
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Ectopic Pregnancy - Obstetrical & Gynaecological Nursing
Ähnlich wie Ectopic Pregnancy - Obstetrical & Gynaecological Nursing (20)
Mehr von Jaice Mary Joy
Mehr von Jaice Mary Joy (14)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Ectopic Pregnancy - Obstetrical & Gynaecological Nursing
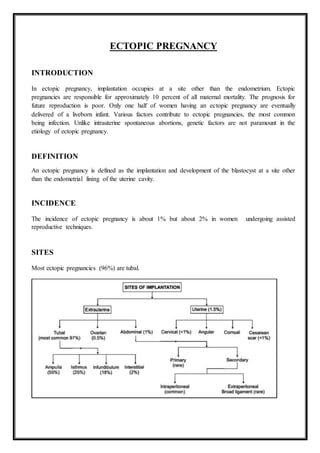
- 1. ECTOPIC PREGNANCY INTRODUCTION In ectopic pregnancy, implantation occupies at a site other than the endometrium. Ectopic pregnancies are responsible for approximately 10 percent of all maternal mortality. The prognosis for future reproduction is poor. Only one half of women having an ectopic pregnancy are eventually delivered of a liveborn infant. Various factors contribute to ectopic pregnancies, the most common being infection. Unlike intrauterine spontaneous abortions, genetic factors are not paramount in the etiology of ectopic pregnancy. DEFINITION An ectopic pregnancy is defined as the implantation and development of the blastocyst at a site other than the endometrial lining of the uterine cavity. INCIDENCE The incidence of ectopic pregnancy is about 1% but about 2% in women undergoing assisted reproductive techniques. SITES Most ectopic pregnancies (96%) are tubal.
- 2. TUBAL PREGNANCY In this condition pregnancy occurs in the fallopian tube. The incidence has increased. The reasons are: increased prevalence of chronic pelvic inflammatory disease, tubal plastic operations, ovulation induction and IUD use. Secondly early diagnosis helps to detect some cases, that in the past, may have resolved spontaneously. Early diagnosis and therapy have helped to reduce maternal deaths due to ectopic pregnancy. The incidence varies from 1 in 300 to 1 in 150 deliveries. ETIOLOGY 1. Infections: - (a) Sexually transmitted infections (STIs) and pelvic inflammatory diseases (PID), due to chlamydia trachomatis (most common) and mycoplasma hominis infection significantly increase the risk of ectopic pregnancy. (b) Postorbital sepsis, puerperal sepsis and appendicitis also increase the risk by causing peritubal adhesions. (c) Genital TB is an important cause in India. 2. Congenital factors like tubal tortuosity, accessory ostia, diverticula and partial stenosis. 3. Salpingitis isthmica nodosa of the tube in which fallopian tube is constricted at various places due to tuberculosis or other infection. 4. Failed contraception: - with contraceptive failure, the relative number of ectopic pregnancies increases. 5. Previous tubal surgery like tuboplasty, salpingotomy, tubal recanalization, etc, can predispose to ectopic pregnancy. 6. Assisted reproductive technology: - Ovulation induction and in vitro fertilization and embryo transfer are associated with 5% risk of ectopic pregnancy and 1% risk of heterotopic pregnancy. 7. Previous ectopic: - After one ectopic pregnancy, there is a 10% risk of having a second ectopic pregnancy. After two ectopics risk increases to 25%. Fate of ectopic pregnancy: - Intraperitoneal bleeding Extraperitoneal bleeding with broad ligament hematoma Secondary abdominal pregnancy
- 3. Mode of termination of tubal pregnancy CLINICAL TYPES OF ECTOPIC PREGNANCY The clinical types are correlated with the morbid pathological changes in the tube subsequent to implantation and the amount of intraperitoneal bleeding. Three types are described: 1. Acute 2. Unruptured 3. Subacute (chronic or old) ACUTE ECTOPIC An acute ectopic is fortunately less common (about 30%) and it is associated with cases of tubal rupture or tubal abortion with massive intraperitoneal hemorrhage. Patient profile The incidence is maximum between the age of 20 years and 30 years, being the maximum period of fertility. The prevalence is mostly limited to nulli- parity or following long period of infertility. Mode of onset The onset is acute. The patients, however, have got persistent unilateral uneasiness in about one-third of cases before the acute symptoms appear. Symptoms The classic triad of symptoms of disturbed tubal pregnancy are: Abdominal pain (100%) Amenorrhea (75%)
- 4. Vaginal bleeding (70%). UNRUPTURED TUBAL ECTOPIC PREGNANCY High degree of suspicion and an ectopic conscious clinician can only diagnose the entity at its preculture state. The physician should include ectopic pregnancy in the differential diagnosis when a sexually active female has abnormal bleeding and/or abdominal pain. Symptoms Presence of delayed period or spotting with features suggestive of pregnancy. Uneasiness on one side of the flank which is continuous or at times colicky in nature. Signs Bimanual examination: Uterus is usually soft showing evidence of early pregnancy. A pulsatile small, well-circumscribed tender mass may be felt through one fornix separated from the uterus. Investigations: With the advent of transvaginal sonography (TVS), highly sensitive radio- immunoassay of b- hCG and laparoscopy, more and more ectopics are now diagnosed in unruptured state. CHRONIC OR OLD ECTOPIC Onset The onset is insidious. The patient had previous attacks of acute pain from which she had recovered or she had chronic features from the beginning. Symptoms 1. Amenorrhoea Amenorrhoea of 5-8 weeks or a few days delayed period or slight bleeding on the expected date of the menstrual period is present in 75% cases. In interstitial pregnancy, amenorrhoea may exceed 10-14 weeks. 2. Pain Pelvic and abdominal pain seen in 95% cases. Pain may be sharp & tearing in nature and pain due to tubal distension, tubal spasm or peritoneal irritation due to bleeding. Pain may be referred to the shoulder due to diaphragmatic irritation by blood (Danforth’s sign). 3. Irregular vaginal bleeding: (70%) History of passage of a fleshy mass (decidual cast) vaginally. Abdominal pain precedes in 80% cases. Most women with ectopic have triad of amenorrhoea, abdominal pain and vaginal bleeding. 4. Vasomotor symptoms: like nausea, vomiting, fainting, dizziness and light headedness may be present due to blood loss and blood in peritoneal cavity.
- 5. 5. Other symptoms: Features of bladder irritation like dysuria Frequency or even retention of urine Rise of temperature due to infection On examination: 1. The patient looks ill. 2. Pallor varying degree is present. 3. Pulse persistently high even during rest—a conspicuous finding. 4. Features of shock are absent. 5. Temperature may be slightly elevated to 38°C. 6. Abdominal examination: Tenderness and muscle guard on the lower abdomen especially on the affected side are a striking feature. A mass in the lower abdomen may be felt which is irregular and tender. Cullen‘s sign—Dark bluish discoloration around the umbilicus, if found, suggests intraperitoneal hemorrhage. 7. Bimanual examination is painful and reveals: Vaginal mucosa—pale. Uterus seems to be normal in size or bulky, often incorporated in the mass occupying the pelvis. Extreme tenderness on movement of the cervix. An ill-defined, boggy and extremely tender mass is felt through the posterolateral fornix extending to the pouch of Douglas. The mass may push the uterus to the opposite side. 8. Rectal examination corroborates the pelvic findings. 9. Examination under anaesthesia (EUA) is helpful to evaluate the pelvic findings but accidental tubal rupture may be provoked during manipulation. Moreover, the diagnostic features of pain on examination and tenderness on moving the cervix (cervical excitation pain) cannot be elicited. INVESTIGATIONS 1. Routine blood examination should be done for: Haemoglobin ABO or Rh grouping Total white cell count and differential count. There may leucocytosis (upto 30,000/mL). ESR: ESR may be high. 2. Human chorionic gonadotropin assays: Current serum and urine pregnancy tests that use enzyme-linked immunosorbent assays (ELISA) are sensitive to levels of 10-20 mIU/mL of hCG and are positive in over 99% of ectopic pregnancies. A negative test usually rules out ectopic pregnancy.
- 6. 3. Ultrasound imaging: Ultrasonic imaging is very important to confirm the clinical diagnosis of suspected ectopic gestation, its size and its location. Transvaginal ultrasonography (TVS) is the modality of choice for its diagnosis. The following pictures may be seen in an ectopic pregnancy - a) An empty uterus. b) An adnexal mass c) There may be slight fluid in the cul-de-sac due to leaking from an unruptured ectopic. d) Bagel sign is a gestational sac in the adnexa surrounded by a hyperechoic ring. Foetal heart in adnexal mass can be seen in 10% cases. e) Colour Doppler will add to the diagnostic accuracy by showing increased vascularity (ring-of-fire pattern). f) The corpus luteum is usually on the same side in an ectopic and may be a clue to diagnosis. 4. Laparoscopy: Laparoscopy is gold standard in diagnosis of ectopic pregnancy and should only be employed in a hemodynamically stable patient. 5. Laparotomy: Laparotomy offers benefit when the diagnosis is in doubt though laparoscopy is usually done for such cases these days. MANAGEMENT OF ECTOPICPREGNANCY Management of ectopic pregnancy (in uncommon locations) has evolved from a radical operative approach (salpingectomy) to a more conservative surgical or medical treatment. However, the type of treatment must be individualized and depends more on clinical presentation. ACUTE ECTOPIC 1. Antishock treatment: Antishock measures are to be taken energetically with simultaneous preparation for urgent laparotomy. Ringer’s solution (crystalloid) is started. Blood transfusion. After drawing the blood samples for grouping and cross matching, volume replacement with colloids (hemaccel) is to be done. 2. Laparotomy: Indications of laparotomy are: Patient hemodynamically unstable. Laparoscopy contraindicated. Evidence of rupture. The principle in laparotomy is “quick in quick out”. CHRONIC ECTOPIC All cases of chronic or suspected ectopic are to be admitted as an emergency. The patient is kept under observation, investigations are done and the patient is put up for laparotomy. Usually a pelvic hematocele is found. Blood clots are removed. The affected tube is identified and salpingectomy is commonly done.
- 7. UNRUPTURED TUBAL PREGNANCY EXPECTANT MANAGEMENT: Where only observation is done hoping spontaneous resolution. Indications are: Initial serum hCG level less than 1,000 IU/L and the subsequent levels are falling. Gestation sac size less than 4 cm. No foetal heart beat on TVS. No evidence of bleeding or rupture on TVS. CONSERVATIVE MANAGEMENT: May be either medical or surgical. Otherwise salpingectomy is done. The advantages of conservative management are: Significant reduction in operative morbidity. Improved chance of subsequent intrauterine pregnancy. Less risk of recurrence. Medical management: 1. Number of chemotherapeutic agents have been used either systemic or direct local (under sonographic or laparoscopic guidance) as medical management of ectopic pregnancy. 2. The drugs commonly used for salpingocentesis are: Methotrexate Potassium chloride Prostaglandin (PGF2α) Hyperosmolar glucose or actinomycin. 3. The patient must be: Hemodynamically stable. Serum hCG level should be less than 3,000 IU/L. Tubal diameter should be less than 4 cm without any foetal cardiac activity. There should be no intra-abdominal hemorrhage. For systemic therapy, a single dose of methotrexate (MTX) 50 mg/M2 is given intramuscularly. 4. Monitoring is done by measuring serum b-hCG on day 4 and day 7. When the decline in hCG between day 4 and day 7 is greater than or equal to 15%, patient is followed up weekly with serum hCG until hCG less than 10 mIU/mL. If the decline is less than 15%, a second dose of MTX 50 mg/M2 is given on day 7. 5. Variable dose methotrexate (MTX) includes: MTX – 1 mg/kg IM on day 1,3,5,7 Leucovorin 0.1 mg/kg IM on day 2,4,6,8 Serum b-hCG is monitored weekly until less than 5.0 mIU/mL.
- 8. Conservative Surgery: Indications: a. Cases not fulfilling the criteria of medical therapy. b. Cases where b-hCG levels are not decreasing despite medical therapy. c. persistent foetal cardiac activity. Different types of conservative surgery - 1. Linear Salpingostomy: A longitudinal incision is made on the antimesenteric border directly over the site of ectopic pregnancy. After removing the products (by fingers, scalpel handle or by suction), the incision line is kept open to be healed later on by secondary intention. Haemostasis is achieved by electrocautery or laser. 2. Linear Salpingotomy: The procedures are the same as those of salpingostomy. But the incision line is closed in two layers with 7-0 interrupted vicryl sutures. This is not commonly done. 3. Segmental Resection: This is of choice in isthmic pregnancy. End-to-end anastomosis can be done immediately or at a later date after appropriate counselling of the patient. 4. Fimbrial Expression: This is ideal in cases of distal ampullary (fimbrial) pregnancy. Salpingectomy is done when (i) whole of the affected tube is damaged (ii) contralateral tube is normal (iii) future fertility is not desired. Following conservative surgery or medical treatment, estimation of b-hCG should be done weekly till the value becomes less than 5.0 mlU/mL. Additional monitoring by TVS is preferred. Following laparoscopic salpingostomy, persistent ectopic pregnancy ranges between 4% and 20%. Persistent ectopic pregnancy is due to incomplete removal of trophoblast. It is high after fimbrial expression and in cases where initial serum b-hCG level is greater than 3,000 IU/L. Prophylactic single dose MTX (1 mg/kg) IM is effective to resolve the problem. PREVENTION OF RECURRENCE OF TUBAL PREGNANCY Incidence of subsequent intrauterine pregnancy (IUP) is 60–70%, in women with unruptured tubal ectopic pregnancy treated by conservative surgery. The incidence of subsequent ectopic pregnancy is about 10–20% and successful conception is about 60%. Salpingostomy done for unruptured tubal ectopic pregnancy does not increase the risk of ectopic pregnancy compared to salpingectomy. Conservative surgery for unruptured tubal ectopic pregnancy is beneficial. Future advice: Main concern is the risk of recurrence. Whenever there is amenorrhea, pregnancy test is done and if positive, high resolution TVS is done to know the site of pregnancy.
- 9. SUMMARY An ectopic pregnancy is an extrauterine pregnancy. The majority occur in the fallopian tube, but other possible sites include cervical, interstitial (also referred to as cornual), hysterotomy (caesarean) scar, intramural, ovarian, or abdominal. This topic included introduction and definition of ectopic pregnancy, sites of ectopic pregnancy, clinical types of ectopic pregnancy, investigation, signs & symptoms and management of the ectopic pregnancy. CONCLUSION Ectopic pregnancy is a known complication of pregnancy that can carry a high rate of morbidity and mortality when not recognized and treated promptly. An ectopic pregnancy occurs when foetal tissue implants outside of the uterus or attaches to an abnormal or scarred portion of the uterus. Ectopic pregnancies carry high rates of morbidity and mortality if not recognized and treated promptly. Risk factors associated with ectopic pregnancies include advanced maternal age, smoking, history of ectopic pregnancy, tubal damage or tubal surgery, prior pelvic infections, IUD use, and assisted reproductive technologies. Ectopic pregnancies may present with pain, vaginal bleeding, or more vague complaints such as nausea and vomiting. With the use of transvaginal ultrasound and serial beta- hCG, and in some cases uterine curettage, most ectopic pregnancies can be diagnosed and treated at an early stage. Medical treatment of ectopic pregnancy with methotrexate avoids surgery and, in properly selected patients, is highly successful and well tolerated.
- 10. BIBLIOGRAPHY 1. Textbook of obstetrics, D.C.Dutta, new central book agency, 2015, 8th edition, page no. 207- 221. 2. Comprehensive textbook of midwifery & gynaecological nursing, Annamma Jacob, 2012, 5th edition, page no. 220-223. 3. Midwifery and obstetrical nursing, J B Sharma, 2015, 1st edition, page no.236-242. 4. https://www.webmd.com/baby/pregnancy-ectopic-pregnancy#1 5. https://www.healthline.com/health/pregnancy/ectopic-pregnancy 6. https://www.ncbi.nlm.nih.gov/books/NBK539860/