test indicated a normal distribution, the
histograms might be skewed due to the outliers present.
21. 21
Graph 3a below shows actual versus predicted values for the initial model (1). This shows
that the initial model is extremely bad at predicting the actual male obesity rate.
Graph 3a. Scatterplot of actual vs. predicted values for model (1).
Graph 3b below shows actual versus predicted values for the refined model (5). This shows
the predictors used in this refined regression yield fairly good estimates of the actual obesity
levels.
23. 23
LINEAR REGRESSION MODEL
This uses data for 20 countries: Bulgaria, Croatia, Estonia, Finland, France, Greece, Hungary,
Italy, Lithuania, Luxembourg, Malta, Netherlands, Norway, Sweden, Switzerland, UK,
Japan, Brazil, Mexico and USA.
There are 8 independent variables (regressors): GDP, Secondary school enrolment,
unemployment, daily fat supply, alcohol consumption, passenger cars, Big Mac Index and
relative Big Mac Index (2).
Descriptive Statistics
Table 2a shows the correlation between the 2 dependent variables (male obesity and female
obesity) and the 8 independent variables.
Table 2a.Correlation Coefficients
Male obesity Female obesity
GDP -0.110 -0.175
LNGDP -0.104 -0.241
Secondary school enrolment -0.303 -0.472
Unemployment 0.045 0.001
Daily Fat supply 0.147 -0.008
Alcohol 0.097 0.081
Passenger cars -0.074 -0.325
Big Mac Index -0.124 -0.256
Big Mac Index (2) 0.074 0.246
Correlation is a statistical technique that measures the degree of linear association between
two variables. The correlation coefficient measures this strength of association. Correlation is
different from regression analysis, in which we try to estimate the average value of one
variable on the basis of the fixed values of other variables. N.B. Correlation suffers from
ceteris non paribus.
In regression analysis, there is an asymmetry between the dependent and independent
variables. The dependent variable is assumed to be statistical and random and to have a
probability distribution. The independent variables are assumed to have fixed values. In
correlation analysis, any two variables are symmetrical; there is no distinction between the
two variables and they are both assumed to be random. A random variable is a variable that
can take on any set of values, positive or negative, with a given probability (Gujarati, 2004,
p.23).
24. 24
CORRELATION ANALYSIS
The correlation between obesity and GDP for males is -0.11 and, for females, is -0.175. This
is as expected in rich countries, which have an inverse relationship between obesity and GDP,
but in poor countries there would be a positive correlation.
The correlation between obesity and secondary school enrolment for males is -0.303 and, for
females, is -0.472. This is negative as expected because, as education enrolment increases,
obesity should decrease owing to improved dietary knowledge.
The correlation between obesity and unemployment for males is 0.045 and for females is
0.001. This very low positive correlation is unexpected. As mentioned in the literature
review, according to Ruhm (2000), a negative correlation would be expected, as unemployed
people have lower time costs, so are able to take part in more physical activities. When a
correlation is unexpected, this is a case of ceteris non paribus. This problem is addressed in
regression analysis.
The correlation between obesity and daily fat supply for males is 0.147 and for females is
-0.008. The male correlation is positive, as expected. A study mentioned in the literature
review (Willet, 1998), argues that there is very weak positive relationship between dietary fat
and body fat. The female correlation is very slightly negative, which is unexpected.
The correlation between obesity and alcohol consumption for males is 0.097 and for females
is 0.081. This is slightly positive, as expected, owing to the high calorie content of alcohol
(Schroder et al. 2007). However, according to Kleiner et al. (2004), this would be as expected
owing to alcohol addiction being a substitute to obesity (food addiction) in individuals.
The correlation between obesity and passenger cars for males is -0.074 and for females is
-0.325. These negative correlations are surprising because cars are a labour-saving good and
the less walking people do, the higher the obesity rate should be. This negative correlation
could be explained by collinearity between GDP and passenger cars, which have a correlation
of 0.649.
The correlation between obesity and the relative Big Mac Index (2) is 0.074 for males and for
females it is 0.246. This is not as expected because the higher the relative price of a Big Mac
is, the lower the consumption of „fast-food‟ expected and hence the lower rate of obesity
expected.
25. 25
Table 2b. Correlation Matrix
GDP1000
Secondary
school
enrolment (%
net)
Unemployment
(% of total
labour force)
Daily fat supply
(g) per capita
Alcohol
Consumption
Passenger
cars per 1000
people Big Mac Index
GDP Pearson Correlation
Sig. (2-tailed)
N 20
Secondary school
enrolment (% net)
Pearson Correlation .320
Sig. (2-tailed) .170
N 20 20
Unemployment (% of total
labour force)
Pearson Correlation -.586
**
.003
Sig. (2-tailed) .007 .989
N 20 20 20
Daily fat supply (g) per
capita
Pearson Correlation .594
**
.187 -.367
Sig. (2-tailed) .006 .429 .111
N 20 20 20 20
Alcohol Consumption Pearson Correlation -.122 .254 .287 .136
Sig. (2-tailed) .608 .280 .220 .566
N 20 20 20 20 20
Passenger cars per 1000
people
Pearson Correlation .649
**
.530
*
-.303 .575
**
.165
Sig. (2-tailed) .002 .016 .194 .008 .488
N 20 20 20 20 20 20
Big Mac Index Pearson Correlation .694
**
.420 -.482
*
.673
**
-.160 .619
**
Sig. (2-tailed) .001 .065 .031 .001 .502 .004
N 20 20 20 20 20 20 20
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
26. 26
Table 2b above shows how strongly correlated the variables are with each other. This helps
us to determine whether there are any problems of multicollinearity.
REGRESSION ANALYSIS
Multicollinearity is a problem with estimating the regression coefficients caused by
predictors that are linearly related with each other. The problem of multicollinearity can be
tested using the Variance Inflation Factor (VIF). VIF shows how the variance of a regressor
is inflated by the presence of multicollinearity. If VIF = 1, there is no collinearity. As a
general rule of thumb, if the VIF > 10, which will happen if R² exceeds 0.90, there is likely
to be a high degree of multicollinearity and there should be a cause for concern. Studenmund
(5th
ed, p.259) mentions a rule of thumb of VIF > 5, which is considered to be a very
conservative rule and is much less commonly used. Tolerance (TOL) can also be used as a
measure of multicollinearity as it is the reciprocal of VIF. If TOL<1, there could be
multicollinearity present. For var1, we would regress it on var2,3,4 etc. and get R². TOL(1) =
1 - R² and VIF(1) = 1/TOL(1). However, VIF (or TOL) is not a perfect measure of
multicollinearity. A high VIF is neither necessary nor sufficient to get high variances and
high standard errors. Therefore, a high degree of multicollinearity may not necessarily cause
high standard errors (Gujarati, 2004, p.326).
27. 27
Table 3. Collinearity Statistics
Model
Collinearity Statistics
Tolerance VIF
1 (Constant)
GDP .158 6.348
Secondary school enrolment
(% net)
.303 3.304
Unemployment (% of total
labour force)
.541 1.849
Daily fat supply (g) per capita .338 2.963
Alcohol Consumption .569 1.757
Passenger cars per 1000
people
.307 3.259
Big Mac Index .224 4.471
DUMUS .483 2.069
DUMLUX .281 3.555
The VIF and TOL figures in Table 3 give no cause for concern as the VIF‟s are all less than
10. However, according to Studenmund, the VIF of GDP (6.348) could be a cause for
concern as it is > 5. The figures suggests that a certain degree of multicollinearity is present
(VIF>1), but not a serious problem. Some variables are more affected by others. GDP has the
highest VIF (6.348). GDP could be affected by unemployment because the higher the
unemployment rate, the lower the GDP will be. Secondary school enrolment could also affect
GDP because the more educated the work force, the higher the GDP is likely to be. The Big
Mac Index has the second highest VIF (4.471). The Big Mac Index also has a positive
correlation of 0.694 with GDP, significant at the 0.01 level; this means the higher the prices
of Big Macs are in a certain country, the higher GDP is likely to be.
30. 30
The t-ratio for unemployment in model (2) is very low which means the variable is not
statistically significant. By excluding the unemployment variable, the model does not
improve and so it is kept in the model on the basis that unemployment is a relevant variable.
Model (2) in Table 4a. is considered to be the preferred model, as it has a better fit (higher
R²). The following analysis will be based on model (2).
GDP and LNGDP must be interpreted together to determine the relationship between Obesity
and GDP. The gradient of the curve of obesity versus GDP in Bulgaria (the lowest income
country in the model) is 14.222 for males and 15.812 for females. In Luxembourg, (the
highest income country in the model), the gradient for males is -1.109 and for females it is
1.328, cet. par. In Bulgaria, there is a positive relationship between income and obesity for
both males and females, and in Luxembourg there is an inverse relationship between income
and obesity, for males but a positive relationship for females, cet. par. This supports the
theory mentioned previously, that the gradient of the curve is positive to a certain level of
GDP, and then it will become negative. The turning point at which the overall gradient
changes from positive to negative is GDP = 18.278 for males and GDP = 20.724 for females.
Luxembourg‟s GDP is 51.59 and the female gradient is still slightly positive at this level.
This shows that Luxembourg women do not follow the trend.
For every percentage point increase in secondary school enrolment, there is a decline in male
obesity of 0.062 percentage points and for female obesity there is a decline of 0.152
percentage points, cet. par. The higher effect in females might suggest that males choose to
pay less attention to dietary advice provided by schools and are more likely to ignore the
health risks associated with obesity.
For every percentage point increase in unemployment, there is a decline in male obesity of
0.023 percentage points and for female obesity there is a decline of 0.407 percentage points,
cet. par. The higher effect in females may be explained if females spend more of their free
time exercising than males do.
For every 1g increase in fat supply, there is a decline in male obesity of 0.013 percentage
points and for female obesity there is a decline of 0.069 percentage points, cet. par. For every
1 litre increase in alcohol consumption, there is an increase in male obesity of 0.181
percentage points and an increase in female obesity of 0.491 percentage points, cet. par. This
may be explained if females drink alcoholic drinks that are more fattening than those drunk
by males.
31. 31
For each additional car per 1000 people, there is an increase in male obesity of 0.004
percentage points, and for females there is a decrease of 0.036 percentage points, cet. par.
For every dollar increase in the Big Mac Index, there is a rise in male obesity of 3.910
percentage points, and for females there is a rise of 5.049 percentage points, cet. par. This is
not the expected outcome, as it is logical that more expensive „fast-food‟ would encourage
people to eat more healthy food and hence the obesity rate would fall, cet. par. The model
does not include any variable for physical activity, which has been shown to be a significant
determinant of obesity rates (Frank et al. 2004; Lincoln 1972). The reason for not including
physical activity as a regressor is because the relevant data for all countries in the model were
not available.
In model (2), the Big Mac Index has been divided by GDP, to create a relative price variable,
BM2. This improved the explanatory power of the model (R² is higher) but the coefficient of
BM2 is unrealistic. BM2 has a slightly higher t-ratio than the original Big Mac Index, but it is
still not significant at conventional levels. A one-unit increase in BM2 would mean an
increase in male obesity of 42.395 percentage points, cet. par. This is unrealistic; a rise of
say, 0.1 units, would be more meaningful. The Big Mac Index in Japan (2004) was 2.33 and
the BM2 was 0.06. This shows that the Big Mac Index was less than average (the average Big
Mac Index in this model is 3.05), and combining this with a very high GDP of 38.2, means
that the BM2 figure is the smallest of all countries in the model. This suggests the Japanese
could consume large quantities of fast-food with very little cost. However, the Japanese
obesity rates are the lowest in the developed world. This contradiction cannot be due to a lack
of availability of fast-food restaurants. According to Nationmaster.com, Japan has the second
highest number of McDonald‟s restaurants in the world, after the USA. 99% of Japanese are
enrolled in secondary education. This is the highest rate of all countries in the model, and
could help explain the lack of obesity is due to a good dietary education. This supports the
idea of Steven E. Landsburg who argues that McDonald‟s cannot be blamed for the obesity
epidemic (Landsburg, 2007, p.138). The Big Mac Index in Bulgaria (2004) was 1.85 and the
BM2 was 0.94. This BM2 figure is the highest of all the countries in the model. This shows
that Big Macs in Bulgaria are relatively more expensive than anywhere else because Bulgaria
has a very low GDP of 1.97 (000‟s US$), but McDonald‟s have not adjusted their prices
according to GDP.
32. 32
MODEL 3 - PHYSICAL ACTIVITY
This uses 10 countries‟ data and 7 independent variables.
Physical activity has been found to be a very significant factor affecting obesity rates. For the
countries in this study, physical activity data were only available for 10 countries, so a
smaller model has been created to see how significant it is for explaining obesity rates. The
physical activity figures are defined as the percentage of the population that partake in either
„moderate‟ or „high‟ activity, three or more days a week (Bauman et al. 2009).
The model does not include secondary school enrolment, television viewing or smoking
prevalence as there was not enough data available for the 10 specific countries.
33. 33
Table 5. Two Linear Regression Models (male and female)
Male Female
GDP 2.951
(2.050)
1.440
3.140
(1.918)
1.637
LNGDP -54.940
(31.801)
-1.728
-58.286
(29.761)
-1.958
UNEMP 3.878
(8.908)
0.435
3.101
(8.336)
0.372
FAT 0.074
(0.341)
0.217
-0.008
(0.319)
-0.024
ALCO 0.110
(1.295)
0.085
0.375
(1.212)
0.310
CAR 0.125
(0.098)
1.277
0.103
(0.091)
1.132
BM2 -35.212
(88.211)
-0.399
-57.690
(82.551)
-0.699
PA 0.241
(0.906)
0.266
0.538
(0.848)
0.635
R² 0.943 0.952
Adjusted R² 0.489 0.565
Note: standard errors are in parentheses and t-ratios are in bold.
The R² for both male and female obesity is very high, 0.943 and 0.952, respectively. This
suggests that physical activity is a crucial variable to include when trying to explain variance
in obesity rates. For every percentage point increase in the male population taking part in
physical activity, there is an increase in male obesity of 0.241 percentage points, cet. par. By
contrast, for every percentage point increase in the female population taking part in physical
activity, there is an increase in female obesity of 0.538 percentage points, cet. par.
34. 34
CASE STUDIES
Case Study: Canada and US comparison
From the original data, it can be seen that for men, the prevalence of obesity was 9.3
percentage points lower in Canada than in the United States (22.9% compared with 32.3%)
and for women, 12.3 percentage points lower (23.2% compared with 35.5%).
Given the similarities between Canada and the US, it is difficult to see what major cultural or
lifestyle differences could account for such a difference. One major difference is the per
capita GDP. The differences in standard of living as captured by GDP may affect the
resources available for food consumption. However, the relationship between income, food
consumption and obesity may not necessarily be positive, as it would also depend on whether
food is a normal or inferior good. Furthermore, income and education are also correlated
(0.320). This positive correlation shows that countries with higher incomes tend to have
better educated populations and therefore their populations are more knowledgeable about
health and food consumption, meaning the relationship between obesity and income could be
negative rather than positive or it could be non-linear, i.e. a parabola.
Different ethnic groups seem to be an important consideration when measuring obesity rates.
Flegal et al. (2002) found that differences in ethnic groups did not vary significantly in the
prevalence of obesity for men, but for women, it was found that the prevalence of obesity was
highest for non-Hispanic black women.
A recent study of data collected between 2007-2009 by the Centers for Disease Control
(CDC), has shown that more than a third of the US population are obese, compared with
about a quarter of the Canadian population. The CDC attributed part of the difference in
obesity to the larger percentage of Black and Hispanic people in the US. These demographics
are shown to be more prone to obesity. This is backed up by Flegal et al. (2002), who cite
ethnicity as a variable affecting obesity rates. When comparing the white populations in the
US and Canada, 25.6% of Canadians and 33% of Americans were obese, whereas over the
whole of the populations, the figures have a wider spread of 24.1% and 34.4% respectively.
Case Study: Japan
The Japanese have the lowest obesity rates in the Developed World (3.4% of males and 3.8%
of females are obese). From the data, it can be seen that the percentage of the population
35. 35
enrolled in secondary school is the highest in all countries (99%). This suggests that obesity
is very low among the well-educated.
According to the study by Bauman et al. (2009), Japan reported less than a third of their
population taking part in „high‟ physical activity. This could suggest that physical activity is
an irrelevant variable for a model trying to explain obesity. 43.3% of Japanese people are
classified as „inactive‟. This is the highest rate in the physical activity model of 10 countries,
as discussed previously. This statistic is very surprising as a low obesity rate would be
expected to be associated with high activity levels. However, this physical activity measure
does not account for everyday exercise. The Japanese have very good public transport
services and tend to walk around more in their day-to-day lives rather than use cars.
The Japanese have a very unique diet, consisting predominantly of fish. Sakata (1995) found
that a conventional Japanese diet consisting mainly from chicken fillet, egg white, fish,
mushroom, seaweed and low-calorie vegetables, has been shown to be useful for keeping a
healthy weight.
However, Asians are particularly susceptible to the health risks associated with excess body
fat and so the Japanese have redefined obesity as BMI > 25 (Anuurad et al. 2003). This has
not been accounted for in the obesity data used in this study.
Case Study: Samoan Women
From the original data, it can be seen that 63% of Samoan women and 32.9% of Samoan men
were obese in 1995. The reasons for such high obesity rates, especially in females, are mainly
owing to modernisation and biological factors. The significantly higher rate in females could
be associated with significant reductions in their specific subsistence activities in modern
settings.
According to Pawson & Janes (1981), peoples of the Pacific Islands tend to become
overweight when they migrate or are exposed to modernization. They conducted a survey of
height, weight, blood pressure and fasting plasma glucose (FPG) among an urbanized
Samoan community in the San Francisco Bay Area, to try to determine the reason behind the
high obesity rate in migrant Samoans. Although the participants‟ average height fell between
the 25th
and 50th
percentile of the US population, about one half of the sample exceeded the
95th
percentile for weight. They concluded that it was difficult to comment on the results they
produced because they were unsure whether the sample population used was in some way a
36. 36
“selected” group of Samoans, becoming fat before they migrate. They also comment that the
cultural beliefs are currently unknown but may be important in determining the Samoan‟s
attitudes toward food and obesity. Baker (1982) supports Pawson & Janes‟ study as he argues
that Samoans suffer large weight gain when they migrate to Hawaii and San Francisco, or
live a relatively affluent life in American Samoa.
Another reason why Samoans might be unusually fat is because of their lifestyle and
surroundings. Their staple diet consists of coconut, taro root, breadfruit, pig and fish, which is
native on the island. The Samoans need to do very little work to maximise the production of
these foods. Due to low work requirements in traditional Samoan society, levels of physical
fitness are proportionately low.
McGarvey (1991) takes an evolutionary perspective on Polynesian obesity, based on
scenarios of the fates of sailors on the voyages of discovery and of settlers in the pioneer
island villages. Their biological characteristics allowed them to rapidly grow adipose-tissue
which might have increased their chances of survival. According to Baker (1982), who
supports this view, Samoans, along with many other Pacific populations, seem to have
undergone a natural selection which favoured those who could rapidly gain weight.
Combining sudden diet and physical activity changes from modernization with such genetic
predispositions might be a cause of the high levels of obesity we see today.
Hodge et al. (1994) conducted a follow-up survey to a survey conducted in 1978, which
showed large differences in the prevalence of obesity between rural and urban populations in
Western Samoa. Cross-sectional differences in the prevalence of obesity, mean BMI and
waist-hip circumference ratio (WHR) were examined after adjusting for age, in urban Apia
and rural Poutasi and Tuasivi. Increased physical activity in men was associated with lower
obesity rates but this was not the case with women. Increased education and job status in
males were associated with increased obesity levels. This might be explained by the culture
of being overweight equating to status and success, which was not so important for females at
the time. However, increasing equality between sexes continues to grow and this could help
explain the very high prevalence of obesity in females.
37. 37
EVALUATION
One fundamental flaw of the study is that BMI is based on weight and so very muscular
people, e.g. sportsmen, might have BMI values which suggest they are overweight or obese
but of course they are not. BMI can be a good measure of total body fat, but it cannot
distinguish between different types of fat distribution. For example, someone with excess fat
in the region of the stomach is more at risk of serious medical conditions such as heart
disease, raised blood pressure and diabetes; whereas someone with fat under the skin, and in
the hip and thigh regions are at risk of medical conditions which are less serious. To sidestep
this problem with BMI measurement, some sort of measurement involving a waist-height
ratio could be used instead (Ashwell, 2011).
The models could be improved by having data for all countries in the same year. The
investigation could be expanded by using more independent variables to try to explain the
causes of obesity. Urbanization could be included as an independent variable as various
studies suggest the prevalence of obesity may be higher in rural than in urban settings.
Technological advancement could also be included as an independent variable; after reading
numerous journals, it is evident that technology has played a crucial role in the change in
obesity rates.
Eating processed or fast food that is high in fat has been shown to be one of the main causes
of obesity. Primary research could be taken to measure the availability of fast food
restaurants compared with „sit down‟ restaurants in different countries. Data for the number
of McDonald‟s restaurants per capita would be helpful, but unfortunately after emailing their
headquarters, this information could not be obtained.
Snacking and comfort eating can also contribute towards obesity rates. This could be
measured by collecting primary data on people‟s mental health. However, this would be a
very time-consuming process and not everybody „comfort eats‟ when they find themselves in
a bad mental state. Dallman et al. (2003) propose people eat comfort food in an attempt to
reduce the activity in the chronic stress-response network of the brain. Mental health remains
a grey area when it comes to data collection and so more work must be done to discover the
association between obesity and mental health problems.
From surveying the literature on obesity it is evident that childhood obesity is an increasingly
prevalent problem and therefore the model might be improved by controlling for age. This
38. 38
would give a clearer view of the relationship between childhood and adult obesity rates. It has
been shown that obesity in children predicts obesity later in life (Deckelbaum & Williams,
2001).
The prevalence of obesity is supposed to increase with age so „population over 65‟ could be
included as an independent variable, as discussed in the literature review (Eleuteri, 2004).
From trying to research the cultural differences between the US and Canada for the first case
study, it was clear that there is a large knowledge gap on the cultural determinants of obesity.
To assess beliefs, expectations and perceptions in relation to body size and food will take
many further years, but it is a subject of great importance for future policy implementation.
It is impossible to include every relevant variable that may contribute towards weight gain as
there are infinite possibilities. These models have tried to narrow down the possibilities and
include what appears to be the most significant variables relating to obesity, having read the
surrounding literature.
The statistical software used in this study was IBM‟s SPSS. This software is adequate for
small-scale research but it has its limitations for more in-depth research. SPSS users have
limited control over the statistical output and would be better off choosing another package.
39. 39
CONCLUSION
From the first model, it was found that income and obesity do not follow a linear relationship.
It can be assumed that increasing incomes in countries will carry on increasing levels of
obesity worldwide, especially in lower income countries.
The second model then gives some hints as to what is contributing towards obesity and from
that, policymakers can try and form policies specific to the circumstances in individual
countries. The most significant factor affecting obesity for both males and females was found
to be GDP and the least significant factor for both males and females was the number of
passenger cars per 1000 people. „CAR‟ was found to be an insignificant variable owing to the
fact it was highly correlated with GDP. The final model included physical activity as an
independent variable which was found to be highly relevant, shown by the large R² value.
From the US and Canada case study, it is shown that ethnicity is an important factor in
explaining obesity rates for women (Flegal, 2002). The Samoan case study demonstrates that
modernization and biological factors are to blame for sky-high obesity rates. It can be
deduced that increased „westernization‟ in Samoa will most likely lead to increased levels of
obesity in the future. From the Japan case study it is shown that education and diet are the
most influential factors affecting obesity rates and these should be specifically targeted by
policymakers. These 3 case studies each have different reasons behind the obesity rates in the
different countries. This shows how complex the model could potentially become. Modelling
causes of obesity cross-country is near impossible using linear regression analysis as there are
too many inter-related determinants of obesity and each country‟s obesity rates will be
contextual.
Much more econometric work must be done on the causes of the rising obesity epidemic. It is
still not yet fully understood why general rises in income have failed to lower obesity rates on
a country level, despite a strong inverse relationship between obesity and income on an
individual level.
40. 40
ACKNOWLEDGEMENTS
The author wishes to acknowledge the contributions of Tony Flegg of the University of the
West of England, who supervised the statistical analysis of this dissertation.
REFERENCES
Anderson, PM. et al. (2003) 'Maternal employment and overweight children.' Journal of
Health Economics. 22. (3).477-504.
Anuurad, E. et al. (2003). „The new BMI criteria for Asians by the regional office for the
western pacific region of WHO are suitable for screening of overweight to prevent metabolic
syndrome in elder Japanese workers.‟ Journal of Occupational Health. 45. (6). 335-343.
Ashwell, M. (2011). „Body Mass Index – BMI – „misses obesity risks‟‟. BBC News.
Available at: www.bbc.co.uk/news/health-12481427. [Last accessed: 24/04/2011].
Baker, P. (1982). „Why do Samoans grow so fat?‟ New Scientist. 96. No.1334.592.
Bauman, A. et al. (2009). „The International Prevalence Study on Physical Activity: results
from 20 countries.‟ International Journal of Behavioural Nutrition and Physical Activity.
21. (6).
Bindon,J. & Baker, P. (1985). „Modernization, migration and obesity among Samoan
adults‟. Annals of Human Biology. 12. (1). 67-76.
Bray, G. & Popkin, B. (1998). „Dietary fat intake does affect obesity!‟. American Journal of
Clinical Nutrition. 68. 1157-73.
Chou, S. et al. (2004). „An economic analysis of adult obesity: results from the Behavioural
Risk Factor Surveillance System.‟ Journal of Health Economics. 23. 565-587.
Comuzzie, A.G. & Allison, D.B. (1998). 'The search for human obesity genes.' Science. 280.
1374-1377.
Cutler, D. et al. (2003). „Why Have Americans Become More Obese?‟ Journal of Economic
Perspectives. 17. (3). 93-118.
Dallman, M. et al. (2003). „Chronic stress and obesity: a new view of “comfort food”‟. PNAS.
100. (20). 11696-11701.
Deckelbaum, R. & Williams, C. (2001). „Childhood obesity: the health issue.‟ Obesity
Research. 9. (4). 239-243.
Drewnowski, A. (2003). „Fat and Sugar: An Economic Analysis‟. The Journal of Nutrition.
133. 8385-8405.
41. 41
Drewnowski, A. & Specter, S.E. (2004). „Poverty and obesity: the role of energy density and
energy costs.‟ The American Journal of Clinical Nutrition.79. (1). 6-16
EarthTrends. (2011). A. GDP, constant US dollars. Provided by the World Resources
Institute. Available at: earthtrends.wri.org/text/economics-
business/variable-220.html. [last accessed: 12/03/2011].
Eid, J. et al. (2008). „Fat City: questioning the relationship between urban sprawl and
obesity.’ Journal of Urban Economics. 63. (2). 385-404.
Eleuteri, B. (2004). „Income and Obesity in OECD Countries‟. Available at:
www.tcnj.edu/~business/economics/documents/eleuteri.tcnj.pdf. [Last accessed: 11/04/2011].
Ewing, R. et al. (2008). „Relationship between Urban Sprawl and Physical Activity, Obesity
and Morbidity.’ American Journal of Health Promotion. 18. 47-57.
Finkelstein, E. et al. (2005). 'Economic Causes and Consequences of Obesity.' Annual Review
of Public Health. 26. 239-257.
FAOSTAT. Food and Agriculture Organisation of the United Nations. (2011). „Fat supply
(g/daily/capita)‟. Available at:
faostat.fao.org/site/609/DesktopDefault.aspx?PageID=609#ancor. [Last accessed: 14/03/11].
Flegal, K.M. et al. (2002). „Prevalence and trends in obesity among US adults.‟ JAMA. 288.
1723-1727.
Frank, L. et al. (2004). „Obesity Relationships with Community Design, Physical Activity,
and Time Spent in Cars.‟ American Journal of Preventative Medicine. 27. (2). 87-96.
Gardner, G & Halweil, B. (2000). 'Underfed and overfed: the global epidemic of
malnutrition.' Worldwatch Institute, paper 150. Available at:
http://www.worldwatch.org/system/files/EWP150.pdf. [Last accessed: 13/04/2011].
Gore, S. et al. (2003). 'Television viewing and snacking.' Eating Behaviour. 4. 399-405.
Gruber, J. & Frakes, M. (2006). „Does falling smoking lead to rising obesity?‟. Journal of
Health Economics, 25 (2). 389-93.
Gujarati, D. (2004). Basic Econometrics. 4th
edition. McGraw-Hill.
Hinde, S. & Dixon, J. (2005). 'Changing the obesogenic environment: insights from a cultural
economy of car reliance.' Transportation Research. Part D. 10. 31-53.
Hodge, A.M. et al. (1994). „Dramatic increase in the prevalence of obesity in Western Samoa
over the 13 year period 1978-1991.‟ International Journal of Obesity. 18. (6). 419-428.
IP Network. (2011). „TV Viewing time per individual in 40 countries across the world
2000-2007.‟ Available at: www.ip-network.com/tvkeyfacts. [Last accessed: 11/03/2011].
42. 42
Kleiner, K. (2004). „Body Mass Index and Alcohol Use.‟ Journal of Addictive Diseases. 23.
(3). 105-118.
Lakdawalla, D. & Phlipson, T. (2002). 'The growth of obesity and technological change: a
theoretical and empirical examination.' Nat.Bur.Econ.Res.Work. Paper No. 8946. Cambridge
MA.
Landsburg, S.E. (2007). ‘More Sex is Safer Sex. The Unconventional Wisdom of Economics.’
Pocket Books. P.138.
Lincoln, J. (1972). „Calorie Intake, Obesity and Physical Activity.‟ American Journal of
Clinical Nutrition. 25. 390-394.
Martinez, J. et al. (1999). „Variables independently associated with self-reported obesity in
the European Union.‟ Public Health Nutrition. 2 (1a). 125-133.
Martorell, R. et al. (2000). „Obesity in women from developing countries.‟ European Journal
of Clinical Nutrition. 54. 247-252.
McGarvey, S. (1991). „Obesity in Samoans and a perspective on its etiology in Polynesians.‟
The American Journal of Clinical Nutrition. 53. 1586-1594.
McLaren, L. (2007). „Socioeconomic status and obesity‟. Epidemiological Reviews. 29. 29-
48.
Moriyama, N. & Doyle, W. (2005). Japanese Women Don’t Get Old or Fat. Random House.
Nayga, R.M. (2000). „Schooling, health knowledge and obesity‟. Applied Economics. 32 (7).
815-822.
Neilsen, S. & Popkin, B. (2003). 'Patterns and trends in food portion sizes, 1977-1998.'
JAMA. 289 (4). 450-453.
Offer, A. et al. (2010). „Obesity under affluence varies by welfare regimes: the effect of fast-
food, insecurity, and inequality.‟ Economics and Human Biology. 8. 297-308.
Pawson, I. & Janes, C. (1981). „Massive Obesity in a Migrant Samoan Population‟. American
Journal of Public Health. 71. (5). 508-513.
Philipson, T. (2001). „The World-wide growth in Obesity: An Economic Research Agenda’.
Health Economics. 10. 1-7.
Rashad, I. (2003). ‘Assessing the underlying economic causes and consequences of Obesity.’
Gender Issues. 21 (3) 17-29.
Rosin, O. (2008). „The Economic Causes of Obesity: a survey‟. Journal of Economic
Surveys. 22 (4).6167-647.
Ruhm, C.J. (2000). 'Are recessions good for your health?' Quarterly Journal of Economics.
115 (2). 617-650.
43. 43
Sakata, T. (1995). „A very-low-calorie conventional Japanese diet: its implications for
prevention of obesity.‟ PubMed. 3 (2). 233-239.
Schroder, H. et al. (2007). „Relationship of abdominal obesity with alcohol consumption at
population scale.‟ European Journal of Nutrition. 46. (7). 369-376.
Senauer, B. & Masahiko, G. (2006). „Is Obesity a result of faulty economic policies? The case
of the United States and Japan.‟ Available at: http://purl.umn.edu/25497. [Last accessed:
25/04/2011].
Studenmund, A.H. Using Econometrics: A Practical Guide. 5th
edition. Addison-Wesley.
The World Bank. (2011)
A. „School enrolment, secondary (% net).‟ Source: United Nations Educational,
Scientific and Cultural Organization (UNESCO) Institute for Statistics. Available at:
data.worldbank.org/indicator/SE.SEC.NENR. [Last accessed: 12/03/2011].
B. „Unemployment, total (% of total labour force).‟ Source: International Labour
Organization. Key indicators of the Labour Market database. Available at:
data.worldbank.org/indicator/SL.UEM.TOTL.ZS. [Last accessed: 14/03/2011].
C. „Passenger cars (per 1,000 people)‟. Source: International Road Federation, World
Road Statistics and data files. Available at:
data.worldbank.org/indicator/IS.VEH.PCAR.P3/countries. [Last accessed:
12/03/2011].
Tucker, L & Friedman, G,M. (1989). „Television Viewing and Obesity in Adult Males.’
American Journal of Public Health. 79. 516-518.
Vandegrift, D. & Yoked, T. (2004). „Obesity rates, income, and suburban sprawl: an analysis
of US states.‟ Health & Place. 10. 221-229.
Wardle, J. et al. (2002). „Sex Differences in the Association of Socioeconomic Status with
Obesity.‟ American Journal of Public Health. 92. (8). 1299-1304.
WHO. (2003). „Obesity and Overweight‟.
http://www.who.int/dietphysicalactivity/publications/facts/obesity/en/. Last accessed:
08/02/2011.
WHO. (2011).
A. Global Information System on Alcohol and Health (GISAH). „Recorded adult per
capita consumption, from 1961, Total.‟ Available at:
apps.who.int/ghodata/?theme=GISAH#. [last accessed: 14/03/11].
B. Tobacco Control Database. „Smoking prevalence in adults (%)‟. Available at:
data.euro.who.int/tobacco/Default.aspx?TabID=2444. [last accessed: 10/03/2011].
44. 44
Willett, W. (1998).
A. „Dietary fat and obesity: an unconvincing relation.‟ American Journal of Clinical
Nutrition. 68. 1149-50.
B. „Is dietary fat a major determinant of body fat?‟. American Journal of Clinical
Nutrition. 67. 556-562.
Websites
www.nationmaster.com/graph/foo_mcd_res-food-mcdonalds-restaurants. [Last accessed:
27/04/2011]. McDonald’s.
www.bigmacindex.org/index.html [Last accessed: 11/04/2011]. The Economist.
46. 46
MODEL 1
Regression
Model Summary
b
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .126
a
.016 -.003 10.3858
a. Predictors: (Constant), GDP1000
b. Dependent Variable: Female Obesity (% of total population)
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 89.088 1 89.088 .826 .368
a
Residual 5501.133 51 107.865
Total 5590.221 52
a. Predictors: (Constant), GDP1000
b. Dependent Variable: Female Obesity (% of total population)
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 19.982 1.867 10.702 .000
GDP1000 -.098 .108 -.126 -.909 .368
a. Dependent Variable: Female Obesity (% of total population)
47. 47
Residuals Statistics
a
Minimum Maximum Mean Std. Deviation N
Predicted Value 14.906 19.939 18.887 1.3089 53
Residual -16.4727 43.1302 .0000 10.2855 53
Std. Predicted Value -3.041 .804 .000 1.000 53
Std. Residual -1.586 4.153 .000 .990 53
a. Dependent Variable: Female Obesity (% of total population)
Regression
Variables Entered/Removed
Model Variables Entered Variables Removed Method
1 DumSamoa,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
b
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .599
a
.359 .333 8.4663
a. Predictors: (Constant), DumSamoa, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 2006.271 2 1003.136 13.995 .000
a
Residual 3583.949 50 71.679
Total 5590.221 52
a. Predictors: (Constant), DumSamoa, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
48. 48
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 18.606 1.545 12.042 .000
GDP1000 -.050 .089 -.064 -.565 .575
DumSamoa 44.451 8.595 .589 5.172 .000
a. Dependent Variable: Female Obesity (% of total population)
Residuals Statistics
a
Minimum Maximum Mean Std. Deviation N
Predicted Value 16.020 63.000 18.887 6.2115 53
Residual -15.1505 19.1837 .0000 8.3019 53
Std. Predicted Value -.462 7.102 .000 1.000 53
Std. Residual -1.789 2.266 .000 .981 53
a. Dependent Variable: Female Obesity (% of total population)
Regression
Variables Entered/Removed
Model Variables Entered Variables Removed Method
1 LNGDP1000,
DumSamoa,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
b
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .641
a
.410 .374 8.2015
a. Predictors: (Constant), LNGDP1000, DumSamoa, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
49. 49
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 2294.239 3 764.746 11.369 .000
a
Residual 3295.981 49 67.265
Total 5590.221 52
a. Predictors: (Constant), LNGDP1000, DumSamoa, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 15.836 2.008 7.885 .000
GDP1000 -.380 .181 -.488 -2.098 .041
DumSamoa 47.105 8.424 .624 5.591 .000
LNGDP1000 3.857 1.864 .485 2.069 .044
a. Dependent Variable: Female Obesity (% of total population)
Residuals Statistics
a
Minimum Maximum Mean Std. Deviation N
Predicted Value 11.421 63.000 18.887 6.6423 53
Residual -12.4035 22.2986 .0000 7.9614 53
Std. Predicted Value -1.124 6.641 .000 1.000 53
Std. Residual -1.512 2.719 .000 .971 53
a. Dependent Variable: Female Obesity (% of total population)
50. 50
Regression
Variables Entered/Removed
Model Variables Entered Variables Removed Method
1 DumUS,
DumSamoa,
LNGDP1000,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
b
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .721
a
.519 .479 7.4829
a. Predictors: (Constant), DumUS, DumSamoa, LNGDP1000, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 2902.535 4 725.634 12.959 .000
a
Residual 2687.686 48 55.993
Total 5590.221 52
a. Predictors: (Constant), DumUS, DumSamoa, LNGDP1000, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
51. 51
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 15.659 1.833 8.542 .000
GDP1000 -.581 .176 -.745 -3.296 .002
DumSamoa 47.364 7.687 .627 6.162 .000
LNGDP1000 4.995 1.735 .628 2.878 .006
DumUS 27.279 8.277 .361 3.296 .002
a. Dependent Variable: Female Obesity (% of total population)
Residuals Statistics
a
Minimum Maximum Mean Std. Deviation N
Predicted Value 5.393 63.000 18.887 7.4711 53
Residual -12.4616 15.8814 .0000 7.1893 53
Std. Predicted Value -1.806 5.904 .000 1.000 53
Std. Residual -1.665 2.122 .000 .961 53
a. Dependent Variable: Female Obesity (% of total population)
Regression
Variables Entered/Removed
Model Variables Entered Variables Removed Method
1 DumLUX, DumUS,
DumSamoa,
LNGDP1000,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
b
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .752
a
.565 .519 7.1920
a. Predictors: (Constant), DumLUX, DumUS, DumSamoa, LNGDP1000,
GDP1000
b. Dependent Variable: Female Obesity (% of total population)
52. 52
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 3159.155 5 631.831 12.215 .000
a
Residual 2431.066 47 51.725
Total 5590.221 52
a. Predictors: (Constant), DumLUX, DumUS, DumSamoa, LNGDP1000, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 15.362 1.767 8.695 .000
GDP1000 -.810 .198 -1.039 -4.087 .000
DumSamoa 47.738 7.390 .632 6.460 .000
LNGDP1000 6.421 1.787 .808 3.594 .001
DumUS 32.572 8.302 .432 3.923 .000
DumLUX 19.579 8.790 .259 2.227 .031
a. Dependent Variable: Female Obesity (% of total population)
Residuals Statistics
a
Minimum Maximum Mean Std. Deviation N
Predicted Value 6.796 63.000 18.887 7.7944 53
Residual -13.1886 15.1232 .0000 6.8375 53
Std. Predicted Value -1.551 5.660 .000 1.000 53
Std. Residual -1.834 2.103 .000 .951 53
a. Dependent Variable: Female Obesity (% of total population)
53. 53
Model 2
Regression (Male, BigMacIndex)
Variables Entered/Removed
Model Variables Entered
Variables
Removed Method
1 Big Mac Index,
DUMUS,
DUMLUX, Alcohol
Consumption,
Unemployment
(% of total labour
force), Secondary
school enrolment
(% net), Daily fat
supply (g) per
capita, Passenger
cars per 1000
people, LNGDP,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
b
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .840
a
.705 .377 5.7793
a. Predictors: (Constant), Big Mac Index, DUMUS, DUMLUX, Alcohol
Consumption, Unemployment (% of total labour force), Secondary school
enrolment (% net), Daily fat supply (g) per capita, Passenger cars per 1000
people, LNGDP, GDP1000
b. Dependent Variable: Male Obesity (% of total population))
54. 54
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 718.727 10 71.873 2.152 .132
a
Residual 300.602 9 33.400
Total 1019.330 19
a. Predictors: (Constant), Big Mac Index, DUMUS, DUMLUX, Alcohol Consumption, Unemployment (%
of total labour force), Secondary school enrolment (% net), Daily fat supply (g) per capita, Passenger
cars per 1000 people, LNGDP, GDP1000
b. Dependent Variable: Male Obesity (% of total population))
Regression (Male, BigMacIndex2)
Variables Entered/Removed
Model Variables Entered
Variables
Removed Method
1 BigMacIndex2,
DUMUS, Alcohol
Consumption,
DUMLUX,
Unemployment
(% of total labour
force), Secondary
school enrolment
(% net), Daily fat
supply (g) per
capita, Passenger
cars per 1000
people,
GDP1000,
LNGDP
a
. Enter
a. All requested variables entered.
55. 55
Model Summary
b
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .858
a
.736 .442 5.4695
a. Predictors: (Constant), BigMacIndex2, DUMUS, Alcohol Consumption,
DUMLUX, Unemployment (% of total labour force), Secondary school
enrolment (% net), Daily fat supply (g) per capita, Passenger cars per 1000
people, GDP1000, LNGDP
b. Dependent Variable: Male Obesity (% of total population))
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 750.088 10 75.009 2.507 .091
a
Residual 269.242 9 29.916
Total 1019.330 19
a. Predictors: (Constant), BigMacIndex2, DUMUS, Alcohol Consumption, DUMLUX, Unemployment (%
of total labour force), Secondary school enrolment (% net), Daily fat supply (g) per capita, Passenger
cars per 1000 people, GDP1000, LNGDP
b. Dependent Variable: Male Obesity (% of total population))
56. 56
Regression (Female, BigMacIndex)
Model Variables Entered
Variables
Removed Method
1 DUMLUX,
DUMUS, Big Mac
Index, Alcohol
Consumption,
Unemployment
(% of total labour
force), Secondary
school enrolment
(% net), Daily fat
supply (g) per
capita, Passenger
cars per 1000
people, LNGDP,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .877
a
.769 .513 5.6519
a. Predictors: (Constant), DUMLUX, DUMUS, Big Mac Index, Alcohol
Consumption, Unemployment (% of total labour force), Secondary school
enrolment (% net), Daily fat supply (g) per capita, Passenger cars per 1000
people, LNGDP, GDP1000
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 959.241 10 95.924 3.003 .057
a
Residual 287.497 9 31.944
Total 1246.737 19
a. Predictors: (Constant), DUMLUX, DUMUS, Big Mac Index, Alcohol Consumption, Unemployment (%
of total labour force), Secondary school enrolment (% net), Daily fat supply (g) per capita, Passenger
cars per 1000 people, LNGDP, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
57. 57
Regression (Female, BigMacIndex2)
Model Variables Entered
Variables
Removed Method
1 BM2, DUMUS,
Alcohol
Consumption,
DUMLUX,
Unemployment
(% of total labour
force), Secondary
school enrolment
(% net), Daily fat
supply (g) per
capita, Passenger
cars per 1000
people,
GDP1000,
LNGDP
a
. Enter
a. All requested variables entered.
Model Summary
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .910
a
.827 .635 4.8922
a. Predictors: (Constant), BM2, DUMUS, Alcohol Consumption, DUMLUX,
Unemployment (% of total labour force), Secondary school enrolment (%
net), Daily fat supply (g) per capita, Passenger cars per 1000 people,
GDP1000, LNGDP
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 1031.333 10 103.133 4.309 .019
a
Residual 215.405 9 23.934
Total 1246.737 19
a. Predictors: (Constant), BM2, DUMUS, Alcohol Consumption, DUMLUX, Unemployment (% of total
labour force), Secondary school enrolment (% net), Daily fat supply (g) per capita, Passenger cars per
1000 people, GDP1000, LNGDP
b. Dependent Variable: Female Obesity (% of total population)
58. 58
MODEL 3 – Physical Activity
Regression (male)
Variables Entered/Removed
Model Variables Entered
Variables
Removed Method
1 LNGDP, Alcohol
Consumption,
Unemployment (%
of total labour
force), Physical
Activity, Passenger
cars per 1000
people, Daily fat
supply (g) per
capita, BM2,
GDP1000
a
. Enter
a. All requested variables entered.
Model Summary
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .971
a
.943 .489 7.1291
a. Predictors: (Constant), LNGDP, Alcohol Consumption, Unemployment (% of
total labour force), Physical Activity, Passenger cars per 1000 people, Daily fat
supply (g) per capita, BM2, GDP1000
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 843.652 8 105.456 2.075 .493
a
Residual 50.824 1 50.824
Total 894.476 9
a. Predictors: (Constant), LNGDP, Alcohol Consumption, Unemployment (% of total labour force), Physical
Activity, Passenger cars per 1000 people, Daily fat supply (g) per capita, BM2, GDP1000
b. Dependent Variable: Male Obesity (% of total population))
59. 59
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) .149 95.191 .002 .999
GDP1000 2.951 2.050 5.242 1.440 .386
Unemployment (% of total labour
force)
3.878 8.908 .759 .435 .739
Daily fat supply (g) per capita .074 .341 .194 .217 .864
Alcohol Consumption .110 1.295 .036 .085 .946
Passenger cars per 1000 people .125 .098 2.228 1.277 .423
BM2 -35.212 88.211 -1.182 -.399 .758
Physical Activity .241 .906 .282 .266 .834
LNGDP -54.940 31.801 -7.184 -1.728 .334
a. Dependent Variable: Male Obesity (% of total population))
Regression (female)
Variables Entered/Removed
Model Variables Entered
Variables
Removed Method
1 LNGDP, Alcohol
Consumption,
Unemployment (%
of total labour
force), Physical
Activity, Passenger
cars per 1000
people, Daily fat
supply (g) per
capita, BM2,
GDP1000
a
. Enter
a. All requested variables entered.
60. 60
Model Summary
Model R R Square Adjusted R Square
Std. Error of the
Estimate
1 .976
a
.952 .565 6.6717
a. Predictors: (Constant), LNGDP, Alcohol Consumption, Unemployment (% of
total labour force), Physical Activity, Passenger cars per 1000 people, Daily fat
supply (g) per capita, BM2, GDP1000
ANOVA
b
Model Sum of Squares df Mean Square F Sig.
1 Regression 875.749 8 109.469 2.459 .458
a
Residual 44.512 1 44.512
Total 920.261 9
a. Predictors: (Constant), LNGDP, Alcohol Consumption, Unemployment (% of total labour force), Physical
Activity, Passenger cars per 1000 people, Daily fat supply (g) per capita, BM2, GDP1000
b. Dependent Variable: Female Obesity (% of total population)
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 8.241 89.084 .093 .941
GDP1000 3.140 1.918 5.498 1.637 .349
Unemployment (% of total labour
force)
3.101 8.336 .598 .372 .773
Daily fat supply (g) per capita -.008 .319 -.019 -.024 .985
Alcohol Consumption .375 1.212 .120 .310 .809
Passenger cars per 1000 people .103 .091 1.822 1.132 .461
BM2 -57.690 82.551 -1.909 -.699 .612
Physical Activity .538 .848 .621 .635 .640
LNGDP -58.286 29.761 -7.514 -1.958 .301
61. 61
Coefficients
a
Model
Unstandardized Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
1 (Constant) 8.241 89.084 .093 .941
GDP1000 3.140 1.918 5.498 1.637 .349
Unemployment (% of total labour
force)
3.101 8.336 .598 .372 .773
Daily fat supply (g) per capita -.008 .319 -.019 -.024 .985
Alcohol Consumption .375 1.212 .120 .310 .809
Passenger cars per 1000 people .103 .091 1.822 1.132 .461
BM2 -57.690 82.551 -1.909 -.699 .612
Physical Activity .538 .848 .621 .635 .640
LNGDP -58.286 29.761 -7.514 -1.958 .301
a. Dependent Variable: Female Obesity (% of total population)