Liver Transplantation
•Als PPTX, PDF herunterladen•
10 gefällt mir•1,494 views

The presentation will help you explore about the procedure of Liver Transplantation.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie Liver Transplantation
Ähnlich wie Liver Transplantation (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Liver Transplantation
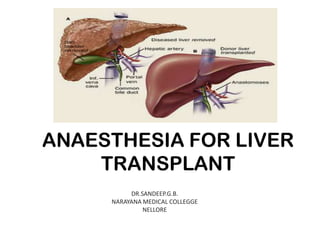
- 1. ANAESTHESIA FOR LIVER TRANSPLANT DR.SANDEEP.G.B. NARAYANA MEDICAL COLLEGGE NELLORE
- 2. OVERVIEW • • • • • • • • • • • • INTRODUCTION INDICATIONS AND CONTRAINDICATIONS SCORING SYSTEMS PATHOPHYSIOLOGY OF END-STAGE LIVER DISEASE PREOPERATIVE EVALUATION AND COMPLICATIONS INTRAOPERATIVE MANAGEMENT MAINTENANCE OF ANAESTHESIA PRE-ANHEPATIC PHASE ANHEPATIC PHASE POST ANHEPATIC PHASE HAEMOSTATIC DISORDERS AND MANAGEMENT POSTOPERATIVE CARE
- 3. INTRODUCTION • Liver transplant surgery is a fairly uncommon procedure in our country. • Liver replacement is the sole life saving procedure for patients with end stage liver disease(ESLD). • The most commonly used technique is orthotopic transplantation
- 4. • The two major goals of liver transplantation are – to prolong survival and – to improve quality of life. • Improvements in organ preservation, surgical technique, the advent of better immunosuppressive agents, the management of coagulopathy, and the Rx of infections, has resulted in a great expansion of this procedure
- 5. INDICATIONS Acute liver failure • • • Acute hepatitis A Acute hepatitis B Drug/toxin hepatotoxicity Cirrhosis from chronic liver diseases • • • • • • Chronic hepatitis B virus and chronic hepatitis C virus infection Alcoholic liver disease Autoimmune hepatitis Cryptogenic liver disease Primary biliary cirrhosis and primary sclerosing cholangitis Secondary biliary cirrhosis Metabolic Disorders • • • • • • Alpha-1 antitrypsin deficiency Hereditary hemochromatosis Wilson’s disease Glycogen-storage disorders Type 1 hyperoxaluria Familial homozygous hypercholesterolemia Malignancy • • Primary hepatic cancer: hepatocellular carcinoma and cholangiocarcinoma Metastatic: carcinoid tumors and islet cell tumors Miscellaneous • • Polycystic liver disease Budd-Chiari syndrome
- 6. CONTRAINDICATIONS Absolute contraindications • • • • • • • • • • • Brain death Extrahepatic malignancy Active uncontrolled infection Active alcoholism and substance abuse AIDS Severe cardiopulmonary disease-CAD, PULM. HTN, Uncontrolled sepsis Inability to comply with medical regimen Lack of psychosocial support Anatomic abnormalities precluding liver transplantation Compensated cirrhosis without complications Relative contraindications • Cholangiocarcinoma • Portal vein thrombosis • Psychologic instability
- 7. TESTS TO EXCLUDE CONTRAINDICATIONS • INFECTIOUS DISORDERS : HIV, Syphilis, EBV, CMV, Toxoplasmosis • MALIGNANCY : – Colonoscopy / ERCP in primary sclerosing cholangitis – In HCC: bone scan, lung CT (metastatic work-up) Screening (colon, breast, cervical, prostate cancer) • CARDIOPULMONARY STATUS : CXR, ECG,2D-ECHO, Thallium stress test, coronary angiography, PFT
- 8. SCORING SYSTEMS • Child-Turcotte-Pugh (CTP) classification
- 9. DRAWBACKS:• Ascites and encephalopathy, are subjective because they are assessed by physical examination alone. • Second, when other methods are used (ultrasonography, psychometric testing, EEG), a different degree of severity is diagnosed • The absence of an assessment of renal function, which is a well-established prognostic marker in cirrhosis
- 10. MODEL FOR END-STAGE LIVER DISEASE (MELD) SCORE:It is a mathematical formula based on the following factors: 1. Creatinine (for adult patients undergoing dialysis twice a week within the last week, the creatinine value would be automatically set to 4 mg/dL) 2. Bilirubin (mg/dL) 3. International normalized ratio
- 11. • Predictive of 3-month mortality in patients with chronic liver disease.
- 12. • Pediatric End-Stage Liver Disease (PELD) scoring system incorporates the following criteria : – – – – – Albumin Total bilirubin INR Growth failure Age (<1 y) • PELD score = 0.436 (age [<1 y]) – 0.687 x Log e (albumin g/dL) + 0.480 x Log e (total bilirubin mg/dL) + 1.857 x Log e (INR) + 0.667 (growth failure [<-2 SD present])
- 13. PATHOPHYSIOLOGY CNS CHANGES: • Hepatic encephalopathy and Raised ICP are common • Accumulation of NH3 and Mn leads to alteration in NT like GABA, Glutamate and NO. • The enzymes of the urea cycle are absent in the brain. • The resulting accumulation of glutamine, an osmotic compound, targets the glial astrocytes and results in cerebral edema in acute liver failure • Recently, the blood breakdown products hemin and protoporphyrin IX have been suggested as possible endogenous BDZ contributing to hepatic encephalopathy because they are potent activators of GABA receptors
- 15. CARDIOVASCULAR SYSTEM • Hyperdynamic state characterized by increased cardiac output and arteriolar vasodilatation • Vasoactive substances bypassing normal hepatic metabolism are most likely responsible. • Cannabinoids, Nitric oxide and guanosine 3,5-cyclic monophosphate (cGMP) have been implicated as mediators • Cardiomyopathy has been associated with alcoholic cirrhosis and hemochromatosis
- 16. • Rhythm disturbances may result from electrolyte or acid–base abnormalities. • Evaluate for IHD– Dobutamine stress echo (DSE) is the preferred preoperative screening study because it assesses the adequacy of myocardial oxygen supply, valvular function, and the presence of intrapulmonary shunting or portopulmonary hypertension
- 17. PULMONARY SYSTEM • Restrictive lung disease • Intrapulmonary shunts • Pulmonary hypertension
- 18. PULMONARY SYSTEM HEPATOPULMONARY SYNDROME Decreased oxygenation (PaO2 <70 mm Hg or a PAO2 - PaO2 gradient >20 mm Hg on room air) associated with intrapulmonary vascular dilation. • A hallmark of this syndrome is intrapulmonary shunting. • Presence of orthodeoxia is a significant clue • Resolves spontaneously after liver transplant
- 19. PULMONARY SYNDROME PORTOPULMONARY HYPERTENSION: (1) Mean pulmonary arterial pressure greater than 25 mm Hg, (2) Pulmonary vascular resistance greater than 120 dyne · sec · cm-5, and (3) Pulmonary capillary wedge pressure less than 15 mm Hg in the setting of portal hypertension
- 20. RENAL SYSTEM • Renal dysfunction is usually the result of – Primary renal disease – Acute tubular necrosis – Hepatorenal syndrome(HRS). • For diagnosis of HRS – A urinary sodium level <10 mEq/L or a fractional excretion of sodium <1% , – Creatinine level of more than 1.5 mg/dl, – A urine volume of less than 500 mL/day
- 21. • Spontaneous bacterial peritonitis is considered the most frequent cause of renal failure in patients with cirrhosis • The mechanism of hepatorenal syndrome is thought to be a combination of reversible renal vasoconstriction in structurally normal kidneys and changes in vasoconstrictor and vasodilator factors.
- 22. • There are two types of hepatorenal syndrome. • Type I : – Rapid onset over weeks, progressive and has high mortality. – Renal function may recover spontaneously when liver function improves – Most common in patients with acute liver failure, alcoholic hepatitis, or acute decompensation of CLD • Type II – Less acute – Seen in patients who become resistant to diuretic therapy.
- 23. HEMATOLOGICAL – Hypocoagulability and Impaired synthesis of coagulation factors (except factor VIII, Von Willebrand Factor) – Hypofibrinogenaemia occurs in the terminal stages of liver failure – Impaired synthesis of coagulation inhibitors – Synthesis of abnormal clotting proteins (dysfibrinogenaemia) – Insufficient clearance of activated and degraded clotting products – Vitamin K deficiency
- 24. • Enhanced fibrinolytic activity – Increased levels of circulating t-PA activity(impaired hepatic clearance, secondary to coagulation activation, induced by portal hypertension) – Diminished synthesis of fibrinolysis inhibitors(alpha 2 antiplasmin, PAI-1) • Quantitative and qualitative platelet defects – – – – – Increased splenic pooling Accelerated immune mediated platelet destruction Thrombin dependent platelet consumption Defective bone marrow destruction Disturbed platelet vessel wall interaction
- 25. Gastrointestinal System • Portal pressure increases • Once a critical level of portal hypertension is reached, portosystemic collaterals form to decompress the portal system. • Problems related to Portal Hypertension a) Oesophageal Varices b) Hypersplenism c) Ascites d) Spontaneous Bacterial Peritonitis (SBP)
- 26. Hepatic Synthetic Function • Plasma concentrations of – albumin, – plasma cholinesterase and – coagulation proteins are decreased in patients with liver disease
- 27. Metabolic dysfunction • Glucose metabolism :– Diminished hepatic glycogen stores as well as impaired gluconeogenesis in patients with liver disease may result in severe hypoglycaemia. – Hence high dose IV glucose infusions must be continued during patient transport as well as intraoperatively, and blood glucose concentrations should be measured frequently during surgery.
- 28. • Ammonia – – It is produced by deamination of amino acids and other organic amines and is converted to urea by the liver. – The BUN level may therefore be low in patients with ESLD, whereas the ammonia concentration may be markedly elevated. – Ammonia itself is neurotoxic and its accumulation in the blood is associated with hepatic encephalopathy
- 29. PHARMACOLOGY
- 30. Surgical procedure • Dissection phase • Anhepatic phase • Reperfusion (neohepatic) phase
- 31. PREOPERATIVE CONSIDERATIONS • Most tests are likely to show that either the patient is fit for surgery without any further medical therapy, or medical management is needed before liver transplantation. • Screening for any new infections on the day of surgery also is crucial because new-onset or uncontrolled ongoing infections may require postponement of surgery. • Avoid intramuscular injectons
- 32. Common investigations are • Full blood count – to establish anaemia, thrombocytopenia or evidence of infection. • Pro-thrombin time –PT may also be raised due to vitamin K deficiency; • Baseline renal function – in patients with cirrhosis a creatinine in the normal range may indeed represent renal impairment. • S.Electrolytes
- 33. • ECG and echocardiography - to help establish ventricular function and the presence of cardiomyopathy, valvular lesions or raised pulmonary vascular pressure. • Exercise ECG or stress echo – the chronic state of vasodilatation may mask ischaemia by limiting ventricular workload, stress testing may be useful where undiagnosed ischaemia is suspected. • CXR or ultrasound imaging of chest - to establish the presence of effusions amenable to preoperative drainage, may be helpful in optimising peri-operative respiratory function. • Pulmonary function tests -
- 34. BLOOD PRODUCTS • 10 U Of Red Blood Cells • 10 U Of Fresh Frozen Plasma • 4 U Of Single-donor Platelets • 10 U Of Cryoprecipitate
- 35. • Prepare the theater
- 36. INTRAOPERATIVE MANAGEMENT • Hemodynamic monitoring • Adequate fluid flow sheets should be maintained. • The frequency of blood sampling for laboratory analysis is dictated by the medical condition of the patient, progress of the procedure, and experience of the transplant team
- 37. Monitor LidCo
- 38. • i.v access • No epidural- deranged coagulopathy • Pulmonary artery catheter, TEE, IBP and CVP monitoring, after induction
- 39. Induction • The patient should only be transported to the operating theatre once the donor organ has been harvested and deemed suitable for transplantation. • Premedication • Induction- Propofol, Thiopentone, Etomidate with or without opioid and short or intermediate acting NMBD
- 40. Issues • An increased risk of pulmonary aspiration. • Nasotracheal intubation is contraindicated • Appropriate tracheal tube size and positioning are especially important in infants and children undergoing LT. • Alterations in hepatic drug metabolising capacity in patients with liver disease will influence the rate of elimination but not the duration of action after a single IV injection.
- 41. • ESLD results in – – – – changes in hepatic blood flow, decreased ability to biotransform certain drugs, hypoalbuminemia, and altered volume of distribution. • Sufentanil and Propofol have extrahepatic metabolism. • Cisatracurium or atracurium
- 42. • A rapid-sequence induction is often warranted • Postinduction hypotension may occur as a result of the very low systemic vascular resistance and relative hypovolemia of these patients. • Avoid Halothane.
- 43. • After induction get advanced venous access • Correction of severe coagulopathy before line placement may be considered • Intraarterial line, central venous cannulation, pulmonary artery catheter, large bore i.v cannulas • Cardiac output monitoring
- 46. Ventilatory monitoring:• Inspired/ expired gas oxygen • Vapour monitoring- Isoflurane/ Sevoflurane • Airway pressure • End tidal CO2- changes in pulmonary blood flow ( cardiac output) to detect air embolism • Minute ventilation
- 47. ICP MONITORING • It is indicated in patients with severe encephalopathy and is initiated in the ICU to determine the need for and assess response to therapies like hyperventilation, osmotic diuresis and barbiturate administration. • Persistence of increased ICP and reduced CPP despite such therapies may preclude LT, particularly because ICP has been shown to increase following reperfusion of the liver graft.
- 48. • An orogastric/nasogastric tube is placed to decompress the stomach and improve surgical exposure. • Before the incision is made, appropriate antibiotic and immunosuppressive (e.g., steroid administration) coverage should be ensured. • Maintain normothermia (prolonged exposure, major fluid shifts, and the implantation of a cold organ)
- 49. Blood sampling:TEG, ABG analysis including electrolytes, blood glucose, haemoglobin – – – – – – – – Baseline Hourly in pre anhepatic phase 15 minutes before anhepatic 1 hour into anhepatic 5 minutes before reperfusion 15 minutes after reperfusion Hourly after reperfusion in OT Post operatively in Liver ICU ENSURE TO PREVENT HEPARIN CONTAMINATION FOR TEG
- 50. Maintainence • A balanced technique using volatile anesthetics in an oxygen/air mixture and opioids results in stable intraoperative hemodynamics. • A combination of opioids and BDZ and TIVA with propofol also have been used for liver transplantation. • N2Oshould not be used to avoid intestinal distention, and because in selected cases (not always predictable) a Roux-enY choledochojejunostomy is done at the end of the procedure.
- 51. • Significant coagulopathy, blood loss, and electrolyte and metabolic derangements require frequent intraoperative laboratory tests. • Measurement of ABG, blood glucose, electrolytes (sodium, potassium, and ionized calcium), and Hct is routine in most transplant centers. • Monitoring of ABG allows one to assess oxygenation and base deficits and possibly lactate levels. • Correction of the base deficit and reduction in lactate levels may be indirect indicators that the donor liver is functioning adequately.
- 52. • Glucose metabolism may worsen during liver transplantation, and progressive hyperglycemia may ensue, especially in the reperfusion phase. • Several mechanisms have been implicated, including enhanced glycogenolysis by the donor liver, decreased glucose use, and insulin resistance
- 53. • The PT,INR, PTT, fibrinogen, and platelets are measured by – Thromboelastography – Activated clotting time • Severe coagulopathy and intraoperative blood loss remain the most significant problems
- 54. • The administration of FFPs, RBCs, platelets, and cryoprecipitate remains the mainstay of therapy for blood loss and coagulopathy during liver transplantation. • Aprotinin, aminocaproic acid, tranexamic acid, and conjugated estrogen • Recombinant factor VIIa
- 55. Dissection phase • The surgical goals of the dissection phase are to mobilize the vascular structures around the liver • Manipulation of the liver and sudden decompression of the abdomen can cause hypotension • Adequate fluid replacement is essential
- 56. • Diuresis should be maintained with mannitol / dopamine/ fenoldopa/loop diuretics • During the end of the dissection stage, the donor organ, which is stored in preservation solution, is flushed with crystalloid or colloid solution on a separate table
- 57. Anhepatic phase • During the anhepatic stage, the new liver is primarily implanted by either Infracaval Interposition Or Piggyback Technique. • The choice of surgical technique has important anesthetic implications.
- 58. INFRACAVAL INTERPOSITION • Complete vascular occlusion is established by clamping the hepatic artery, portal vein, infrahepatic vena cava, and suprahepatic vena cava
- 59. • Because the IVC is occluded, cardiac preload becomes dependent on collateral flow • Cardiac output often decreases significantly with an accompanying increased heart rate. • If VVBP is not used, volume loading with a target CVP of 10 to 20 mm Hg and occasionally small infusions of vasopressors (e.g., phenylephrine) are needed before the infrahepatic and suprahepatic caval clamps are placed to prepare for the anhepatic phase.
- 60. • As the response to caval occlusion may differ among patients, a temporary “test clamp” on the IVC may guide management before vascular clamps are permanently placed. • Alternatively, VVBP can be instituted before vascular exclusion of the liver is established. • Bypass is usually accomplished by cannulation of the femoral and portal veins with diversion to the suprahepatic vena cava through the axillary, subclavian, or jugular vein
- 61. • Advantages of VVBP include – – – – – – – improved hemodynamic stability, improved perfusion of organs during the anhepatic phase, decreased red blood cell and fluid requirements, splanchnic decompression, reduced renal impairment, limited metabolic impairment, and a reduced incidence of pulmonary edema • Lymphocele, hematoma, major vascular injury, nerve injury, pulmonary air embolism, and death have been associated with VVBP
- 62. PIGGYBACK TECHNIQUE • The vena cava is partially occluded during the anhepatic phase. • Although improved hemodynamics has been shown, it is considered surgically more difficult than caval interposition, and may lead to greater technical complications.
- 63. • The anhepatic stage begins with excision of the native liver and control of bleeding. • The ice-cold liver donor graft is placed into the surgical field. • The suprahepatic, infrahepatic, and portal vein anastomoses are completed in that order. • The hepatic artery anastomosis can be performed before reperfusion or after restoration of blood flow . • Profound acidosis and hypocalcemia frequently develop during the anhepatic stage, so laboratory parameters should be monitored closely.
- 64. • Fluid management can be challenging, and the return of significant volume when the clamps are released at completion of the vascular anastomoses must be anticipated. • Aggressive fluid management to maintain adequate B.P, may result in fluid overload with possible cardiopulmonary compromise and considerable liver and intestinal swelling. • An engorged liver and intestines may pose a significant technical challenge for the surgeon during the reperfusion phase, especially when performing a Roux-en-Y choledochojejunostomy.
- 65. • At the end of the anhepatic phase, the vascular clamps are removed in staged fashion, and each anastomosis is inspected for leakage. • The return of preload by establishment of continuous caval flow results in normal or supranormal filling pressure. • Removal of the portal vein clamp allows blood flow from the splanchnic circulation into the donor liver and constitutes the BEGINNING OF THE REPERFUSION PHASE. • The most critical part of the reperfusion phase is the period immediately after the vascular clamps are removed from the liver graft. • Significant hemodynamic instability and cardiac arrest can occur within seconds to minutes of unclamping, particularly after unclamping the portal vein.
- 66. • Reduced cardiac contractility, arrhythmias, severe bradycardia, profound hypotension, and hyperkalemic arrest all have been reported, and anesthetic management is directed at maintaining or recovering cardiovascular stability. • This goal may require immediate pharmacologic intervention, such as the administration of epinephrine, atropine, calcium, or occasionally sodium bicarbonate. • Methylene blue has been shown in one small study to attenuate hemodynamic changes of the reperfusion syndrome. • Preoperative placement of external pads may be helpful for immediate postreperfusion cardiac arrest.
- 67. Reperfusion syndrome • The exact mechanism is unknown and remains elusive. – High potassium concentrations in the preservative solution (UW solution), – Donor demographics, – The surgical technique, and – Decreased systemic vascular resistance. – Hypothermia, – Metabolic acidosis, – Endogenous vasoactive peptides from the intestine, and – Sudden atrial stretching in response to unclamping and reperfusion.
- 69. • After the initial reperfusion phase, the hepatic artery anastomosis is completed, the gallbladder is removed, and the bile duct is reconstructed. • Hepatic artery reconstruction is mostly done by end-to-end anastomosis OR by a jump graft from the aorta. • Bile drainage is usually accomplished by choledochocholedochostomy and occasionally by Roux-en-Y choledochojejunostomy. • Attention should be paid to the diagnosis and management of significant coagulopathy and resultant bleeding in the reperfusion phase.
- 70. • Laboratory analysis and clinical evidence of surgical bleeding should guide management of the coagulopathy. • When adequate hemostasis is established, the abdomen is closed. • Hypertension may develop toward the end of the procedure in some patients, and treatment should be initiated before leaving the operating room.
- 71. Hemostatic management Dissection phase:• Intrinsic haemostatic deficiencies can be worsened by iatrogenic haemodilution. • During this stage patients may exhibit enhanced fibrinolytic activity as monitored by TEG.
- 72. ANHEPATIC PHASE • Hyperfibrinolysis is the most striking abnormality and it occurs late during the anhepatic phase and worsens with revascularisation of the new liver. • Frank fibrinolysis with evidence of diffuse bleeding may occur in up to 20% of patients. • Fibrinolysis is caused by abrupt increases in tissue plasminogen activator from graft endothelial cell release and the lack of hepatic clearance during the anhepatic period.
- 73. Treatment • • • • RBCs are transfused to maintain a Hct around 30%. FFP is given to maintain the PT below 1.2-1.5 times normal. Platelets are kept above 50X109 L-1. TEG based coagulation therapy has also been proposed where administration of a fluid mixture of packed cells, FFP`s, and crystalloids in a ratio of 3:2:2.5 for volume replacement. • The infusion of platelets for maximum amplitude less than 40mm; cryoprecipitate for poor clot formation rate and additional FFP for prolonged reaction time(>12min). • Those in favour of this TEG based therapy argue that blood requirements decreased significantly compared to controls.
- 74. Postoperative considerations 1.Post operative bleeding 2.Liver Function – Favourable signs regarding hepatic function in the immediate postoperative period include the following: 1. Hemodynamic stability 2. Awakening from anaesthesia 3. Clearance of lactate 4. Resolution of hypoglycaemia 5. Normalization of coagulation profile (prothrombin time) 6. Resolution of elevated transaminases 7. Good renal function 3.Vascular complications 4.Rejection
- 75. Postoperative care • Postoperative tracheal intubation is no longer mandatory • Fluid shifts or blood loss perse should not be considered an indication for postoperative intubation • Analgesic requirements in patients with ESLD undergoing liver transplantation appear to be significantly decreased compared with other major abdominal surgery
- 76. • Frequent assessment of cardiac and pulmonary function, serum glucose and electrolytes, RFT, LFT, and coagulation and the blood count is crucial. • Patients who have adequate postoperative liver function and have received steroids tend to be hyperglycemic, which may warrant an infusion of insulin.
- 77. THANK YOU
Hinweis der Redaktion
- In addition, the “ceiling” and “floor” effect in terms of the limits set to the laboratory parameters of bilirubin, albumin, and prothrombin time in the grades A, B, and C and changes of serum bilirubin concentrations with therapy (e.g., with ursodeoxycholic acid) do not allow assessment using a continuous scale of severity.
- portal hypertension, which can be defined as portal venous pressure greater than 10 to 12 mm Hg.[Intractable elevated ICP is a significant reason to exclude a patient from transplantation.
- changes in oxygen saturation when changing from the supine to erect positions
- (hepatic venous pressure gradient of 10–12 mm Hg, defined as the pressure gradient between the portal vein and the hepatic vein),
- significant coagulopathy (e.g., dilution and consumption of clotting factors, platelet entrapment, endogenous heparinoid-like substances, primary fibrinolysis