2. OBJECTIVES
Describe the high quality of CPR and it’s impact on
survival.
Describe all the steps of chain of survival.
Apply the BLS concept in Chain of survival.
Learn about stages of coping of dying patient.
Learn about care of terminally ill patient.
Learn about care after death.
4. INTRODUCTION
International Studies approximately 50% of all deaths
are due to cardiovascular disease for the most part this
means heart attacks are the greatest killer in United
States more people die of heart attacks than of gunshots
,cancer ,AIDS or car accident.
If you wait and don’t take action to assist an individual in
need it’s possible that by the time help arrives the
person may be brain dead. Human brain may survive
without oxygen up to four minutes without suffering any
permanent damage.
5. ANATOMY & PHYSIOLOGY
The cardiovascular system maintains blood
fl
ow
to deliver oxygen and nutrients to every cell and
removes the carbon dioxide and waste products
made by those cells.
The heart is a muscular organ which pumps a
continuous
fl
ow of blood through the blood
vessels of the circulatory system. The main
components of the heart are:
1. Heart muscles -contract to pump blood.
2. Heart chambers -collect and channel blood
fl
ow.
3. Heart valves -allows only one-way
fl
ow of
blood.
4. Conduction system -coordinate heart muscle
contraction
5. Coronary blood vessels -supply blood to the
heart
6. Effective external chest compressions push blood
out of heart chambers and thus maintain blood
fl
ow and oxygen delivery to the heart, brain and
other vital organs.
The heart will fail to maintain a good blood
fl
ow if it
pumps at a too slow rate (less than 60/min), too
fast (more than 150/min) or unorganized rhythm
(ventricular
fi
brillation).
The coronary blood vessels supply oxygen to the
heart muscles and conduction system.
Most of blood
fl
ow (perfusion) to the heart
muscles occur during the diastole (relaxation)
phase.
Full chest recoil is important to allow for adequate
perfusion to the heart muscles and blood
fi
lling of
the heart chambers during the relaxation (diastole)
phase
IMPORTANCE OF CHEST RECOIL
7. The human body needs oxygen to sustain life.
After about four minutes without oxygen, brain
cells start dying and can lead to irreversible brain
damage and ultimately death.
The main components in respiratory system are:
1. Airways-to channel air to the lungs.
2. Lungs and blood vessels-for gas exchange
3. Muscles for breathing-to move air in and out of
the lungs
Room air contains 21% oxygen. Rescue
breathing using exhaled air contains 16% oxygen.
Most child-related cardiac arrests occur as a
result of a hypoxic event. Therefore, breathing
and oxygenation are important for a successful
resuscitation.
The tongue may occlude the upper airway in an
unconscious patient.
ANATOMY & PHYSIOLOGY OF THE
RESPIRATORY SYSTEM

7
8. DEFINITION
CPR is a technique of basic life support for the purpose
of oxygenation to the heart, lungs and brain until
appropriate medical treatment can come and restore
the normal cardiopulmonary function.
9. HISTORICAL REVIEW
The
fi
rst arti
fi
cial mouth to mouth respiration was given
in 5000 BC
Ventilation started at 3000 BC
First step of newborn resuscitation by blowing in 1780
First experimental direct cardiac massage in 1874
First successful direct cardiac massage in man in 1901
First experimental indirect cardiac massage and
de
fi
brillation done in 1946
Indirect cardiac massage in 1960
Development of cardio pulmonary resuscitation due to
the works of Peter safar 1980
10. PURPOSE OF CPR
To maintain blood circulation by external cardiac
compressions.
To maintain an open clear airway to maintain breathing
by external ventilation to save life of the patient to
provide basic life support till medical and advanced life
support arrives.
To support and restore effective oxygenation and
circulation with intact neurologic function and return of
spontaneous circulation.
11. INDICATIONS OF CPR
Cardiovascular disorders :Coronary artery disease,
CHD ,congenital heart disease ,coronary
embolism ,cardiac rupture and dissection.
Pulmonary embolism ,pulmonary edema and asphyxia
Metabolic causes hyperglycemia and electrolyte
imbalances
Fluid imbalance , extensive hemorrhage, hypotension and
shock
12. INDICATIONS OF CPR
Neurological causes, brain injuries and massive CVA
Poison, substance and drug overdose
Carbon monoxide poisoning and propranolol overdose
Other causes: electrical shock hyperthermia, narcotic
overdose
15. ADVANCED AIRWAYS
Endotracheal Tube: It is a
speci
fi
c type of tracheal tube that
is inserted through the mouth or
nose. It is the most technically
dif
fi
cult airway to place
Laryngeal Mask Airway (LMA)
is an advanced airway
alternative to ET intubation and
provides comparable ventilation.
Esophageal-Tracheal Tube:
(sometimes referred to as a
combitube) is an advanced
airway alternative to ET
intubation. This device provides
adequate ventilation comparable
to an ET tube.
18. WARNING SIGNS OF CARDIAC
ARREST
Early signs: loss of consciousness and convulsions
Late signs apnea, dilated pupil ,absence of Heart
sound
Changes in respiratory rate a weak or irregular pulse,
bradycardia ,cyanosis ,hypothermia.
Tightness of the chest ,the person may describe a
sensation as if someone was sitting on the chest
causing dif
fi
culty in breathing .
19. WARNING SIGNS OF CARDIAC
ARREST
Any chest pain or breathing dif
fi
culties be reported .
Sweating along with cool pale skin. Nausea and
vomiting.
Denial is another sign usually accompanied by any one
of the signs listed above heart attack victims often say
that they are having pain due to indigestion heartburn
asthma or illness.
20. WARNING SIGNS OF CARDIAC
ARREST
The longer you argue with the person about the validity
of their symptoms the less time they may have to live.
Don’t wait until the heart stops.
As the heart issues continues the heart may eventually
stop beating this is called cardiac arrest. If the person is
in cardiac arrest does not get help immediately he will
be likely to die.
22. PARTS OF BLS
Chest compressions (C)
Airway (A)
Breathing (B)
De
fi
brillation(D)
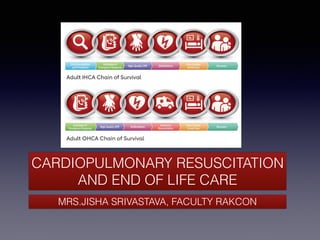
23. CHAIN OF SURVIVAL IN HOSPITAL
Surveillance, prevention and treatment of pre-arrest condition
by activating RRT(Rapid Response Team).
Immediate recognition of cardiac arrest and activation of code
blue.
Early CPR with emphasis on on chest compressions.
Rapid de
fi
brillation.
Multidisciplinary post cardiac attack care.
24. CHAIN OF SURVIVAL OUTSIDE
Immediate recognition of cardiac arrest and activation of
Emergency Response Team
Early CPR with emphasis on chest compressions.
Rapid de
fi
brillation with AED.
Effective Advanced Life Support.
Multidisciplinary post cardiac attack care.
25. STEPS OF BLS
Scene safety (check for surrounding for any hazards)
Assessment
Active emergency response system and get automated
external de
fi
brillator
Check pulse (Carotid) not more than 10 seconds
Begin cycles of 30 compressions and two breaths if you
do not de
fi
nitely feel a pulse within 10 seconds
Perform
fi
ve cycles of CPR (30:2) with C A B (chest
compressions airway breathing sequence)
26. 1. SCENE SAFETY
Assess to make sure the scene is safe for you to respond
to the patient.
Is it Safe to approach the victim, I may suffocate/ get
burnt/get hypothermic /get electric shock.
Is it safe for the victim to be attended to were he has
collapsed indeed to take victim out of water or switch off
the main switch to start cardio pulmonary resuscitation.
27. 2. ASSESSMENT
Assess Responsiveness: Stimulate and speak to the adult
asking if they are ok.
Look at the chest and torso for movement and normal
breathing.
If unresponsive: if not breathing or breathing is not normal,
gasping
(One provider)
fi
rst call the emergency response team and
bring an AED to the patient.
(Two providers) Have someone near call the emergency
response team and bring the AED and the other provider
can start CPR
Place patient supine on a hard
fl
at surface.
28. 3.CIRCULATION
Check the patient for a carotid pulse for 5-10 seconds. (Do not check for more than 10
seconds.). Locate the larynx and move two
fi
ngers to the side to palpate the carotid
pulse.
If the patient has a pulse: Move to the airway and rescue breathing portion of the
algorithm: Provide 10 rescue breaths per minute (1 breath every 6 seconds). Recheck
pulse every 2 minutes.
If the patient doesn’t have a pulse: Begin 5 cycles of CPR (lasts approximately 2
minutes).
Start with chest compressions: Provide 100 to 120 compressions per minute. This is 30
compressions every 15 to 18 seconds.
Place your palms midline, one over the other, on the lower 1/3 of the patient’s sternum
between the nipples
lock your arms.
29. Using two arms press to a depth of 2 inches
(5cm) on the patient’s chest.
Press hard and fast.
Allow for full chest recoil with each
compression.
1 cycle of adult CPR is 30 chest
compressions to 2 rescue breaths.
If two providers are present: switch rolls
between compressor and rescue breather
every 5 cycles.
Mechanism increase of intra thoracic
pressure and direct compression of the heart
recommended.
3.CIRCULATION
30. 4. AIRWAY
In the event of a witnessed collapse with
no reason to assume a C-spine injury
Use the Head Tilt-Chin Lift maneuver:
place your palm on the patient’s forehead
and apply pressure to tilt the head
backward.
Place the
fi
ngers of your other hand
under the mental protuberance of the chin
and pull the chin forward and cephalic.
31. 4. AIRWAY
In the event of an unwitnessed
collapse, drowning, or trauma:
Use the Jaw Thrust maneuver.
(This maneuver is used when a
cervical spine injury cannot be
ruled out.):Place your
fi
ngers on
the lower rami of the jaw.
Provide anterior pressure to
advance the jaw forward.
32. Scan the patients chest and torso for
possible movement. Watch for abnormal
breathing or gasping.
If the patient is breathing adequately:
Continue to assess and maintain a patent
airway and place the patient in the recovery
position. (Only use the recovery position if
its unlikely to worsen patient injury).
If the patient is not breathing or is breathing
inadequately: If the patient has a pulse:
Commence rescue breaths immediately.
If the patient has no pulse: Begin CPR.
(move to the “Circulation” portion.)
5.BREATHING
33. 5.BREATHING
Use a barrier device if
available.
Pinch the patient’s nose
closed.
Make a seal using your mouth
over the mouth of the patient
or use a pocket mask or bag
mask.
34. 5.BREATHING
For bag mask use C and E
technique.
Each rescue breath should last
approximately 1 second. Watch
for chest rise. Allow time for the
air to expel from the patient.
During normal CPR without an
advanced airway: Provide
approximately 6-8 rescue breaths
per minute.
5.BREATHING
35. During normal CPR with an advanced
airway: Provide 10 rescue breaths per
minute (don’t pause chest compressions
for breaths).
If patient has a pulse and no CPR is
required: Provide 10 rescue breaths per
minute (1 breath every 6 seconds).
Recheck pulse every 2 minutes.
If there is a foreign body obstruction:
Perform abdominal thrusts
5.BREATHING
36. RECOVERY POSITION
Lateral recumbent or 3/4 prone position:
This position is used to maintain a
patent airway in the unconscious
person.
Place the patient close to a true lateral
position with the head dependent to
allow
fl
uid to drain. Assure the position
is stable.
Avoid pressure of the chest that could
impairs breathing.
Position patient in such a way that it
allows turning them onto their back
easily.
Take precautions to stabilise the neck in
case of cervical spine injury.
Avoid the recovery position if it will
sustain injury to the patient.
37. DEFIBRILLATOR
Arrival of the AED (Automated
External De
fi
brillator)
1.POWER ON
Turn AED On NOW! (early
de
fi
brillation is the single most
important therapy for survival of
cardiac arrest and should be done as
soon as it arrives).
Follow verbal AED prompts.
38. 2. ATTACHMENT
Firmly place appropriate
pads (adult/pediatric) to
patient’s skin to the indicated
locations (pad image).
1. Anterolateral 2.
Anteroposterior
DEFIBRILLATOR
39. 3. ANALYSE
A short pause in CPR is required to
allow the AED to analyze the rhythm.
If the rhythm is not shockable: Initiate 5 cycles of CPR.
Recheck the rhythm at the end of the 5 cycles of CPR.
If the shock is indicated: Assure no one is touching the
patient or is in mutual contact of a good conductor of
electricity by yelling “Clear, I’m Clear, you’re Clear!” prior
to delivering a shock.
Press the shock button when the providers are clear of
the patient.
Resume 5 cycles of CPR.
DEFIBRILLATOR
40.
41. ADVANCED CARDIOPULMONARY LIFE SUPPORT (ACLS)
DEFINITION
Advanced cardiac life support (ACLS) is a group of
procedures and techniques that treat immediately life-
threatening conditions, including cardiac arrest, shock,
stroke, and trauma.The goal of ACLS is to stabilize
patient’s condition. This includes restoring normal vital
signs and alertness.
42. DIFFERENCE BETWEEN BLS AND ACLS
BLS stands for Basic Life Support. BLS involves a variety
of life-saving skills and techniques, like CPR — a
combination of chest compressions and rescue breaths
BLS is performed mostly by healthcare professionals, like
doctors, physicians, nurses, EMTs (Emergency Medical
Technicians), paramedics, but also
fi
rst responders like
police of
fi
cers and
fi
re
fi
ghters.
BLS is performed when patients are in cardiac arrest,
respiratory arrest or distress, or when there is an
obstructed airway. Besides the skills and techniques
involved with BLS, other necessary skills like working well
in a team environment, critical thinking, and problem-
solving are all vitally important.
43. DIFFERENCE BETWEEN BLS AND ACLS
ACLS stands for Advanced Cardiovascular Life Support. In
ACLS, healthcare professionals use a set of algorithms to
treat conditions ranging from cardiac arrest and myocardial
infarctions (heart attacks) to stroke and other life-threatening
emergencies.
ACLS providers must have the skills and knowledge to place
advanced airways and insert an IV (Intravenous) or IO
(Intraosseous) line for the administration of
fl
uids and
medications.
And they must have a thorough understanding of all the
medications available to them that are used to treat for the
variety of heart rhythms and conditions they will encounter.
44. 1.CPR QUALITY
Push hard (at least 2 inches [5 cm]) and fast (100-120/
min) and allow complete chest recoil.
Minimize interruptions in compressions.
Avoid excessive ventilation.
Change compressor every 2 minutes, or sooner if
fatigued.
If no advanced airway, 30:2 compression-ventilation ratio.
Quantitative waveform capnography – If Petco2 is low or
decreasing, reassess CPR quality.
45. 2. SHOCK ENERGY FOR
DEFIBRILLATION
Biphasic: Manufacturer recommendation (eg, initial dose
of 120-200 J); if unknown, use maximum available.
Second and subsequent doses should be equivalent, and
higher doses may be considered.
Monophasic: 360 J
46. 3. DRUG THERAPY
Epinephrine(sympathomimetic catecholamine is the
primary drug administered during cardiopulmonary
resuscitation (CPR) to reverse cardiac arrest. Epinephrine
increases arterial blood pressure and coronary perfusion
during CPR via alpha-1-adrenoceptor agonist effects.) IV/IO
dose: 1 mg every 3-5 minutes
47. 3. DRUG THERAPY
Amiodarone(anti-arrhythmic drug works by blocking certain
electrical signals in the heart that can cause an irregular
heartbeat) IV/IO dose: First dose: 300 mg bolus. Second
dose: 150 mg. or
Lidocaine(antiarrhythmic drug blocks cardiac sodium
channels shortening the action potential and is used
intravenously only for arrhythmia.)IV/IO dose: First dose:
1-1.5 mg/kg. Second dose: 0.5-0.75 mg/kg.
48. 4. ADVANCED AIRWAY
Endotracheal intubation or supraglottic advanced
airway
Waveform capnography or capnometry to con
fi
rm and
monitor ET tube placement
Once advanced airway in place, give 1 breath every 6
seconds (10 breaths/min) with continuous chest
compressions
49. 5. RETURN OF SPONTANEOUS
CIRCULATION(ROSC)
Pulse and blood pressure
Abrupt sustained increase in Petco2 (Postapneic End-Tidal
Carbon Dioxide Pressure)(typically ≥40 mm Hg)
Spontaneous arterial pressure waves with intra-arterial
monitoring
51. 5 H’S AND MANAGEMENT
Hypovolemia :warmed crystalloids and/or blood products
Hypoxia :Proper oxygenation and ventilation
Hydrogen ion (acidosis):If a patient has respiratory
acidosis, they can be treated by providing adequate
ventilation. Metabolic acidosis is one of the most common
abnormalities in patients suffering from serious diseases,
and there have been numerous etiologies and treatments
of the underlying disease as the basis of therapy.21 A
common intervention to treat metabolic acidosis may be by
the administration of sodium bicarbonate.
52. 5 H’S AND MANAGEMENT
Hypo/hyperkalemia:Hyperkalemia can be treated by
administering sodium bicarbonate or calcium chloride or by
performing dialysis.
Treatment of hypokalemia gradual replacement of potassium
to normal serum levels. In an emergency, intravenous
potassium is warranted, with the knowledge that many
patients who are hypokalemic are also hypomagnesimic.
Repletion of magnesium stores will facilitate more rapid
correction of hypokalemia and is recommended in severe
cases of hypokalemia.7
Hypothermia:active external methods (e.g., forced warm
air) and minimally invasive methods (e.g., warm IV
infusions).25
53. 5T’S AND MANAGEMENT
Tension pneumothorax: Treatment of a tension
pneumothorax is either needle compression and/or
thoracostomy with chest tube placement.
Tamponade, cardiac:Thoracotomy or pericardiocentesis is
used to treat cardiac arrest
54. 5T’S AND MANAGEMENT
Toxins :
The drug of choice for the treatment of benzodiazepine overdose
is Flumazenil.
The drug of choice for the treatment of opioids are naloxone are
0.4–2 mg IV, IO, IM or SC, and may be repeated every 2–3
minutes.
Beta-blocker toxicity :Improvement has been reported with
glucagon (50–150 mcg kg−1), high-dose insulin and glucose, lipid
emulsions, phosphodiesterase inhibitors, extracorporeal and
intra-aortic balloon pump support, and calcium salts.
Treatment of Calcium channel blocker overdose can include the
administration of calcium chloride 10% in boluses of 20 ml (or
equivalent dose of calcium gluconate) every 2-5 minutes in
severe bradycardia or hypotension followed by an infusion as
needed.
55. 5T’S AND MANAGEMENT
Thrombosis, pulmonary : Speci
fi
c treatments for
cardiac arrest resulting from pulmonary embolism
include administration of
fi
brinolytics, surgical
embolectomy and percutaneous mechanical
thrombectomy.
Thrombosis, coronary: Treatment options include
immediate coronary angiography, primary percutaneous
coronary intervention (PPCI) or other interventions such
as (more rarely) pulmonary embolectomy.
67. POSSIBLE COMPLICATIONS OF
CPR
Coronary vessel injury
Die from injury
Hemoperitoneum
Hemothorax
Interference with
ventilation
Liver injury
Myocardial injury
Pneumothorax
Rib fractures
Spleen injury
Sternal fracture
68.
69. POST RESUSCITATION CARE
Post-resuscitation care is meant to optimize ventilation and
circulation, preserve organ/tissue function, and maintain
recommended blood glucose levels. Below
fi
nd a
systematic approach followed by a post-resuscitation care
algorithm to guide you in your treatment.
70. RESPIRATORY SYSTEM
Chest X-ray to verify ET tube placement
Arterial blood gas (ABG) and correct acid/base
disturbance
Pulse oximetry (continuously monitor)
Heart rate and rhythm (continuously monitor)
End-tidal CO2 (if the patient is intubated)
Maintain adequate oxygenation (saturation between
94% and 99%)
POST RESUSCITATION CARE
71. RESPIRATORY SYSTEM
Maintain adequate ventilation to achieve PCO2 between
35 to 45 mm Hg unless otherwise indicated.
Intubate if:Oxygen and other interventions do not
achieve adequate oxygenation
Needed to maintain a patent airway in the child with a
decreased level of consciousness
Ventilation is not possible through non-invasive means,
e.g., continuous positive airway pressure (CPAP)
Control pain with analgesics and anxiety with sedatives
(e.g. benzodiazepines)
POST RESUSCITATION CARE
72. CARDIOVASCULAR SYSTEM
Arterial blood gas (ABG) and correct acid/base
disturbances
Hemoglobin and hematocrit (transfuse or support as
needed)
Heart rate and rhythm (continuously monitor)
Blood pressure (continuously monitor with arterial line)
Central venous pressure (CVP)
Urine output
POST RESUSCITATION CARE
73. CARDIOVASCULAR SYSTEM
Chest X-ray
12 lead ECG
Consider echocardiography
Maintain appropriate intravascular volume
Treat hypotension (use vasopressors if needed and
titrate blood pressure)
Pulse oximetry (continuously monitor)
Maintain adequate oxygenation (saturation between
94% and 99%)
Correct metabolic abnormalities (chemistry panel)
POST RESUSCITATION CARE
74. GASTROINTESTINAL SYSTEM
Monitor nasogastric (NG)/orogastric (OG) tube for
patency and residuals
Perform a thorough abdominal exam
Tense abdomen may indicate bowel perforation or
hemorrhage
POST RESUSCITATION CARE
75. GASTROINTESTINAL SYSTEM
Consider abdominal ultrasound and/or abdominal CT
Routine blood chemistries including liver panel
Arterial blood gas (ABG) and correct acid/base
disturbances
Be vigilant for bleeding into the bowel, especially after
hemorrhagic shock
POST RESUSCITATION CARE
76. HEMATOLOGICAL SYSTEM
Monitor complete blood count and coagulation panel
Transfuse (as needed)Correct thrombocytopenia
Fresh frozen plasma is to replenish clotting factors
Consider calcium chloride or gluconate if massive
transfusion required
Correct metabolic abnormalities (chemistry panel),
especially after transfusion
POST RESUSCITATION CARE
77. NEUROLOGICAL SYSTEM
Elevate head of bed if blood pressure can sustain cerebral
perfusion
Temperature:Avoid hyperthermia and treat fever aggressively
Do not re-warm hypothermic cardiac arrest victim unless
hypothermia is interfering with cardiovascular function
Treat hypothermia complications as they arise
Blood glucoseTreat hypo/hyperglycemia (hypoglycemia
de
fi
ned as less than or equal to 60 mg/dL)
Monitor and treat seizures: Seizure medications
POST RESUSCITATION CARE
78. NEUROLOGICAL SYSTEM
Monitor and treat seizures: Seizure medications
Remove metabolic/toxic causes
Blood pressure (continuously monitor with arterial line)
Maintain cardiac output and cerebral perfusion
Normoventilation unless temporizing due to intracranial swelling
Frequent neurological exams
Consider CT and/or EEG
Dilated unresponsive pupils, hypertension, bradycardia,
respiratory irregularities, or apnea may indicate cerebral
herniation
POST RESUSCITATION CARE
79. RENAL SYSTEM
Monitor urine output: Infants and small children: > 1 mL/kg
an hour Larger children: > 30mL an hour
Exceedingly high urine output could indicate neurological or
renal problem (diabetes insipidus)
Routine blood chemistries
Arterial blood gas (ABG) and correct acid/base
disturbances
POST RESUSCITATION CARE
80. RENAL SYSTEM
Urinalysis (when indicated)
Maintain cardiac output and renal perfusion
Consider the effect of medications on renal tissue
(nephrotoxicity)
Consider urine output in the context of
fl
uid resuscitation
Toxins can sometimes be removed with urgent/emergent
hemodialysis when antidotes fail or are not available
POST RESUSCITATION CARE
81. ETHICAL ISSUES IN CPR
Patients who may bene
fi
t from resuscitation efforts should
have equitable access to such efforts.
Decisions to attempt resuscitation must take into account
the accepted standards of medical care, the safety of the
medical personnel, and known patient preferences.
It is appropriate for out-of-hospital providers to honor valid
orders to limit life- sustaining interventions at the end of life.
Educational information regarding such policies should be
disseminated to the community and to out-of-hospital and
hospital providers.
82. ETHICAL ISSUES IN CPR
Patient goals and preferences for end of life care should be
honored by out-of- hospital and hospital providers at the
end of life.
EMS out-of-hospital order systems should support efforts to
provide or forgo these treatments based on available
information.
The appropriate surrogate decision-maker, as de
fi
ned by
state law, should be involved in decisions regarding life-
sustaining treatments if immediately available.
83. ETHICAL ISSUES IN CPR
If the patient’s goals or medical circumstances are unclear,
medically appropriate resuscitative measures should be
undertaken.
It is ethically permissible for treatments, once started, to be
withdrawn when additional information becomes available.
This information may include the lack of response to
treatment or de
fi
nitive information about the patient’s goals
for life-sustaining treatments.
84. ETHICAL ISSUES IN CPR
Resuscitative efforts may also be appropriately not initiated,
withdrawn, or limited in unsafe situations, such as during a
global pandemic, a violent situation, or an environmental
disaster, in order to protect staff properly.
Facilities should develop protocols to guide alteration of
resuscitation practices in these extraordinary
circumstances.
When resuscitative efforts are not indicated, emergency
physicians should assure appropriate medical and
psychosocial care during the dying process.
86. SUMMARY AND CONCLUSION
Of course, as professionals, we know how important it is to not
only get the training you need, but to do so as ef
fi
ciently as
possible, which is why our BLS blended learning courses also
include adaptive learning functionality, which allows you to
receive personalized, focused courses. Basic Life Support
(BLS) is a level of medical care used in emergency, life-
threatening situations until the victim can be cared for
professionally by a team of paramedics or at a hospital. It can
help people who are choking, drowning or are suffering from
cardiac arrest, and it can make the difference between life and
death for some people.
87. RESEARCH ARTICLE
Comparative assessment of basic life support knowledge
between professional nurses and nursing students
Implications of the study
Registered nurses appeared to have more knowledge in BLS than nursing
students at AAUJ. However, the mean score of both nurses and students were
almost similar. In addition, with regard to BLS knowledge, there was no
signi
fi
cant difference between nurse's experience and the academic level of
nursing students. The gap between nurses and students' knowledge of BLS
needs to be
fi
lled. Moreover, continuous evaluation of knowledge of BLS and
practice is needed to provide answers to the consequences of inadequate
knowledge of BLS. Nurses who have been working for 10 years or more are
unable to retain their basic and advanced resuscitation skills for long. An
improvement in BLS skill retention is crucial to reduce possible disability and
death caused by time lag in resuscitation.Overall, this study strengthens the
idea that using high
fi
delity simulation scenarios can enhance and retain both
knowledge and skill more than the classical BLS courses.
89. INTRODUCTION
Lost grief and death are universal facets of life. A person’s
reaction to loss is inclined by importance of what was lost
and the culture in which the person is raised. Death is a
universally shared event. All cultures and religions have
beliefs and rituals to explain and cope with death loss and
grief. It is common in American Society to avoid talking
about death and to be unable to imagine our own
death.Children are often kept away from funerals and
most people have little contact with dying
90. DEFINITION OF DEATH
Death is de
fi
ned as cessation of heart, lung function, of whole
brain function, or of higher brain function
According to president’s Commission for the study of ethical
problems in medicine and biomedical and behavioral
research United States 1983 de
fi
ned death is either
irreversible cessation of circulatory and respiratory functions,
irreversible cessation of all functions of the entire brain
including the brain stem.
91. THE NATURE OF DEATH
Except for suicide a person has no control over when or
how death occurs.
Death may be sudden unexpected and instant, as when a
person is killed in an accident or dies of a massive heart
attack or stroke ,death may also be the end of a long battle
against chronic disease such as cancer or heart disease or
simply the diminished function of multiple systems in old
age.
Each death and dying experience is unique.
92. CULTURAL CONSIDERATIONS
Right to know if they are dying .
Mexican Americans and Korean Americans are less likely
to want to be told if they have a terminal illness they also
believe that the family not the patient should make
decisions about life sustaining treatments .
Certain cultures believe that talking about death can bring
it on example: Greece, China, Italy ,Korea ,Mexico and
the southern African nations .
American Indian culture included a fear of death and it is
thought that truth telling about the terminal prognosis
violates the tradition and taboos and can lead to harmful
outcomes.
93. DEFINITION OF END OF LIFE CARE
Care given to people who are near the end of life and
have stopped treatment to cure or control their disease.
End-of-life care includes physical, emotional, social,
and spiritual support for patients and their families.
94. GOALS OF END OF LIFE CARE
The goal of end-of-life care is to control pain and other
symptoms so the patient can be as comfortable as
possible.
95. RIGHTS OF DYING PATIENT
The person who is dying has the
right to:
Be treated as a person until Death.
Caring human contact.
Pain control.
Cleanliness and comfort.
Maintain a sense of hope whatever
its focus.
Participate in his care or planning of
it.
Respectful caring ,medical and
nursing attention.
Continuity of care and caregiver.
Information about his condition and
impending death.
Honest answers to questions.
Explore and change religious beliefs.
Maintain individuality and express
emotions freely without being judged.
Make amends with others and settle
personal business.
Say goodbye to family members and
signi
fi
cant others in private or with
the assistance of the nurse.
Assistance for signi
fi
cant others with
grief process.
Withdraw from social contact if
desired.
Die at home in familiar surroundings.
Die with dignity.
Respectful treatment of the body
after death.
96. STANDARDS OR GOOD END OF LIFE
CARE
You must consider the terminally ill patient’s preferences,
personality and lifestyle when planning care .
Rigid rules ,routines and agency regulations should not be
automatically applied.
Every effort is made to maintain functional capacity and to
relieve discomfort through the control of symptoms
regardless of the expected length of time until death.
97. STANDARDS OR GOOD END OF LIFE
CARE
Pain control is a major goal of treatment.
The patient’s preferences and intentions regarding health
care as set out in an advance directive or by durable power
of attorney for health care will take precedence as far as law
will allow.
The patient should feel safe and secure with the care that is
provided and with the level of communication regarding this
care.
98. The patient will have ample opportunities to
fi
nish business
with loved ones and to say goodbyes.
Opportunities will be provided for the dying patient to spend
fi
nal moments in a personally meaningful way with people
who are important to the patient.
STANDARDS OR GOOD END OF LIFE
CARE
99. Family members and signi
fi
cant others will have opportunities
to discuss the patient’s imminent death and their emotional
needs with the staff.
Family members and signi
fi
cant others will be provided
private time with patient before and after death as desired.
Family members will be allowed to perform rituals and carry
out cultural customs regarding the body after death
STANDARDS OR GOOD END OF LIFE
CARE
100. SETTINGS OF END OF LIFE CARE
End-of-life care may include
Palliative care
Supportive care
Hospice care.
101. HOSPICE AND PALLIATIVE CARE
Hospice is a philosophy of care for dying and their families it
was developed in England in the early 90s as a reaction to
the dying person’s needs for care and comfort.
The intent of Hospice care is to help patients in the end
stage of life and their families experience and process of
death with the highest quality of life and least amount of
disruption as possible
Philosophy of hospice is based on the acceptance of death
as a natural part of life and emphasize the quality of
remaining life.
102. HOSPICE AND PALLIATIVE CARE
The patients not only suffered from physical aspects of the
disease such as pain but they suffer from psychological,
spiritual and emotional discomfort as well.
The needs of the patient and their signi
fi
cant others are met
through a multidisciplinary team approach where the team
provides palliative care
103. HOSPICE AND PALLIATIVE CARE
Palliative care is concerned with treating symptoms and
things providing comfort measures and promoting the best
quality of life .
Nurses who care for dying patients have a unique
opportunity to become an intimate part of their lives nurses
can support dying patients physically and emotionally while
maintaining a professional role.
109. CHANGES IN CIRCULATORY SYSTEM
Decreased blood perfusion
Mottled discoloured skin
Decreased cerebral perfusion
Decreased level of perfusion
Delirium
Disorientation
Hallucination
110. CHANGES IN CIRCULATORY SYSTEM
Drowsiness
Decrease in Cardiac output and intravascular volume
Tachycardia
Hypotension
Peripheral cynosis
Peripheral cooling
Pulse become weak and irregular
111. CHANGES IN INTEGUMENTARY
SYSTEM
Increase risk of pressure related injuries
Decreased blood perfusion
Decreased mobility
Decreased nutritional status
Increased risk of friction and shearing
113. CHANGES IN NEUROLOGICAL
SYSTEM
Decreased or loss of consciousness
Dif
fi
culty understanding or
fi
nding the right words
Sensation and power loss in legs
fi
rst, followed by hands
Pupils might become sluggish to light
Pain might be signi
fi
cant
114. CHANGES IN URINARY SYSTEM
Decreased Urine out put
Decreased intake
Blood pressure too low for kidney
fi
ltration
Possible Incontinence
116. SIGNS OF IMPENDING DEATH
1. PHYSICAL SIGNS
As death approaches the patient grows physically weaker
and begins to spend more time sleeping. Body functions
slows ,appetite decreases and the patient may refuses
even favorite foods and later
fl
uids as well.
Explain to the patient and the family what to expect
Moistening the patients lips and mouth and providing oral
hygiene will be more comforting than pushing foods or
fl
uids.
117. SIGNS OF IMPENDING DEATH
Urine output decreases on urine becomes more
concentrated .
There may be a edema of the extremities and over the
sacrum.
Incontinence may occur as patient becomes less
aware of their surroundings however be alert to the
possibility of urinary retention and the need for
catheterization.
118. Vital signs change as death approaches the pulse increases
and becomes weaker or thready blood pressure declines
and skin of the extremities becomes mottled cool and dusky
Respirations becomes shallow and irregular, secretions may
pull in the lungs causing respirations to sound most often at
the time of death followed by periods of apnea no breathing
may be noted
SIGNS OF IMPENDING DEATH
119. Body temperature may rise and the patients if responsive
may complain of feeling hot or cold although the extremities
are cool to the touch as circulations slows.
Blanket should be used as the patient desires
SIGNS OF IMPENDING DEATH
120. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
As outlined in kuebler Ross stages of coping with dying it
is hope that the patient will have reached the stage of
acceptance as death draws closer during this time the
patient will talk about making Funeral arrangements and
putting my affairs in order to die with closure is to say
goodbye to those people and things that are important
121. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
It may also involve saying I am sorry, forgive me ,I forgive
you and I love you.It is a time when patient may or gives
to family and friends special memories or positions
A life review can assist patient in telling their story and
putting their life in perspective helping the patient right or
share his story of life with signi
fi
cant others allows them
to keep special memories of their loved ones.
122. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
As individuals approached death their spiritual needs
take on greater importance .
Religious practices and rituals have great signi
fi
cance
work for some patients it is important for you to be
familiar with those beliefs
Rather than impose your own religious beliefs on dying
patients and family you should assist patients in
fi
nding
comfort and support in their own belief system
123. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
Everyday activities and news are not of interest in
nonverbal communication becomes most holding
important
Holding their hands stroking their hair are most
meaningful always be aware of the remarks you make .
They do hear. Hearing is believed to be one of the last
sensors to be lost before death .
May exhibit confusion and disorientation
124. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
They may report dreams or visions of deceased
relatives and they usually not frightened by these
experiences.
Often this is comforting and they may speak of
preparing for a journey to join loved ones at times .
125. PSYCHOLOGICAL AND SPIRITUAL
ASPECTS OF DYING
Patients may become restless and agitated ,adequate
pain and anxiety medication can ease the these
symptoms
Keep silence soft light in the room and assurance that it
is OK to go and that family members will be take care of
each other may ease the dying individuals anxiety
about leaving their responsibilities.
126. SIGNS OF CLINICAL DEATH
Absence of pulse heartbeat and respiration
Pupil becoming
fi
xed and not reacting to light
Absence of all re
fl
exes
No ECG activity
Rigor mortis stiffening of the body after death ,the arms
and legs cannot be bent or straightened .
Postmortem hypostasis it is a dark red or bluish
discoloration due to the settling of the blood
127. GRIEF
Grief is the total emotional feeling of pain and distress
that a person experiences as a reaction to loss..
People who are dying and their loved ones experience
loss and grief when faced with a terminal diagnosis.
Bereavement is the state of having suffered a loss by
death
A person who is grieving may experience physical and
emotional symptoms such as crying, fatigue, changes in
appetite, sleep disturbances ,loneliness and sadness.
128. SYMPTOMS OF GRIEF
Depression sadness crying and mood swings
Fatigue ,apathy ,lack of interest and motivation
Inability to concentrate
Inability to complete task
Loneliness, isolation, sleep alterations, sleep
more ,insomnia
129. SYMPTOMS OF GRIEF
Loss of appetite ,weight loss or weight gain ,nausea
Changing sexual interest
Anxiety, shortness of breath, chest pains, rapid heartbeat,
sighing ,heaviness in chest feeling of helplessness,
Restlessness ,Anger, guilt etc
Symptoms of same illness that the deceased suffered
130. FACTORS AFFECTING GRIEF AND
DEATH
Childen , young and
middle age
Family
Socioeconomic
factors and Cultural
Factors
Nurse Patient
131. FACTORS AFFECTING GRIEF AND
DEATH
CHILDREN : The child’s development may be retarded due to
the death of a parent or the child regress.
YOUNG AND MIDDLE AGED ADULTS: Seperation from loved
one is dif
fi
cult to accept
FAMILY: They feel lost auto what to say and how to act
PATIENT: Some people frankly express their feelings and fear
and some hide it and some act aggressive.
NURSE: Her reaction largely depends on her own past
experiences.
SOCIOECONOMIC FACTORS: A bereaved family may suffer
more acutely if there is no other earning members in the family.
CULTURAL INFLUENCES: Cultural background necessities
the family members to display emotion and distress.
132. STAGES OF GRIEF: Engel(1964)
SHOCK AND DISBELIEF: No, Not me
DEVELOPING AWARENESS: is characterised by physical and
emotional responses, such as anger, feeling empty, or crying
why me
RESTITUTION: Rituals surrounding loss, religious, cultural or
social expression of mourning
IDEALIZATION: Exaggeration of the good qualities of the
person or object lost
OUTCOME: Final resolution of grief process, including dealing
with loss as a common life occurrence.
133. MEETING THE NEEDS OF GRIEVING
INDIVIDUAL
Assist people who are grieving by accepting their
feelings and behaviours and validating their loss.
To validate the loss is to reassure the grieving person
that the loss was important and understood. Quiet
presence ,a warm caring concern for the person’s well
being and ability to listen to person speak about the pain
and loss are supportive.
Encourage the grieving individuals to tell you what the
person or lost object was like and what the loss means to
them. Avoid the use of clinches like ‘you will forget all
about this after a while ‘and do not minimize the loss
Observe the patients nonverbal communications and use
appropriate nonverbal language such as a gentle touch.
134. MEETING THE NEEDS OF GRIEVING
INDIVIDUAL
Crying maybe embarrassing for the patient and a simple
act of handing the tissue acknowledges the acceptability of
weeping.
You should avoid saying I know just how you feel or don’t
cry because this minimizes the patient’s feelings.
Finally with the stages of acceptance the level of daily
function begins gradual improvement .
Successful movement through the grieving stages allows
the person to emerge with realistic memories of the event
and the deceased ; to
fi
nd renewed energy and a sense
that life has meaning and to attain experience, pleasure,
social relationships and activities. The time it takes to
move through the stages depends on the laws and its
meaning to the person.
135. KUEBLER ROSEANNE 5 STAGES OF
COPING WITH IMPENDING DEATH
1. DENIAL: no not me, the person cannot believe the
diagnosis or prognosis denial serves as a buffer to protect the
patient from an uncomfortable and painful situation.A patient
may seek other opinions or believe there has been an error.
2. ANGER: Why me the person looks for a cause or
fi
xes
blame displaced anger may target physicians ,nurses family .
3. BARGAINING: if I am good then I get reward, the wishes
for extension of life or later for relief from pain and the person
knows from the past experience that good behavior is often
rewarded.
136. KUEBLER ROSEANNE 5 STAGES OF
COPING WITH IMPENDING DEATH
4. DEPRESSION: It's hopeless there is a sense of great loss
of the impending loss of being people mourn losing family,
positions ,responsibilities and all they value.
5. ACCEPTANCE: I am ready, the pain is gone, the struggle
is over, the patient has found peace .There is withdrawal from
engagement in everyday activities ,an interest ,verbal
communication is less important and touch are most
important.
137.
138. HOPE AND DYING PROCESS
Hope is an inner positive life force a feeling that what is
desired is possible.
It takes many forms and changes as the patient
declines.
At
fi
rst there is hope for cure then a hope that might be
for treatment will be possible, next a hope for
prolonging life and
fi
nally for a peaceful death.
Such as what are you hoping for from this admission or
what are you hoping for today can allow patient to
talk .You can always be supportive of recognizing and
af
fi
rming the wish the patient is expressing.
140. 1. ADDRESSING THE PATIENT’S FEAR
OF DYING
Patient expressed many fears when they know they are dying
: fear of pain loneliness, abandonment ,the unknown, loss of
dignity and loss of control
There may also be un
fi
nished business that occupies the
patients thoughts. The concept of comfort care focuses on
identifying symptoms that cause the patients distress and
adequately treat those symptoms
The application of the nursing process to care of the dying
patient uses skills and knowledge from physical emotional
social and spiritual context
Throughout the nursing process therapeutic communication is
an important skill the nurse uses to promote communication.
141. 1. ADDRESSING THE PATIENT’S FEAR
OF DYING
The
fi
rst step in addressing these fears is to is for you to
become comfortable with your own beliefs values and
attitudes about death and dying second read and learn
about actual dying process and observe experienced
nursing personal talking with dying patients
Open to the dif
fi
cult questions of life and death that permits
patient to discuss their feelings and needs patience are
usually sensitive as to how caregivers react too
uncomfortable subjects.
Fears of isolation or loneliness decrease with nursing care
that seeks to treat the patient with compassion and
individuality. The families anxiety decreases as they see the
patient responding to the care attention to the team.
142. 2. ASSESSMENT AND DATA
COLLECTION
A baseline assessment including data collection are essential to identify the problems and needs of the patient and
his family.
Questions about advance directives regarding treatment options ,resuscitation, advanced life support or organ
donation can provide information about the patient’s attitude towards death and the stages of his grief or dying
reaction, denial anger etc
Asking questions about religious beliefs and practices as well as asking directly what do you hope for during this
admission and what are your concerns illicits data or for the provision of comprehensive comfort care
At no time should the patient be pushed to discuss something he’s obviously avoiding a question such as is there
anything else you do like to talk about opens the door for issues the patient may wish to discuss.
An assessment of the patients physical condition include such as measures as weight mobility and ability to perform
activities of daily living ,weakness or energy level ,appetite ,nausea, indigestion, gas bowel and bladder function and
respiratory function
Be special attention to assessing pain location nature an what relieves it or makes it worse pain should be assessed
using zero to 10 scale or similar method of measuring the patients reporter of page the frequency of pain
assessment depends on many factors such as the severity of pain and whether pain is increasing or well controlled
on the current treatment regimen
The patients emotional condition can often be observed during the interaction an symptoms such as anxiety,
agitation ,confusion or depression may be obvious
Validating your observation with patient allows him to speak about his feelings stating tell me how you are coping
with all this begins to identify strengths and needs.
spiritual assessment can begin with questions about patients religious a
fl
iction and whether he would like to meet
with the spiritual advisor, chaplain ,Robbie religious leader even when a patient indicate none for religious af
fi
liation.
af
fi
liation he may have spiritual needs close regarding spiritual distress may be found in questions
such as why is God punishing me or what what the meaning in his life has been
143. 3. NURSING DIAGNOSIS
Common nursing diagnosis for the patient who is dying:
Activity intolerance
Death anxiety
De
fi
cient knowledge
Fatigue
Fear
Grieving
Imbalanced nutrition less than body requirements
Impaired physical mobility
Impaired skin integrity
Pain
Risk for loneliness
Self care de
fi
cit
144. 4. PLANNING
It is important to include the patient and his family in planning
care and establishing goals or outcomes.
Planning should be a team effort with all members of the team
aware of patient goals and needs
Giving the patient control is the most is the
fi
rst priority at a
time when it seems that he has no control
As far as possibly agency rules and routines that are geared
towards cure should be relaxed to recognize that the goal is
comfort
This would include relaxing restrictive visiting hours eliminating
routine vital signs and laboratory work and avoiding rigid
schedules for getting up bathing or sleeping therapy.
The patients who do not respond to theses treatment can be
given nerve blocks.
145. 1.ANTICIPATORY GUIDANCE
Anticipatory death assist in preparing the family and
patient by giving them guidance about physical
changes, symptoms and complications that may arise.
This may also aid the patient and family in deciding
about possible Hospice care.
146. 2. END STAGE SYMPTOM
MANAGEMENT
Many expected symptoms suggest pain,
gastrointestinal distress, dyspnea, fatigue, cough death
rattle and delirium are related to metabolic changes at
the end of life .
The last few days of patient life have been studied
extensively.
The nurse must recognise these symptoms and be able
to either alleviate them or help explain them to the
patient and family.
147. 3. PAIN CONTROL
The nursing research has demonstrated safe and effective principle of pain
control .
Many terminally ill patients unnecessarily die with uncontrolled pain it is
perhaps the best the
fi
rst fear patients have regarding dying .
Pain can be controlled illuminated in most all cases when the medical and
nursing team works together
Regularly scheduled pain medication with PRN backup for breakthrough pain is
one of the most effective method of controlling pain
There is no risk of becoming addicted or of reaching a safety or effectiveness
limit when narcotics are increased in response to pain for the dying patient
Transdermal fentanyl patch has helped eliminate the burden of pain at the end
of the life.
Non chemical method approaches to a pain relief include visualisation and
guided image ,imagery relaxation and breathing exercises, massage ,music
therapy ,meditation, religious healing bio feedback, hypnosis or self hypnosis,
transcutaneous electrical nerve stimulation TENSE and hydrotherapy Whirlpool
etc. Teach the patient one or more of these simple techniques as adjoint to drug
148. 4. CONSTIPATION , DIARRHEA
Constipation is predictable for a patient receiving opiates
experiencing decreased
fl
uid intake and mobility and having
certain abnormal disease .
Antiemetics ate the
fi
rst choice to eliminate nausea and vomiting
In addition to classic nursing measures for preventing
Constipation increasing
fi
bre,
fl
uids and exercise consult with
physician for orders for stool softeners and standing laxative
order
suppository's and enemas or manual disimpaction can be
avoided in most cases with careful monitoring and adherence to
laxative.
149. 5. ANOREXIA, NAUSEA , VOMITING:
Anorexia all loss of appetite may do be due to nausea ,drug
side effects ,the disease process or slow down that occurs
naturally in the dying process.
Antiemetics are
fi
rst choice to eliminate the nausea and
vomiting .
Small servings of home prepared food favourites and attention
to illuminating unpleasant sights and odors at meal time may
stimulate poor appetite and bad tastes can be improved by
frequent oral care ,mouthwash or hard candies
A nutritionist may be helpful in suggesting food choices that
are appealing and easily digested.
Dysphagia (dif
fi
culties in swallowing) may also be a problem .
Moistening the mouth with
fl
uids or arti
fi
cial saliva may be
helpful
150. 6. DEHYDRATION
As death nears patients spent more time sleeping or in a semi
responsive state, they take in fewer and fewer
fl
uids until the
question arises about providing intravenous
fl
uids or tube feeding
out of concern for dehydration.
Research has shown that dehydration results in less distress and
pain and that hydration does not improve comfort .
Dry mouth and thirst are the most common complaints which may
be induced by the drugs being administered and these can be
alleviated by small sips of
fl
uids and lip lubrication.
151. 7.DYSPNEA
Dif
fi
culty breathing may be seen early in the dying process in certain lungs
or heart disorders it is also seen shortly before death when respirations may
become noisy irregular or labored
secretions in the lungs accumulate and block their way to contribute to
noisy or rattling respiration the patient is usually not responsive or not
aware of the diypnea but it is upsetting to family members.
Suctioning is not effective in clearing the secretion but medication
suggests scopolamine patch or morphine can decrease secretions and
ease breathing administering oxygen by nasal prongs may provide comfort.
152. 8.DEATH RATTLE
Noisy respirations are heard when patient can no longer
clear their throats of normal secretions. Family members
are often alarmed and are afraid the patient will choke to
death in these cases .
Scopolamine or morphine drugs that are known to reduce
secretions may be used to quite the patient and bring
breathing back to normal.
153. 9.DELIRIUM
Dying patients may experience hallucinations or altered
mental status
nurses must
fi
rst search for cause such as pain
positional discomfort or bladder distinction and address
those physical problems
next nurses should discuss the delirium with the
patient’s family and increase the family to talk to the
patient in quiet tones while remaining calm
154. 10.IMPAIRED SKIN INTEGRITY
Weight loss ,decrease nutrition ,in continuance and inactivity all
contribute to the risk of skin breakdown.
Turn and position the patient use protective measures such as
an air pressure mattress heel or elbow protectors, a sheepskin
or form pads and keep the skin clean and dry.
An indwelling or condom catheter may be indicated to
conserve the patient’s indwelling energy and to prevent skin
breakdown.
155. 11.WEAKNESS, FATIGUE,DECREASED
ABILITY TO PERFORM DAILY LIVING
Weakness fatigue decrease ability to perform activities of
daily living increasing weakness eventually results in the
patients becoming bedbound .
Accept the patient’s wishes regarding walking ,sitting up
in a chair or remaining in bed .
The dying patient is not going to get stronger or better he
gets weaker and weaker not because he’s lying in bed
but because he’s dying.
Allow the patient to do as much as possible for himself
and provide physical care when he is no longer able
156. 12. ANXIETY, DEPRESSION, AGITATION
OR PSYCHOLOGICAL SYMPTOMS
Anxiety ,depression ,agitation ,emotional or psychological
symptoms may be treated with appropriate drugs with
good effect.
Listen and use good therapeutic communication skills to
allow the patient to express his fears ,feelings and needs
to convey nonjudgmental acceptance .
Skillful assessment of these symptoms may identify
physical pain or spiritual distress that can be treated
157. 13. SPIRITUAL DISTRESS, FEAR OF
MEANINGLESSNESS
Each person needs to believe that his life has had
meaning; this is the spiritual nature of the dying
process.
A life review allows the patient to put his life in
perspective.
Reminiscing is one way of starting a life review .
Encouraging the patient to tell about family
photographs or albums ask what was it like when you
were a child , worked on the farm, lived in the city and
met your wife it is more important to listen than to talk
158. 6. EVALUATION :
It is based on speci
fi
c expected outcomes written for the
patient.
The outcome depends on which nursing diagnosis are
pertinent to patients situation
In most cases the degree of comfort obtained for the patient by
nursing interventions need to be evaluated .
Was pain adequately controlled?
Was tissue integrity protected ?were actions to facilitate the
patients and family grieving process effective ? was the
patients fear alleviated ? did interventions for a self care de
fi
cit
make the patient more comfortable? answers to these
questions help determine whether expected outcomes have
been met if the care plan is not effective then plan must be
revised
160. After the physician has pronounced death and legally
documented the death in medical record , the care of the
body is performed by the nurse.
An autopsy consent may be requested and obtained , if
required.
If the patient is to be an organ donor, arrangements will be
made immediately.
The family often wishes to view the body before
fi
nal
preparations are made.
If the patient had any valuables they are handed over to the
relatives.
CARE OF BODY AFTER DEATH
161. PURPOSES
Make the body look natural and beautiful as possible .
Perform his last rites tenderly
Do everything you can for the relatives.
Protect other patients from unpleasant sights and
sound which could frighten them
162. PREPARATION OF ARTICLES
Articles for bath
Disposable gloves gown mask and other protective
clothes
Absorbable pads gauze dressings
Perineal pads
Restrains for jaw, hands and legs
Dressing for draining wounds
Cotton swabs
Thumb Forceps
Patient’s own set of clothes
Body wraps (Sheets)
Identi
fi
cation tags
163. STEPS OF PROCEDURE
Review the institution policy on post mortem care and follow
institutional policy and hand over the patients possession to
family members.
Wash the hands don gloves ,gown and mask
Maintain the alignment of the body place the body in supine
position
164. STEPS OF PROCEDURE
Gently close the eyes and mouth of the body
If possible place dentures in the mouth of the body.
To give normal appearance to the body jaw should be
supported with the help of a bandage
165. STEPS OF PROCEDURE
Remove all the appliances used for the care of the patient for
example urinary catheter nasogastric tubes IV Lines.
Clean the body parts with sponge bath to remove strains and
secretions.
Remove soiled dressing and replace with clean gauze
dressing.
166. STEPS OF PROCEDURE
Brush and comb the hairs of patient.
Plug all body ori
fi
ces suggest such as ears, nose, vagina
mouth with cotton plugs and place protective absorbing pads
under buttucks.
Dress the body in a clean own dress if family will be viewing
the body and remain with them unless they wish to be alone.
167. STEPS OF PROCEDURE
Place the padded ties around the ankles: crisscross the
wrists over the abdomen and secure; and place a gauze tie
or chin strap under the jaw keep the mouth closed.
Identi
fi
cation tag should contain patients name ,Hospital
registration number relative name, specify address, ward
number, bed number, date and time of death and cause of
death.
168. STEPS OF PROCEDURE
Place the body on the shroud or in the morgue bag and
check for placement of drainage pads and secure the shroud
at the chest ,waist and knees and place ID tag on the outside
the shroud.
Attach a special label if the patient had a contagious disease
Transfer the body to the mortuary.
169. RECORDS AND REPORT
Vital signs and time of absence of same events leading to
the death
Time when physician declared death
Any marks wounds bruises on the body before death and
are made during care of the body.
Removal or securing of drains and tubes
Time of noti
fi
cation to the family
Remove of jewellery and replacement of dentures
Consent forms and release forms signed
Time when body was taken to the morgue.
Processing for Death Certi
fi
cate
171. LEGAL AND ETHICAL ISSUES IN THE
ASPECT OF DEATH
The health care system is still grappling with the care of the
dying patient patients right to make decision about end of life
situations advanced directives and the designation of a health
care proxy have gained legal and public acceptance
172. 1. ADVANCE DIRECTIVES
An advanced directive spells out patients wishes for health
care at the time when they may be unable to indicate their
choice.
A durable power of attorney for health care is a legal
document that appoints a person’s health care proxy chosen
by patient to carry out his wishes.
Their choices regarding arti
fi
cial feeding and
fl
uids ,ventilators and administration of antibiotics , DNR are
documented.
173. 1. ADVANCE DIRECTIVES
The form provides orders for emergency medical personnel
regarding end of life wishes and summarizes a person’s
advanced directives
Nurses must keep upto date on legal decisions related to
these issues and continue to learn and apply new nursing
theory and procedures regarding end of life care they must
also deal with their own feelings and values regarding patients
choices to seek life drowning or death seeking treatment
174. 2.EUTHANASIA
Euthanasia is the act of ending another persons life to end
suffering with or without his consent it may be called mercy
killing .
some distinction is also made between active and passive
euthanasia .Passive euthanasia occurs when a patient
choose to die by refusing treatment that might prolong life
an example would be withholding arti
fi
cial feeding or
parenteral
fl
uids when the patient is unable to take them
orally.
175. 2.EUTHANASIA
It would also include not treating pneumonia with antibiotics.
on during the refusal of life longing treatment of a patient
with a terminal illness is legall and activie Euthanasia is
generally de
fi
ned as administering a drug or treatment to
end the patient’s life.
Euthanasia is not legal in India
176. 3.ADEQUATE PAIN CONTROL
Adequate pain control is another issue that affects the
comfort of the dying.
Physicians may be reluctant to prescribe large enough
doses of pain medication for fear of legal action under the
control section they may also be concerned about being
viewed as as prescribing a lethal doses in an assisted
suicide effort .
177. 4. ORGAN DONATION
Kidneys ,livers ,hearts and lungs are organs that can be
transplanted from one person to another
Other tissues suggest corneas ,bone and skin can also be
transplanted.
The need for organs and tissues for transplantation far exceeds the
supply every day people die waiting for a transplant people can
indicate their wish to be donors on their drive those licenses are in
advanced directives but the next of kin must give permission to
remove the organs or tissues of that person.
178. 4. ORGAN DONATION
Physicians are usually the people who request organ donation from
family members but you may be in a position to answer questions
the family raises about organ donation
You should know that donation of organs does not delay Funeral
arrangements there is no of evidence that organs were removed
when the body is dressed and there is no cost to the family for the
removal of organs donated
179. 5. AUTOPSY IN INDIA
Post mortem is a Latin phrase literally means ‘after death’. A post
mortem examination is a medical examination carried out on the
body after death. It is also called an autopsy (which means ‘to see
for oneself’).
The protocol stipulates that post-mortem for organ donation be taken
up on priority and be conducted even after sunset at the hospitals
which have the infrastructure for conducting such post-mortem on a
regular basis.
180. 5. AUTOPSY IN INDIA
It is also to be ensured by the facility that video recording of post-
mortem shall be done for all post-mortem conducted in the night, to
rule out any suspicion and preserved for future reference for Legal
purposes.
However, cases under categories such as homicide, suicide, rape,
decomposed bodies, suspected foul play should not be subjected
for post-mortem during night time unless there is a law-and-order
situation.
181. SUMMARY AND CONCLUSION
Death Is the most dif
fi
cult loss human beings
experience.Nurses assist the grieving through
validation of the loss and coping skills and caring
support. Hope is a positive life force.
182. RESEARCH ARTICLE
What matters most for end-of-life care? Perspectives from community-based palliative care providers and administrators
Abstract
Objectives There has been little research conducted to understand the essential meaning of quality, community-based,
end-of-life (EOL) care, despite the expansion of these services. The purpose of this study was to de
fi
ne what matters
most for EOL care from the perspective of a diverse range of palliative care providers in the community who have daily
encounters with death and dying.critical domains of EOL care evolved from the interviews, indicating that quality EOL
care extends beyond managing physical pain, but includes a holistic perspective of care, a healthcare team dedicated to
the EOL journey and a patient-centred pathway. Tailoring the provision of care to consider these important elements plays
a critical role in supporting a positive EOL experience for patients and families.
Nine critical domains of EOL care evolved from the interviews with the large cross-section of palliative care providers
serving home settings. Many of the themes we found correspond to the broader
fi
ndings of previous research and
palliative care's best practice elements employed in many countries.The contribution that our study makes is in denoting
which elements of EOL are the most essential: quality EOL care extends beyond managing physical pain, but includes a
holistic perspective of care, a healthcare team both dedicated and
fl
exible to accompanying their patients and families on
this journey, and is patient centred. Resourcing and building palliative care programmes that embody these philosophies
play a crucial role in supporting a positive EOL experience for patients and families.
183. BIBLIOGRAPHY
The Trained Nurses Association of India, Fundamentals of Nursing , Procedure manual,Edition 2009
American Heart Association, Basic Life Support Provider Manual 2020
American Heart Association, Advanced Life Support Provider Manual 2020
Sushma Pandey, Principles and Procedures of Nursing Foundation, vol-1
Dewit, ONeil, Fundamental Concepts and Skills for Nursing, edition-4
Dr. Vijay kumar Gauttam, Advanced practises in Nursing
Navdeep Kaur Brar, Text book of Advanced practises in Nursing,
https://www.acls-pals-bls.com/algorithms/bls/UNITED MEDICAL EDUCATION
https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/algorithms
https://cpr.heart.org/en/resources/cpr-facts-and-stats
184. EVALUATION
1. A dying patient has excessive secretions that are caus- ing
dyspnea. Which medication will best help dry the secretions
and increase comfort? Select all that apply.
a. Haloperidol
b. Scopolamine
c. Acetaminophen
d. Diazepam
185. EVALUATION
2. What are nursing interventions the nurse can provide at the end of life? Select all that apply.
(A)Position the patient to increase comfort and prevent
complications.
(B)Provide comfort measures such as massage.
(C)Research experimental treatments that may help
the patient
fi
nd a cure.
(D)Administer medications to increase comfort.
(E)Teach the family CPR for use if the patient dies
when the nurse is not present.
(F)Sit quietly with the patient and family.
186. 3. A 94-year-old gentleman is admitted from home to the hospital with
pneumonia. What factors lead the nurse to believe he is nearing the
end of his life?
(A)His abdomen is distended and his skin tone is
yellow.
(B)He has a fever of 101.6F and a respiratory rate of
28.
(C)He has been having dif
fi
culty swallowing and is
losing weight.
(D)He has crackles in his lung bases bilaterally.
EVALUATION
187. 3. A patient’s family member says, “I heard someone
say my mother could have a ‘good death.’ What on earth is a good death?” Which
response by the nurse is best?
(A)“Some things that can contribute to a good death are allowing patients to make
their own decisions at the end of life, and assuring that they die comfort- ably.”
(B)“In reality, no death is a good death, but we do our best to make sure patients
are comfortable right up until they die.”
(C)“Research has shown that patients can die good deaths if they are kept
sedated so they don’t really know what is happening during the last days until
they die.”
(D) “A good death occurs when the patient is kept alive as long as possible, so
she can take care of all her ‘un
fi
nished business’
fi
rst.”
EVALUATION