Point-of-care test for TB based on immunodominant peptides of M. tb cell-wall proteins
1. Point of care test for TB based on imm nodominant peptides of M tb cell all proteinsPoint‐of‐care test for TB based on immunodominant peptides of M. tb cell‐wall proteinsPoint of care test for TB based on immunodominant peptides of M. tb cell wall proteins
Jesus M Gonzalez2 Sherri T Burda3 Bryan Francis R Sam Niedbala1,2 Suman Laal1, 3, 4Jesus M. Gonzalez2, Sherri T. Burda3, Bryan Francis, R. Sam Niedbala1,2, Suman Laal1, 3, 4
1TB Biosciences, 205 Webster Street, Bethlehem, PA, 2Lehigh University, Department of Chemistry, Bethlehem, PA, TB Biosciences, 205 Webster Street, Bethlehem, PA, Lehigh University, Department of Chemistry, Bethlehem, PA,
3V Aff i M di l C N Y k H b H l h C S N Y k NY 3Veterans Affairs Medical Center, New York Harbor Health Care System, New York, NY, , y , , ,
4New York University Langone Medical Center Departments of Pathology and Microbiology New York NY4New York University Langone Medical Center, Departments of Pathology and Microbiology, New York, NYy g p gy gy
b1. Abstract 2 Background1. Abstract 2. Backgroundg
( )The need for an accurate rapid simple and affordable point‐of‐care (POC) test for The need for an accurate, rapid, simple and affordable point of care (POC) test for
Tuberculosis (TB) that can be implemented in peripheral health‐care settings Tuberculosis (TB) that can be implemented in peripheral health care settings
remains unmet The WHO has recommended that the current commercial rapid remains unmet. The WHO has recommended that the current commercial rapid
diagnostic TB tests not be used since they fail to achieve adequate sensitivity diagnostic TB tests not be used since they fail to achieve adequate sensitivity
and/or specificity We have earlier reported the identification of highly and/or specificity. We have earlier reported the identification of highly g
immunogenic cell wall proteins of M tuberculosis (M tb; PTRP LipC PPE55) immunogenic cell–wall proteins of M. tuberculosis (M.tb; PTRP, LipC, PPE55). g p ( p )
Epitope mapping of these proteins delineated their immunodominant regions Epitope mapping of these proteins delineated their immunodominant regions. p p pp g p g
Antibodies raised against these epitopes seem to be associated to active TB and Antibodies raised against these epitopes seem to be associated to active TB and g p p
t t l t t TB BCG i ti Th tid l id high ifi it i not to latent TB or BCG vaccination. These peptides also provide high specificity in p p p g p y
h h ld t t f i f ti TB ti t d i ti t ith t b l i household contacts of infectious TB patients and in patients with non‐tuberculosis p p
l di W h d l d t t id l t l fl t t b d lung diseases. We have now developed a prototype rapid lateral‐flow test based lung diseases. We have now developed a prototype rapid lateral flow test based
i f h id Th id j d i i i on nine of these peptides. The peptides were conjugated to a carrier protein using on nine of these peptides. The peptides were conjugated to a carrier protein using
d d / l h f ll d b l fstandard EDC/NHS coupling chemistry followed by size exclusion purification. standard EDC/NHS coupling chemistry followed by size exclusion purification.
Peptide conjugation was confirmed using MALDI‐MS after which the proteins Peptide conjugation was confirmed using MALDI MS after which the proteins
were adsorbed onto colloidal gold and also striped onto nitrocellulose The assay were adsorbed onto colloidal gold and also striped onto nitrocellulose. The assay
parameters were adjusted to determine positive/negative status within 15 minutes parameters were adjusted to determine positive/negative status within 15 minutes
The Tuberculosis infection can be described in terms of stages:via visual or instrumented assessment The prototype lateral flow assay was The Tuberculosis infection can be described in terms of stages:via visual or instrumented assessment. The prototype lateral flow assay was g
St g 1 l t t TB li i l t t th i f ti i d t t bl tested with sera samples from 124 smear positive TB patients and 47 healthy PPD+ Stage 1: latent TB, no clinical symptoms are present, the infection is undetectable tested with sera samples from 124 smear‐positive TB patients and 47 healthy PPD+ g , y p p ,
t thi i tor PPD subjects from India a TB endemic country to confirm continued at this point.or PPD‐ subjects from India, a TB‐endemic country, to confirm continued p
St E th h th b t i l b d h i d lt f l i ld discrimination between TB patients and non TB controls The individual sensitivity Stage 2: Even though the bacterial burden has increased, culture of samples yield discrimination between TB patients and non‐TB controls. The individual sensitivity Stage 2: Even though the bacterial burden has increased, culture of samples yield
i l
p y
achieved with each peptide ranged from 27% to 86% A combinatorial analysis of negative results.achieved with each peptide ranged from 27% to 86%. A combinatorial analysis of negative results.
h h f b d d b l l b
p p g 7 y
the res lts as performed and a sensiti it of 98% as obtained ith onl three of Stage 3: At this point the infection can be detected by culture samples or by the results was performed and a sensitivity of 98% was obtained with only three of Stage 3: At this point the infection can be detected by culture samples or by p y 9 y
th tid d Th i iti l lt d t t th f ibilit f d i i g sophisticated techniques such as Nucleic acid amplification teststhe peptides used. These initial results demonstrate the feasibility of devising a sophisticated techniques such as Nucleic acid amplification tests.p p y g
id POC TB t t th t i b d f ll l t d i d i t tid Stage 4: Smear examination detect 50% of the cases at this stage chest X‐rays rapid POC TB test that is based on carefully selected immunodominant peptides Stage 4: Smear examination detect 50% of the cases at this stage, chest X rays p O o y o o p p
f M b ll ll i can result in positive identification as wellof M. tb cell‐wall proteins. can result in positive identification as well.of M. tb cell wall proteins.
4 Rapid test goals3 Diagnosis in developing countries 4. Rapid test goals3. Diagnosis in developing countries 4 p gg g
Rapid diagnosis of TB is essential to reducing transmission and mortality in Rapid diagnosis of TB is essential to reducing transmission and mortality in Devise a simple, accurate and affordable TB test p g g y
de eloping co ntries here 90% of the estimated nine million cases of TB occ r
Devise a simple, accurate and affordable TB test
developing countries, where 90% of the estimated nine million cases of TB occur. that meets the WHO specifications for a test that p g , 9
I th l ti li i l i i i i i ti f d
that meets the WHO specifications for a test that
In these locations clinical suspicion, microscopic examination of smears made can replace sputum smear microscopy p , p
di tl f th t l f id f t b illi (AFB) d i ll
can replace sputum smear microscopy.
directly from the sputum samples for acid fast bacilli (AFB), and occasionally y p p ( ), y
h t X i th t id l d di ti t l S i chest X‐rays, remain the most widely used diagnostic tools. Smear microscopy, chest X rays, remain the most widely used diagnostic tools. Smear microscopy,
h h f i i ( i i h lf f ) di ithough fast, is too inaccurate (missing over half of cases), tedious, time though fast, is too inaccurate (missing over half of cases), tedious, time
d f l l hconsuming and requires examination of multiple specimens . In settings with consuming and requires examination of multiple specimens . In settings with
ample resources TB diagnosis has been based on smears made from ample resources, TB diagnosis has been based on smears made from Microscopic examination of smear
decontaminated and concentrated specimens culture of bacteria and nucleic
p
made directly from sputum of patient decontaminated and concentrated specimens, culture of bacteria and nucleic made directly from sputum of patient
f f bacid‐amplification tests (NAAT) for almost two decades While these technologies for presence of bacteria. acid‐amplification tests (NAAT) for almost two decades. While these technologies p
are far more sensitive than the direct sputum smear used routinely in TB‐endemic are far more sensitive than the direct sputum smear used routinely in TB‐endemic
settings the required laboratory infrastructure trained personnel and high settings, the required laboratory infrastructure, trained personnel and high
patient burden makes their implementation unrealistic in resource limited patient‐burden makes their implementation unrealistic in resource‐limited p p
environments Additionally mycobacterial culture which is the gold standard environments. Additionally, mycobacterial culture, which is the gold standard y, y , g
for TB diagnosis is slow taking from two to eight weeks to produce a definitive for TB diagnosis, is slow, taking from two to eight weeks to produce a definitive g , , g g p
lt Th i i t t d id gh f di g i results. Thus, microscopy is not accurate and rapid enough for proper diagnosis , py p g p p g
f TB i l li i ith HIV d i hild d th of TB, even more so in people living with HIV and in children, and other Desired Performance, p p g ,
t h i h b t i l lt d NAAT ith t l i
Desired Performance
techniques such as mycobacterial culture and NAAT are either too slow, require > 95% sensitivity in smear positive TB patientstechniques such as mycobacterial culture and NAAT are either too slow, require
hi i d i f b h
> 95% sensitivity in smear positive TB patients
sophisticated infrastructure or both > 60% sensitivity in smear negative TB patientssophisticated infrastructure or both
l fi k b i h d i f i
> 60% sensitivity in smear negative TB patients
Currently, five key barriers to the detection of TB exist: > 98% specificity (individuals with LTBI Non TB Currently, five key barriers to the detection of TB exist: > 98% specificity (individuals with LTBI, Non TB
1. The difficulty of distinguishing between latent TB infection and active TB Mycobacterial diseases other lung diseases OLD)1. The difficulty of distinguishing between latent TB infection and active TB Mycobacterial diseases, other lung diseases OLD)
disease by other immunological tests
y g )
disease by other immunological tests
2 The lack of validated accessible and rapidly testable biomarkers Minimum Performance2. The lack of validated, accessible, and rapidly testable biomarkers Minimum Performance
3 Long delays in accurate diagnosis before patients can get treatment 90% iti it i iti TB ti t3. Long delays in accurate diagnosis before patients can get treatment Chest X‐ray: radiological > 90% sensitivity in smear positive TB patients
4 Lack of an accurate lab free point of care (POC) test
Chest X ray: radiological
i ti f l
9 y p p
% ifi it (i di id l ith LTBI NTM OLD)4. Lack of an accurate, lab‐free point‐of‐care (POC) test examination of lungs. > 95% specificity (individuals with LTBI, NTM, OLD)
5 The unavailability of facilities that can test for drug resistance
g 95 p y ( , , )
5. The unavailability of facilities that can test for drug resistance.g
5 R lt5. Results
6 C bi i l l i
5 esu ts
6. Combinatorial analysis
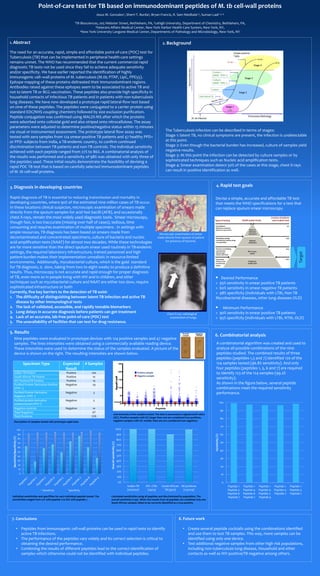
Nine peptides were evaluated in prototype devices with 124 positive samples and 47 negative
6. Combinatorial analysis
Nine peptides were evaluated in prototype devices with 124 positive samples and 47 negative g
samples The lines intensities were obtained using a commercially available reading device A combinatorial algorithm was created and used to samples. The lines intensities were obtained using a commercially available reading device. A combinatorial algorithm was created and used to p g y g
These intensities were used to determine the status of the samples evaluated A picture of the analyze all possible combinations of the nine These intensities were used to determine the status of the samples evaluated. A picture of the analyze all possible combinations of the nine p p
device is shown on the right The resulting intensities are shown below peptides studied The combined results of three device is shown on the right. The resulting intensities are shown below. peptides studied. The combined results of three g g p p
peptides (peptides 1 3 and 7) identified 120 of the peptides (peptides 1,3 and 7) identified 120 of the
S i T E t d # S l
p p (p p ,3 7)
124 samples tested (96 8% sensitivity) And only Specimen Type Expected # Samples 25 124 samples tested (96.8% sensitivity). And only Specimen Type Expected
l
# Samples 4 p (9 y) y
f tid ( tid 1 3 6 d 7) i d Result four peptides (peptides 1, 3, 6 and 7) are required Result
I di TB P ti t P iti 20 P i i l
p p (p p , 3, 7) q
t id tif f th l ( % Indian TB Patient Positive 100 20 Positive sample to identify 123 of the 124 samples (99.2%
South African TB Patient Positive 10
ff
Negative sample
y 3 4 p (99
iti it ) South African TB Patient Positive 10
15
toff
g p
sensitivity).
HIV Positive/TB Positive Positive 14 15
Cut
sensitivity).
A h i h fi b l l id
HIV Positive/TB Positive Positive 14
P ifi d P t i D i ti P iti N g ti
al/C
As shown in the figure below, several peptide Purified Protein Derivative Positive Negative 29
gna
As shown in the figure below, several peptide
b h d(PPD +) 10
Sig
combinations meet the required sensitivity (PPD +)
S
combinations meet the required sensitivity
Purified Protein Derivative Negative 3 performance
Negative (PPD )
g 3
5
performance.
Negative (PPD ‐) 5
Purified protein derivative Negative 5Purified protein derivative
d t i d (PPD ?)
Negative 5
0
Cutoff 100undetermined (PPD ?) 1 1 2 2 3 3 4 4 5 5 6 6 7 7 8 8 9 9
0 100( )
Negative controls Negative 10
1 1 2 2 3 3 4 4 5 5 6 6 7 7 8 8 9 9
P tidNegative controls Negative 10 Peptide
90
Total Negatives 47
90
Total Negatives 47
l 12
Line intensity of the samples tested. The data is presented as signal/cutoff ratios
Total Positives 124
y p p g /
(S/C) Positive samples with S/C larger than one are considered true positives 8(S/C). Positive samples with S/C larger than one are considered true positives,
ti l ith S/C ll th id d t ti
80
Description of samples tested with prototype rapid tests negative samples with S/C smaller than one are considered true negatives.Description of samples tested with prototype rapid tests
70
100 100%
70
100 100%
90 90% 60
)
90
)
90% 60
(%)
80
(%)
80%
y (
80
y (
80%
)
vity
70
city
%
%)
50
tiv
7
fic
70%
y (
sit
60
cif
tiy
en
pec
60%
vit
40
Se
50
Sp
60%
itiv
40
40
ty/
50%
nsi
40
vit
50%
sen
30
30
tiv
40%
l s
30
30
nsit
40%
ral
20
en
%
er
20
Se
30%
Ove
20
10
O
20%
0 10
10%
10
10%
0% 00% 0
Indian TB HIV +/TB+ South African All positives Peptide 1‐ Peptide 1‐ Peptide 1‐ Peptide 1‐ Peptide 1‐
S iti it S ifi it (100/100)
/
(14/14) TB (9/10)
p
(123/124)
Peptide 1
Peptide 3
Peptide 1
Peptide 4
Peptide 1
Peptide 4
Peptide 1
Peptide 4
Peptide 1
Peptide 3Sensitivity Specificity (100/100) (14/14) TB (9/10) (123/124) Peptide 3‐ Peptide 4‐ Peptide 4‐ Peptide 4‐ Peptide 3‐
Peptide 6‐ Peptide 6‐ Peptide 7‐ Peptide 7 Peptide 7
Individual sensitivities and specifities for each individual peptide tested The Calculated sensitivities using all peptides and discriminated by population The
Peptide 6
Peptide 7
Peptide 6
Peptide 7
Peptide 7
Peptide 9
Peptide 7 Peptide 7
Individual sensitivities and specifities for each individual peptide tested. The
sensitivities ranged from 27% with peptide 2 to 86% with peptide 7
Calculated sensitivities using all peptides and discriminated by population. The
overall sensitivity is 99% When the results from all peptides are combined only one
Peptide 7 Peptide 7 Peptide 9
sensitivities ranged from 27% with peptide 2 to 86% with peptide 7. overall sensitivity is 99%. When the results from all peptides are combined only one
South African samples failed to be correctly identified as a true positive.p y p
7 Conclusions 8 Future work7. Conclusions 8. Future work
• Peptides from immunogenic cell wall proteins can be used in rapid tests to identify • Create several peptide cocktails using the combinations identified • Peptides from immunogenic cell‐wall proteins can be used in rapid tests to identify • Create several peptide cocktails using the combinations identified p g p p y
ti TB i f ti
p p g
d th t t t TB l Thi l b active TB infections. and use them to test TB samples. This way, more samples can be
Th f f th tid id l d it t l ti i iti l t
p y, p
id tifi d i l d i• The performance of the peptides vary widely and its correct selection is critical to identified using only one device.p p p y y
bt i i th d i d f
g y
T t dditi l ti l f th hi h i k l ti obtaining the desired performance. • Test additional negative samples from other high risk populations, obtaining the desired performance.
C bi i h l f diff id l d h id ifi i f
Test additional negative samples from other high risk populations,
i l di b l i l di H h ld d h • Combining the results of different peptides lead to the correct identification of including non‐tuberculosis lung disease, Household and other Combining the results of different peptides lead to the correct identification of
l h h h ld b d f d h d d l d
including non tuberculosis lung disease, Household and other
ll i i / i hsamples which otherwise could not be identified with individual peptides. contacts as well as HIV positive/TB negative among others.samples which otherwise could not be identified with individual peptides. contacts as well as HIV positive/TB negative among others.