
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (19)
Ähnlich wie In vivo effects of Interleukin 2 on Lymphocyte Subpopulations in a Patient with a Combined Immunodefciencyi
Ähnlich wie In vivo effects of Interleukin 2 on Lymphocyte Subpopulations in a Patient with a Combined Immunodefciencyi (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
In vivo effects of Interleukin 2 on Lymphocyte Subpopulations in a Patient with a Combined Immunodefciencyi
- 1. Immunobiol., vol. 167, pp. 452-461 (1984) 1 Universitats-Kinderklinik Tiibingen, Tiibingen, 2 Medizinische Hochschule Hannover, Hannover, and 3 GBF _ Gesellschaft fur Biotechnologische forschung mbH, Braunschweig, Federal Republic of Germany In vivoEffects ofInterleukin 2 on Lymphocyte Subpopulations in a Patient with a Combined Immunodeficiency* R. DOPFER', D. NIETIIAMMER', H. H. PETER', E.-M. KNIEP', D. A. MONNER" and P. F. MDHLRADT' Received April 17, 1984 . Accepted May 29, 1984 Abstract This report describes a clinical trial with Imerleukin 2 (IL-2) on a 17-month old male child with combined immunodeficiency (Nezelof's syndrome). IL-2 was prepared from conditioned media of phytohemagglutinin-stimulated leukocytes from huffy coats. The purification of IL- 2 involved chromatography on Matrex Blue A sepharose and gel filtration chromatography. The preparation was free of macrophage cytotoxicity factor, macrophage migration inhibition factor and colony-stimulating factor. It contained negligible activity of interferon-y_ lL-2 activity was adjusted to 1600 U/ml, which corresponds to about 0.8 Ilg homogeneous IL-2/ml. The patient was treated over a 50-day period with a total dose of 20,000 U IL-2, which was injected subcutaneously. IL-2 was well tolerated. Within 3 weeks, the treatment led to a normalization of a lymphocytosis which had prevailed for the previous 3 months. A pro nounced eosinophilia also improved but did not reach normalleve1s. The most striking effect was a normalization of the OKT4-tIOKT8-t ratio with a concomitant relative increase in OKT3-t cells in the peripheral blood. No effects were seen on E rosette formation, B cell counts or serum Ig levels. Also NK or ADCC activity remained high, as before the treatment. Infectious episodes and requirement for antibiotic treatment were less frequent during IL-2 therapy. Some effects of IL-2 were transient, e.g., the counts of OKT4-t and OKT3-t cells which returned to pathological values a few weeks after the treatment was discontinued. Introduction Interleukin-2 (IL-2) is a lymphokine produced by stimulated helper T cells. IL-2 binds to T cells which have, after antigen or mitogen contact, , Parlially supported by DFG Sachbeihilfe Pe 151 /7-6 (H.H.P.), by BMFT pmject PTB 8372 (E.M.K.), and by BMFT project 8426. Abbreviations: ADCC = antibody-dependent cellular cytotoxicity; ADA = adenosine deaminase; AIDS = acquired immunodeficiency syndrome; BSA = bovine serum albumin; eIg = cellular immunoglobulin; ConA = Concanavalin A; DiY = diphtheria toxin; IL-2 = Interleukin 2; IFN = interferon; LGL = large granular lymphocytes; NK = natural killer; PBMC = peripheral blood mononuclear cells; PHA = phytohemagglutinin; PNP = purine nucleoside phosphorylase; SIg = surface immunoglobulin.
- 2. In vivo Effects of Interleukin 2 . 453 acquired the appropriate receptor. This provides the necessary signal for proliferation of T cells (for reviews see 1,2). IL-2 is, therefore, a prerequis ite for expansion of antigen-specific regulatory and effector T cell clones. Helper T cells playa central role because they provide help for humoral as well as cellular defense mechanisms, and consequently IL-2 also indirectly affects the humoral response by expansion of helper clones. Thus, defects of the pre- or intra-thymic T cell development lead to a severe combined immunodeficiency syndrome affecting both cellular and humoral defense. A number of pathological conditions have been reported in which deficits in IL-2 production are associated with grave immune disorders. In children, defective IL-2 production was found in various primary immunodeficien cies (3), in a child with Nezelof's syndrome (4) and in an infant with pediatric acquired immunodeficiency syndrome (AIDS) (4). In adults, a decreased or absent IL-2 production has been reported in systemic lupus erythematosus (5), angioimmunoblastic lymphadenopathy (6) and in AIDS (7). We describe here the case of a child with a cellular immunodeficiency syndrome, characterized by an elevated number of apparently immature T cells, an abnormally low percentage of mature T cells and, at an advanced stage, a low OKT4/0KT8 ratio. The effects of a 50-day treatment with IL-2 on the T lymphocyte subpopulations are reported. Materials and Methods Production of fL-2 from buffy coat leukocytes Human IL-2 was produced in bioreactors, basically as described (8), but with the following modifications. Lymphocytes were prepared from 24 h buffy coats obtained from the blood bank in Springe, FRG. The isolation of lymphocytes, which will be described in detail elsewhere, included a step in a Hemoneucs blood wash centrifuge to remove the bulk of erythrocytes, precipitation with a plasma expander (Plasmasteril, Fresenius, Bad Homburg, FRG) similar to described procedures (9), and removal of adherent cells with carbonyl iron (10). The resulting leukocyte mixture consists of 70 % lymphocytes, 20 %granulocytes, and 10 % monocytes. These leukocytes were sumulated for 20 h with 2 % PHA (Gibco, Grand lsland, N.Y., USA) in serum-free RPMI 1640 in bioreactors at a cell concentration of 5 x 10'1 ml. Routine preparations contain about 20 U/ml of IL-2 (for definition sec below). Partial purific3.uon of IL-2 2% vlv n-butanol was added as a preservative, media (3000 ml) were adjusted to pH 6.5 with 1 M phosphoric acid, and the mixture passed over a 3 x 12 em column of Matrex Gel Blue A (Amicon, Witten, FRG) at a rate of 100 mllh. 2 %n-butanol was also added to all other buffers used except in the last dialysis step. The column was washed with 300 ml of 150 mM NaCI in 10 mM N';K phosphate buffer pH 6.5, and 300 ml of0.4 M NaCI in the same buffer. This procedure removes the mitogen and about 90 % of the protein. IL-2 activity was then washed off in about 200 ml of buffer containing 1 M NaCI. This eluate was concentrated to 10 mt on PM 10 membranes (Amicon), and subjected to gel chromatography on a 2.6 x 100 em Ultrogel AcA 44 (LKB, Bromma. Sweden) column equilibrated with 0.2 M Tris. 05 M glycine. 2 % n-butanol, adjusted to pH 7.6 with HCl. The flow rate was 15 mllh.
- 3. 454 . R. DOPFER et a1. Fractions eluting at a mol. wt. range of 18,000--22,000 contained IL-2 and were pooled, concentrated on PM 10 membranes to 12 ml after addition of 1% human AB serum, and dialyzed against PBS. The preparations were free of macrophage migration inhibition factor, macrophage cytotoxicity factor and colony stimulating factor, but occasionally contained interferon in titers corresponding to those in untreated conditioned media. The IL-2 activity was adjusted to approx. 1500 U/ml. The preparations were only moderately pyrogenic in the rabbit fever-test. IL-2 rest, defim'tion ofa unir IL-2 activity was tested with murine Con A blasts as responder cells as described (11). An internal standard was always included in the tests. 2000 U, as defined by us, correspond to about 1 Ilg of pure IL-2, as we estimated from highly purified, partially-sequenced IL-2 prepared in our laboratory. Laboratory tests to establish jmmune competence Differential red and white blood cell counts were performed at least twice a week. Peripheral blood mononuclear cells (PBMC) were isolated from heparinized blood by FicolUHypaque density gradient centrifugation. The analysis of lymphocyte markers and functions have been detailed in a previous paper (12), which also contains first admission data of the infant (No.2) described in this report. Briefly, lymphocytes expressing surface membrane Ig (SIg+) were characterized with fluoresceinated F(abh goat anti-human IgG, IgA, IgM antiserum (Behringwerke AG, Mar burg, fRG). B cells showing terminal differentiation were identified by strong cytoplasmic Ig (CIg+) reactivity on methanol-fixed cytocentrifuged smears. The T cell markers included spontaneous rosette formation with neuraminidase-treated sheep erythrocytes (E-rosettes) and staining with the monoclonal reagents OKT3 (pan T cell marker), OKT4 (T helper/inducer phenotype), OKT8 (T suppressor/killer phenotype) and OKTlO (early thymocytes (13), some bone marrow cells (14), and NK cells (15». Fe-receptor bearing lymphocytes were detected by rosette formation with IgG-coated ox erythrocytes (EA-IgG-rosettes). Mitogen and alloanti gen responsiveness were determined in flat-boHom-microculture plates using optimal concen trations of phytohemagglutinin (PHA), concanavalin A (Con A), a lectin-free IL-2, Can A + IL-2 and irradiated allogeneic PBMC (12). Natural killing (NK) and antibody dependent cellular cytotoxicity (ADCC) were measured in 12 hr ~ICr release assays against K562 and Ll210 target cells, respectively (12). The evaluation of the humoral immune response included measurements of serum Ig concentrations by laser nephelometry, isoagglutinin titers and specific antibodies .to candida, bovine serum albumin (BSA) and diphtheria toxin (DiT) (12). Adenosine deaminase (ADA) and purine nucleoside phosphorylase (PNP) were determined in whole blood to exclude genetic defects of the purine salvage pathway known to be associated with severe combined immunodeficiency (16). Results Clinical symptoms and immunological status of the patient A. O. The patient, a boy whose parents were first degree cousins with no family history of immunodeficiency, was hospitalized when five months old because of recurrent infections of the gastro-intestinal and upper and lower respiratory tract. He was slightly underweight and his skin showed signs of eczema and dermatitis. Cervicallymphnodes were enlarged, and X-ray of the thorax revealed no thymus shadow. Biopsy of the skin showed infection
- 4. In vivo Effects of Interleukin 2 . 455 with candida and rod-shaped bacteria. Biopsy of one lymph node revealed granulomas consisting of mast cells, eosinophils and plasma cells, and signs of infection with bacillus of Calmette and Guerin with which the patient had been vaccinated as a newborn. Platelet counts, hemoglobin and serum calcium levels were within normal ranges, which makes the diagnosis of a Wiscott-Aldrich or DiGeorge syndrome unlikely. ADA and PNP blood enzyme activities were normal as Table I. Immunological state of patient A.b. 2 months after hospitalization, January 1982, age 7 months Patient Age-matched healthy controls Blood cells/~l celiS/ILl leukocytes 28000 12200 (6000-17500) lymphocytes 23000 7600 (4000-13500) eosinophils 3600 300 (70-750) platelets 220000 340000 (220 000-460 000) hemoglobin (gil) 122 122 (100-150) CaH (mvalll) 4.7 4.9 (4.6-5.2) Immunoglobulins IgG (gil) 2.8 3.1 (1.2-8.3) IgM (gil) 2.0 0.6 (0.3-1.3) IgA (gil) 1.0 0.3 (0.1-0.6) IgE (IUlml) 38 49 Lymphocyte surface markers % pos. cells % pos. cells SIg <I 2-12 CIg < I 1- 3 OKT 10 63 8-36 OKT3 34 60-80 OKT4 28 4s-{'0 OKT 8 10 18-30 EA-IgG-rosettes 46 3-36 E-rosettes 75 56-85 In viero immune response cpm cpm medium control 400 1500 (300-4600) PHA (5 ~lIml) 2200 170000 (33 000-450 000) Con A (10 ~l!ml) 2400 120000 (16000-470 000) IL-2 6300 12000 (3400-17000) Con A + IL-2 23 300 96000 (40000-200000) allo MLC 300 28000 (3 500-85 000) % spec. ~ICr release % spec. 5lCr release NK a K 562 (16,1. 501, 1,1) 74/58/21 54/25/6 ADCC a L 1210 (25,1, 801, 2,1) 95/86/76 81/59127
- 5. 456 "R, DoPFE> etal. was a chromosomal analysis performed on the patient's PBMe. Leukocytes were high and differential blood counts showed a lymphocytosis and elevated numbers of eosinophils, Serum IgG was low, while IgM, IgA and IgE levels were within the age-matched normal range, Low isoagglutinin titers were present but specific antibodies against candida, BSA or DiT, the latter} months after vaccination with DiT, could not be detected, The majority of the circulating lymphocytes formed E-rosettes and an elevated proportion carried Fc-IgG receptors (46 % EA-IgG rosettes), Serotyping with monoclonal antibodies showed an abnormally high fraction of OKTlO+ cells, whereas the percentage of OKT}+, OKT4+ and OKT8+ cells was diminished, Immature B cells (SIg+) and B cells undergoing terminal differentiation (CIg+) were well below 1% of the isolated PBMe. A similar impairment was found for the lymphoproliferative response towards polyclonal T cell mitogens and alloantigens, However, the strongly diminished Con A-induced lymphoproliferation could be improved by external supply of IL-2, The response to IL-2 without additional mitogens was at the lower margin of the response of healthy controls, Finally, NK and ADCC activities of the patient'S PBMC were both markedly elevated as compared to a control group, These laboratory parameters are sum marized in Table 1. Taken together they all point to a T cell defect as the underlying cause for the patient's combined immunodeficiency. The condi tion may best be classified as a variant of Nezelof's syndrome with lymphocytosis (Fig, 1). - ll - 2 Il - 2 Normal .. Range '- .-----. 20000 .~ i' ~ g ".0 15000w 0 ,,,0 , 0 , , • ".- 10000 ! : , " ""~ " " J ,0 • . " "g- , 1,1 f , , , , :L , :~ , 0 , , , ~ : , °'0, , , E " I' ., ,~ I' oJ • 0 0, ,~ 5000 q ~' '0, j 0 0 7/1/&2 811 911 1011 II/I 12'1 1/1/83 211 3/1 ' " 5/1 DQte Fig. 1. Lymphocyte and eosinophil counts of patient A. O. over a lO-month period which included twO phases of IL-2 treatment.
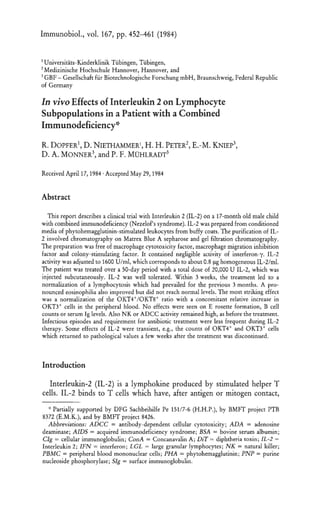
- 6. In vivo Effects of Interleukin 2 . 457 Treatment with II-2 Throughout the time of hospitalization the patient received prophylactic and therapeutical antibiotic treatment including Isoniazid, Colistinsulfate, Flucloxacillin, Ketoconazol, and Trimethoprim-Sulfamethoxazol. A treat ment with thymosin (10 mg twice a week) over 5 months produced no clinical improvement and had neither effects on leukocyte countS nor on lymphocyte markers and functions. Three weeks after thymosin treatment had been stopped, thymus epithelium was transplanted from a child who had undergone cardiac surgery. Again no improvement of the immunologi calor clinical status was noted. A bone marrow transplantation was considered but an HLA-matched sibling was not available and a haplo identical transplantation of bone marrow from the father was refused by the parents. In this situation, informed consent was obtained from the parents to start IL-2 treatment. The treatment was begun when the patient was 17 months old, 4 months after thymosin treatment had been stopped and 3 months after the thymus epithelium transplantation had failed. By this time, the patient had an abnormally low ratio of OKT4+ versus OKTS+ T cells (Fig. 2). 40 % of the lymphocytes were of large granular morphology (LGL), and 69 % of the lymphocytes exhibited the NK cell marker HNKI (17). IL-2 was injected subcutaneously in the inguinal region since it had been shown in animal experiments that IL-2, when injected intravenously, is cleared rapidly from 100 ... 80 ~ •u •> ;; o .. 60 40 20 Status before Il-2 • • • • • • •• Il-2 Injections !IIIIIIIII •, "I, /0---0 OKT 10 ~ .___/ . OKT 3 /X'~'OKT' / ------.~ ___.OKra -.--- Status after Il-2 • •• Normal Range L--L~'~'~~_-L__-L_ _~_,"r-_~___~ 1/14/82 7127 I 10/26 118 11123 12114 211/83 Date 20 • , , • r 15 '3 10 ~ 7 g ~ ;; . x Fig. 2. Lymphocyte counts and percentages of OKT3, OKT4, OKT8, and OKTtO positive lymphocytes during the first IL-2 treatment period. Differential blood cell counts were done with capillary blood. Lymphocyte markers were analyzed on leukocytes isolated from venous blood by a Ficoll/Hypaque gradient centrifugation.
- 7. 458 . R. DOPFER et ,I. the blood (18, 19). 1 ml doses of 1600 U IL-2 were given every 3 to 4 days over a period of 50 days. The only side effect was a mild but inconsistent fever reaction. Within three weeks after beginning of IL-2 treatment, lymphocyte counts, which had been high for the previous 3 months, decreased to and stayed at normal levels. The percentage of LGL had dropped to 14 %. Also eosinophils decreased, but remained at elevated numbers (Fig. I). Before, during, and 50 days after IL-2 treatment, humoral and cellular immune parameters were determined. Part of the results are shown in Fig. 2. It appeared that IL-2 treatment led to an increase of the percentage of OKT4+ and OKT3+ cells and a slight increase of mitogen responsiveness (maximal PHA response 55,400 cpm, maximal ConA response 25,400 cpm). No effect was seen on E- and EA-IgG-rosette formation nor on B cell counts and terminal B cell differentiation. Similarily, serum Ig levels and specific antibody production did not notably change during the IL-2 treatment. The same was true for NK and ADCC activities which remained high during the entire observation period. Several weeks after discontinuation of IL-2 treatment, the percentage of circulating mature T cells was again very low (Fig. 2) and the number of eosinophils had risen (Fig. 2). Upon resumption of IL-2 treatment, eosinophils dropped as during the first period of administration, but rose again towards the end of the 6-week treatment. No immunological data were gathered this time as the drawing of larger volumes of blood was considered too great an inconvenience to the patient. Although difficult to quantitate, there were signs of general improvement of the patient's clinical status while under IL-2 treatment. The infectious episodes, and conse quently the requirement for antibiotic treatment were less frequent during IL-2 therapy. However, the effects of IL-2 appeared of a transient nature. Three months after the last IL-2 treatment the patient's condition wors ened. He died from pneumonia at the age of 26 months. An autopsy was refused by the parents. Discussion All available evidence suggested that the patient A. b. suffered from a combined immunodeficiency (Nezelof's syndrome) due to a T cell defect accompanied by an abnormal proliferation of an immature pre-Tor NK like cell type. Thus, the proportion of lymphocytes showing an immature T or NK cell phenotype (OKTIO+, HNKI +, Fc-IgG receptor+, LGL mor phology) was clearly elevated and functional NK cell activity of the patient's PBMC was also high. In contrast, we observed low percentages of mature T cells expressing OKT3, OKT4, or OKT8 phenotypes. In agree ment with this finding was the severely impaired T cell response to
- 8. In vivo Effects of Interleukin 2 . 459 mitogens which could, however, be partially restored in vitro by the addition of IL-2. This observation and the low percentage of OKT4+ T helper/inducer cells suggested that the defective T cell response was at least partially due to a lack of the patient's IL-2 producing capacity. Since the therapeutic approaches to overcome the T cell differentiation defect by medication with thymosin or transplantation of thymic epithelium had not shown any promising effects, we decided to treat the patient with human IL-2, in the hope of expanding T cells that had acquired IL-2 receptors in response to antigen. Over the first treatment period of 50 days, the pathologically high number of circulating lymphocytes decreased to nearly normal values whereas the percentages, yet not the absolute numbers, of OKT4+ and OKT3+ cells increased in the blood and the OKT4/0KT8 ratio became almost normal. As DE SOUSA has pointed out, the lymphocytes in a sample of peripheral blood represent only a millionth of the total lymphocytes in the body (20), and it is, therefore, impossible to precisely interpret these effects of IL-2 as an expansion of OKT4+ cells, a normalization of a prior maldistribution of lymphocytes (20) or both. In any event, a modest normalization of the immune status is evident, and is further supported by the transient improvement of the responsiveness to T cell mitogens. It has been reported that IL-2 induces in vitro growth and enhancement of activity of murine NK cells (21). Such effects were not observed in our patient, possibly because NK-like, OKTIO+ cells were numerous, and NK activity was high even before IL-2 treatment. IL-2 was well tolerated at the given dose and the subcutaneous route of injection. The patient, weighing 5 kg, was given a total dose of 20,000 U of IL-2 for 50 days. According to our estimation based on the specific activity of a preparation of IL-2 from our laboratory which was pure enough to yield a partial amino acid sequence, 2000 U corresponded to about I I!g of pure IL-2. At a first glance, it appears unlikely that a dose of 10 I!g of a peptide given over a period of 50 days should have any effects at all. It is, however, known that other peptides are biologically active at pg levels (22). Such levels may well have been reached in the lymphatic system under our conditions. Similar doses were used in a brief in vitro trial by FLOMENBERG et al. (4). In this case, post mortem histological data were reported, suggesting that the draining lymph node near the IL-2 injection site showed nests of lymphocytes which were not seen in the other lymph nodes. An interesting side effect of the IL-2 therapy was the decrease in circulating eosinophils. It is difficult to interpret this finding and correlate it with known effects of IL-2. Eosinophilia, however, has been reported in immunodeficient patients (23). In these cases, eosinophilia was correlated with Pneumocystis carinii infections which frequently occur in immunode ficient patients. Since post mortem inspection of our patient was not feasible, a safe diagnosis of such infections could not be obtained in this case. We think, however, that the observed decrease of eosinophils following
- 9. 460 . R. DOPFER et al. IL-l administration may be a further, though indirect, sign of transient improvement of the immunological.status. We realize that many questions, in particular that of the appropriate dose of IL-2, are still open, but we are hopeful that IL-2 therapy can assist conventional medication of life-threatening infections in immunodeficient patients and may, if not restore a normal T cell response, at least prolong the life of such patients until a HLA-matched bone marrow donor can be found. References 1. GILLIS, S., D. Y. MOCHIZUKI, P. j. CONLON, S. H. HEFENFIDER, C. A. RAMTHUN, A. E. GILLIS, M. B. FRANK, C. S. HENNEY, and J. D. WATSON. 1982. Molecular characteriza tion of Interleukin 2. Immunol. Rev. 63: 167. 2. FARRAR, j. j., W. R. BENJAMIN, M. L. HILFIKER, M. HOWARD, W. L. FARRAR, and J. FULLER-FARRAR. 1982. The biochemistry, biology, and role of Interleukin-2 in the induction of cytotoxic T cell and antibody-forming B cell responses. Immuno!. Rev. 63: 129. 3. LOPEZ-BoTET, M., G. FONTAN, M. C. G, RODRIGUEZ, and M. O. DE LANDAZURI. 1982. Relationship between IL-2 synthesis and the proliferative response to PHA in different primary immunodeficiencies. J. Immuno!. 128: 679. 4. FLOMENBERG, N., K. WELTY., R. MERTF.LSMANN, N. KERNAN, N. CiOBANU, S. VENUTA, S. FELDMAN, G. KRUGER, D. KIRKPATRICK, B. DUPONT, and R. O'RULLY. 1983. Immunologic cffccts of Interlcukin 2 in primary immunodeficiency diseases. J. Immuno!. 130: 2644. 5. LINKER-IsRAELI, M., A. C. BAKKE, R. C. KITRIDOU, S. GENDLER, S. GILLIS, and D. A. HORWI17.. 1983. Defective production of lnterleukin 1 and Interleukin 2 in patients with systemic lupus erythematosus (SLE). j. Immuno!. 130: 2651. 6. PETER, H. H., P. GRONEWOLD, H. KIRCHNER, and H. NORTHOl'F. 1983. Lymphokine production in common varied immunodeficiency, polyclonal hyper-gammaglobulinemia and granulomatous diseases. In: lnterleukins, Lymphokines and Cytokines. Eds. j. J. OPPENHEIM and S. COHEN. Academic Press, Inc. New York, USA, pp. 677-685. 7. CiOBANU, N., K. WELTE, G. KRUGER, S. VENlITA,J. GOLD, S. P. FELDMAN, C. Y. WANG, B. KOZINER, M. A. S. MOORE, B. SAFAI, and R. MERTELSMANN. 1983. Defective T-cell response to PHA and mitogenic monoclonal antibodies in male homosexuals with acquired immunodeficiency syndrome and its in vitro correction by Interleukin 2. J. Clinical Immunology (in press). 8. B6DEKER, B. G. D., j. LEHMANN, J. VAN DAMME, H. KApPMEYER, W.-D. GASSEL, K. HAVEMANN, U. SCHWUl.ERA, F. RUHL, and P. F. MOH}.RADT. 1984. Production of five human lymphokines (granulocyte-macrophage colony stimulated factor, Interferon-y, Interleukin-2, macrophage cytotoxicity factor and macrophage migration inhibitory factor) from Con A stimulated lymphocyte cultures in bioreactors. Immunobiol. 166: 12. 9. PAULY, J. L., C. W. RUSSELL, J. A. PLANINSEK, J. MINOWADA. 1982. Studies of cultured human T lymphocytes. I. Production of the T cell growth-promoting Iymphokine Interleukin-2. j. Immuno!. Methods 50: 173. 10. LE BLANC, P. A., and S. W. RUSSELL 1981. Depletion of mononuclear phagocytes: pitfalls in the use of carbonyl iron, carrageenan, silica, trypan blue, or antimononuclear phago cyte serum. In: Methods for Studying Mononuclear Phagocytes. Eds. D. O. ADAMS, P. J. EDELSON, and H. KaZEN. Academic Press, New York, USA, pp. 231-242. 11. B6DEKER, B. G. D., C. KORTMANN, H. H. PETER, W.J. PICHLER, and P. F. MUHLRADT. 1982. Intcrlcukin-2 in the ontogeny of human lymphoid tissue. Immunobiol. 162: 66.
- 10. [n vivo Effect'; of Interleukin 2 461 12. PETER, H. H., W. FRIEDRICH, R. DOPFER, W. MOLLER, C. KORTMANN, W.j. PICHLER,F. HEINZ, and C. H. L. RIEGER. 1983. NK cell function in severe combined immunodefi ciency (SCID): evidence of a common T and NK cell defect in some bm not all SCID patients. J. Immuno!. 131: 2332. 13. KUNG, P., and G. GOLDSTEIN. 1981. Functional and developmental compartment'; of human T lymphocytes. Vox. Sang. 39: 121. 14. jANOSSY, G., N. TIDMAN, E. S. PAPAGEORIOU, P. C. K UNG, and G. GOLDSTEIN. 1980. Distribution of T lymphocyte subsets in the human bone marrow and thymus: an analysis with monoclonal antibodies. J. Immuno!. 126: 1608. 15. ORTAlDO, J. R., S. 0. SHARROW, T. TIMONEN, and R. B. HEIlBERMANN. 1981. Detenni nation of surface antigens on highly purified human NK cells by flow cytometry with monoclonal antibodies, J. ImmunoL 127: 2401. 16, HIRSCHHORN, R" and D. W, MARTIN, 1979. Enzyme defects in immunodeficiency diseases. In: Immune Deficiency. Eds, M, D. COOPER et al., Springer-Verlag Berlin, Heidelberg, New York. pp. 65-87. 17. ABO, T., and C. M. BALCH, 1982. Characterization of HNK-l t (Leu-7) human lympho cytes. II. Distinguishing phenotypic and functional properries of natural killer cells from activated NK-like cells. J. Immuno!. 129: 1758. 18. MOHLRADT, p, E, and H, G. Opm. 1982. Clearance of Interleukin 2 from the blood of normal and T cell-depleted mice. Eur. J, Immuno!. 12: 983. 19. DONOHUE, J. H., and S. A. ROSENBERG. 1983. The fate of Interleukin-2 after in vivo administration. j. Immuno!. 130: 2203, 20, DE SOUSA, M., and A. M, CARROLL. 1982. Circulation of lymphocytes: Relevance to clinical immunology. Plasma Therapy and Transfusion Technol. 3: 375, 21. KURIBAYASHI, K., S. GILLIS, D. E. KERN, and C. S, HENNEY. 1981. Murine NK cell cultures! effect'; of Interleukin-2 and interferon on cell growth and cytotoxic reactivity. J. Immunol. 126: 2321. 22, GRAY, C. H., and V. H. T, JAMES. 1979, In: Honnones in Blood. Vol. I. Acad, Press. London, New York, San Francisco, USA. 23. JOSE, D. G., R, A. GAlTI, and R. A, GOOD. 1971. Eosinophilia with pneumocystis carinii pneumonia and immune deficiency syndromes. J. Pediatrics. 79: 748. Dr, p, F. MUHLRADT, GBF - Gesellschaft fur Biotechnologische Forschung mbH, Masche roder Weg 1, D-3300 Braunschweig, FRG