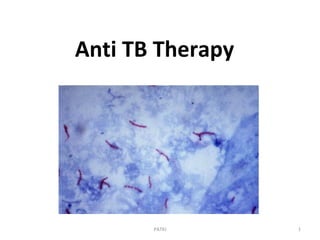
Anti tb drugs
•Als PPT, PDF herunterladen•
26 gefällt mir•9,340 views

This ppt discusses Pharmacology of Anti tubercular drugs and their use in clinical practice.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Anti tb drugs
Ähnlich wie Anti tb drugs (20)
Mehr von Dr Pralhad Patki
Mehr von Dr Pralhad Patki (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Anti tb drugs
- 2. At the end of the session, students will be able to • Enumerate primary and second line anti tubercular drugs. • Describe phases of treatment of tuberculosis. • Describe mechanism of action, and adverse effects of Primary and secondary Anti Tb drugs. • Define MDR tuberculosis and measures to prevent it. • Describe the roll of Vaccines and drugs to prevent tuberculosis. PATKI 2
- 3. 3 Tuberculosis : A Global Emergency • One third of the world’s population is infected • TB kills 5,000 people a day – 2 to 3 million/yr • More than 100,000 children will die this year • Hundreds of thousands of children will become TB orphans this year • HIV and TB co-infection are producing explosive epidemics • MDR is seriously threatening global TB control
- 4. 4 TB is the Leading Infectious Cause of Death among Persons >5 years old 0 1 2 3 4 TBARI DiarrheaAIDS Malaria Tropical Diseases Number of deaths (millions) Source: WHO World Report 2000
- 5. 5 Tuberculosis the Disease • Normal progression of disease – 50% die, 25% spontaneous cure, and 25% chronic excretors • Treatment requires multiple drugs for prolonged periods. Good results possible • Treatment interruptions or monotherapy lead to drug resistance • Drug resistance can be transmitted (primary) or developed (secondary)
- 6. • Coughing that lasts at least three weeks • Coughing up blood • Chest pain • Discomfort when breathing or coughing • Fever • Chills • Night sweats where you wake up soaking wet • Exhaustion, Loss of appetite, • Weight loss PATKI 6
- 7. 7 Treatment of TB • TB is treated with multiple drugs to avoid drug resistance and treatment failures • Intensive phase = 4 drugs: Rifampicin, Isoniazid, Pyrazinamide, and Ethambutol or Streptomycin • Continution phase = 2 drugs: INH & Rif or Eth • If drugs are counterfeit or substandard, may cause treatment failures and lead to the development of Multidrug-Resistant TB (MDRTB)
- 8. 8
- 9. M. tuberculosis: peculiar featuresM. tuberculosis: peculiar features • Rapid growers: In the wall of cavitary lesion, extracellular. • Slow growers: intracellular, within the macrophages at inflamed sites. • Spurters: intermittent growth spurts. • Dormant: Do not grow for long time, become active at times of low host resistance. • ATYPICAL- AVIUM, KANSASII • Lipoarabinomannan- helps survival in macrophages Bacilli continuously shift from one to other subpopulation.Bacilli continuously shift from one to other subpopulation.
- 10. Mycobacterial cell wallMycobacterial cell wall Baron S (ed.) Medical Microbiology. 4th edition. Chapter 33
- 11. PATKI 11
- 12. Diagnosis of TB • Clinical features are not confirmatory. • Zeil Nielson Stain • Adenosine deaminase test • Culture most sensitive and specific test. – Conventional Lowenstein Jensen media 3-6 wks. – Automated techniques within 9-16 days • PCR is available, but should only be performed by experienced laboratories • Mantoux test
- 13. PPD Tuberculin Testing • Sub cutaneous • Weal formation • Itching – no scratch. • Read after 72 hours. • Induration size. • 5-10-15mm
- 14. PPD result after – 72 hours.
- 15. Interpretation • (i) Induration less than 5 mm – no exposure to tubercular bacilli. • (ii) Induration between 5-9 mm – this can be due to atypical mycobacteria or BCG vaccination. It may suggest infection in immunocompromised children such as HIV infection or other immunosupression; • (iii) Induation 10 mm or more – an induration of 10 mm or more at 48-72 hours in a child with symptoms of tuberculosis should be interpreted as tubercular disease
- 16. PATKI 16
- 17. Chemotherapy in tuberculosisChemotherapy in tuberculosis • Goals of anti-tubercular chemotherapy • Kill dividing bacilli: Patient is non-contagious : transmission of TB is interrupted. • Kill persisting bacilli: To effect cure and prevent relapse. • Prevent emergence of resistance: so that the bacilli remain susceptible to the drugs.
- 18. Chemotherapy in tuberculosisChemotherapy in tuberculosis • Goals of anti-tubercular chemotherapy • Kill dividing bacilli: Patient is non-contagious : transmission of TB is interrupted. • Kill persisting bacilli: To effect cure and prevent relapse. • Prevent emergence of resistance: so that the bacilli remain susceptible to the drugs.
- 19. Antitubercular AgentsAntitubercular Agents • Now there is emergence of multidrug resistant ( MDR ) TB . More than 0.4 million cases globally . • In addition- HIV association.
- 20. Overview-Anti TB regimen. Essential anti-TB drugs-Primary drugs. Anti TB therapy. TB a rampant infectious disease . Anti TB drugs have revolutionized the management. Standard Category I regimens (new cases) Management of smear- negative suspect case- Category 2 patients 20PATKI
- 21. Lines and Regimens Defined • First-Line Therapy – Category I regimen for new patients – Category II regimen for re-treatment patients – Suspicion of resistance to one anti-TB drug Category III- New cases of smear –ve pulmonary TB with limitedNew cases of smear –ve pulmonary TB with limited parenchymal involvement or severe form of extraparenchymal involvement or severe form of extra pulmonary TB .pulmonary TB .e.g.-Lymph node TB Unilateral pleural effusion Bone (excluding spine ) Peripheral joint & skin TB • Second-Line Therapy – For patients with resistant TB to more than one drug 21PATKI
- 22. First Line Anti-Tuberculosis Drugs • Isoniazid (INH, H) • Rifampicin (RIF, R) • Pyrazinamide (PZA, Z) • Ethambutol (EMB, E) • Streptomycin (SM, S) Plus Pyridoxine 22PATKI
- 23. Antitubercular AgentsAntitubercular Agents First line drugs:First line drugs: Isonizid ( H) Rifampicin (R) Ethambutol (E) Pyrazinamide ( Z) Streptomycin ( S) now reserved drug in first line
- 24. Antitubercular AgentsAntitubercular Agents Second line drugs:Second line drugs: Thiacetazone Para aminosalicylic acid (PAS) Ethionamide ( Etm) Kanamycin Cycloserine Amikacin Capreomycin
- 25. Antitubercular AgentsAntitubercular Agents Newer Second Line drugs:Newer Second Line drugs: Ciprofloxacin Ofloxacin Levofloxacin Clarithromycin Azithromycin Rifabutin
- 26. Drugs used in TuberculosisDrugs used in Tuberculosis 1st line drugs high efficacy, low toxicity • Isoniazid (INH) • Rifampin • Pyrazinamide • Ethambutol • Streptomycin 2nd line drugs Low efficacy, high toxicity or both • Ethionamide • Para aminosalicylic acid • Cycloserine • Amikacin/ Capreomycin • Fluoroquinolones • Rifabutin
- 27. Antitubercular AgentsAntitubercular Agents Isoniazid (Isonicotinic acid hydrazide,H):Isoniazid (Isonicotinic acid hydrazide,H): Essential component of all anti TB regimen (except intolerance to H or resistance) -It is tuberculocidal , kills fast multiplying organism & inhibit slow acting organism -Acts both on intracellular ( present in macrophages ) & extracellular bacilli -It is the cheapest AT AgentIt is the cheapest AT Agent
- 28. Antitubercular AgentsAntitubercular Agents -Atypical mycobacteria are not inhibited by INH. Not active against any other micro-orgs. Mechanism of Action :Mechanism of Action : Inhibit synthesis of mycolic acid ( unique fatty acid component of mycobacterial cell wall .)
- 29. Antitubercular AgentsAntitubercular Agents -INH enters the bacilli by passive diffusion. It must be activated to become toxic to bacilli. It becomes toxic by Kat G (multifunctional Catalase - peroxidase , a bacterial enzyme ) which catalyzes the product from INH an Isonicotinoyl radical that subsequently inter-acts with mycobacterial NAD & NADP.
- 30. Antitubercular AgentsAntitubercular Agents a nicotinoyl NAD isomer which ↓ the activity of enoyl acyl carrier protein reductase (Inh A) & β- ketoacyl carrier protein synthase ( Kas A) , inhibition of these enzymes↓ the synthesis of mycolic acid an essential component of the mycobacterial cell wall & causes cell death.
- 31. MOA of 1MOA of 1stst line drugsline drugs Mycolic Acid Arabinogalactan Peptidoglycan Cell membrane DNA RNA polymerase mRNA R I B O S O M e Protein Isoniazid - Pyrazinamide - Mitochondria (ATP) - Rifampin - Ethambutol - Streptomycin - Cytoplasm
- 32. Antitubercular AgentsAntitubercular Agents - If INH is given alone , inherent resistant bacilli proliferate selectively & after 2-3 months an apparently resistant infection emerges .
- 33. Antitubercular AgentsAntitubercular Agents - Combination therapy with INH has good resistance preventing action . - There is no cross resistance .
- 34. Antitubercular AgentsAntitubercular Agents PharmacokineticsPharmacokinetics : -Completely absorbed orally , penetrate all body tissues, tubercular cavities , placenta & meninges . - Metabolized in liver by acetylation & metabolites are excreted in urine . - Rate of acetylation shows genetic variation ( fast acetylators > 30% Indians - t½ -1 hr Slow acetylators >60% Indians -t ½- 3 hrs)
- 35. Antitubercular AgentsAntitubercular Agents (daily regimen is not affected but biweekly regimens are less effective in fast acetylators ) DoseDose – 4-6 mg/ kg for >50 kg – 300 mg daily - 600 mg bi-wkly
- 36. ISONIAZID (INH): PharmacokineticsISONIAZID (INH): Pharmacokinetics Acetylation (Phase II) Hydrolysis (Phase I) Isonicotinic acid INH N-acetyl transferase N-acetyl Isoniazid Acetyl hydrazine Genetic polymorphism affects INH metabolismGenetic polymorphism affects INH metabolism Slow acetylators are at higher risk of developing neuritisSlow acetylators are at higher risk of developing neuritis
- 37. Antitubercular AgentsAntitubercular Agents ADRs -ADRs - Well tolerated drug 1.Peripheral neuritis & other neurological manifestations- parasthesia , numbness, mental disorientation & rarely convulsion ( due to interference with utilization of pyridoxine & ↑ excretion in urine )
- 38. Antitubercular AgentsAntitubercular Agents Due to this Pyridoxine given prophylactically -10 mg/day10 mg/day which prevents neurotoxicities (INH neurotoxicity treated with Pyridoxine-100 mg/ day100 mg/ day ) 2. Hepatitis – more common in older patients & alcohlics ( reversible) 3. Rashes , fever , acne & arthralgia .
- 39. Rifampicin • Bactericidal to M Tub. N Menig, H Influen, Klebsi, Lepre, • All population of M Tub. Extra and intracellular. Sterilizing effect. • DNA dependent RNA Polymerase. • Bioavailability 70 %- ABSENCE OF FOOD. • Enzyme inducer- Drug interactions. OC. INH • High sterilizing effect. All forms of bacteria PATKI 39
- 40. R • 450-600 MG Oral , Morning • Color of urine • Hepatitis • With INH • With PYRAZINAMIDE • ADR- Hepatitis, Cutaneous syndrome • Abdominal syndrome • Meningococcal meningitis –Prophylaxix PATKI 40
- 41. SM- 1 G- IM Activity against bacteria: Bactericidal Inhibit bacterial protein synthesis. Active – Aerobic Gr - ve bacilli , not anaerobic. Exibit post-antibiotic effect Adverse Effects: Narrow margin of safety All are ototoxic and nephrotoxic. PATKI 41
- 42. Mechanism of action • Protein synthesis inhibitors- 3 steps 1. Transport into bacteria. 2. Inhibition of initiation complex of peptide chain, misreading of RNA chain → termination of peptide chain → Abnormal proteins. 3. Incorporation of ab proteins in cytoplasmic membrane →↑ permeability → ↑ transport. 03/27/19 42PATKI
- 43. Antibacterial spectrum • Primarily active against - Gr –ve aerobic bacilli. - E.coli, klebsiella, shigella , Proteus , psuedomonas etc… - But none is active against salmonella. • Few gr +ve cocci - Staplylococcus aureus, Str. Viridans, Str. Feacalis(streptomycin,gentamicin). • Aminoglycosides not active against str.pnuemoniae. • Not effective against - Gr +ve bacilli, Gr –ve cocci, and Anaerobes 03/27/19 43PATKI
- 44. Adverse effects • I) Ototoxicity - cochlear damage • vestibular damage • Cochlear damage - Deafness is permanent with tinnitus • Auditory nerves degenerate in retrograde manner • Hearing loss affects high frequency sounds first, than low frequencies leading to progressive hearing loss. • Vestibular – Head ache, nausea & vomiting vertigo, Ataxia – Streptomycin ,Gentamicin. • Potentiated by pre-existing disease / other drugs ( Ethacrynic acid, Furosemide) .03/27/19 44PATKI
- 45. Pyrazinamide • More active at pH 5.5- Intracellular action. • Converted to pyrazinoic acid . Cidal. • Distributed to all tissues including meninges • Sterilizing effect, -Inhibits mycolic acid • 70 mg/ kg • Hepatitis • Uricacid. Hyperurecemia PATKI 45
- 46. Ethambutol • Static , inhibits arabinosyltransferase • Cell wall , mycolic acid • 75% excreted unchanged. • RBC concentration –double. • 25 mg /kg • Inflamed meninges • Optic neuritis, loss of acuity of vision, color, PATKI 46
- 47. Activities of Antituberculosis Drugs Drug Early bactericidal activity Preventing drug resistance Sterilizing activity Isoniazid ++++ +++ ++ Rifampicin ++ +++ ++++ Pyrazinamide + + +++ Streptomycin ++ ++ ++ Ethambutol ++ - +++ ++ + Highest ++++ High +++ Intermediate ++ Low + 47PATKI
- 48. Continuation Phase of Treatment • The preferred continuation phase consists of isoniazid and rifampicin given for four months. • Isoniazid and ethambutol given for six months is an acceptable continuation phase regimen that may be used when adherence cannot be assured, but is associated with a higher rate of failure and relapse, especially in patients with HIV infection. 48PATKI
- 49. Treatment Recommendations 1. Streptomycin may be substituted for EMB. 2. Ethambutol may be omitted for adults and children who have negative sputum smears, do not have extensive pulmonary tuberculosis or severe forms of extra- pulmonary disease and who are HIV negative 3. Associated with higher rate of treatment failure and relapse; should generally not be used in patients with HIV infection. Ranking Initial Phase (2 mos.) Continuation Phase Preferred INH, RIF, PZA, EMB1,2 daily INH, RIF daily, 4 mos. INH, RIF, PZA, EMB1,2 3x/wk. INH, RIF 3x/wk, 4 mos. Optional3 INH, RIF, PZA, EMB daily INH, EMB daily, 6 mos. 49PATKI
- 50. Dose Recommendations Drug Daily 3x Week INH 5 (4-6), max 300/d 10 RIF 10 (8-12), max 600/d 10 (8-12) max 600/ d PZA 25 (20-30) 35 (30-40) EMB children: 20 (15-25)* adults: 15 (15-20)* 30 (25-35) Streptomycin 15 (12-18) 15 (12-18) *The recommended daily dose of ethambutol is higher in children (20 mg/kg) than in adults (15mg/kg), because the pharmacokinetics are different (peak serum ethambutol concentrations are lower in children than in adults receiving the same mg/kg dose) mg/kg (range) 50PATKI
- 51. Success story • 37 million lives have been saved between 2000-2013. • TB incidence fell world wide -1.5% per year. • But- 2013- 9 million cases- 1.5 million died, -60% men. PATKI 51
- 52. Second line • PAS- SAME like Sulpha • Cycloserine- cellwall synthesis-Neurotoxicity, psychiatric illness, Oral • Caproemycin, 1 gm im. Nephrotoxicity, ototoxic • Amikacin • Thiacetazone • Rifabutin- Atypical, Rifapentine PATKI 52
- 53. Fluoroquinolones • Ciprofloxacin • Ofloxacin • Levofloxacin • Spar • Gati • Moxi PATKI 53
- 54. TB Treatment and Liver • Hepatitis-Main ADR of Anti TB regimen. • Use standard short-course regimen for patients without clinical evidence of chronic liver disease but history of: – Hepatitis virus carriage – Acute hepatitis – Excessive alcohol consumption • Use a liver-sparing regimen for patients with established chronic liver disease – 2SHRE/6HR or 2SHE/10 HE 54PATKI
- 55. Hepatitis • Hepatitis (asymptomatic elevation AST/ALT occurs in 20% patients on 4 drugs) – Drug induced hepatitis = ↑ AST or ALT ≥3 times upper limits of normal in the presence of symptoms OR ↑ >5 times if asymptomatic – INH, PZA and RIF can all cause hepatotoxicity – Hepatitis from INH is age related, from PZA is dose related, and RIF is unpredictable and less common 55PATKI
- 56. TB Treatment and Hepatitis • If ↑ ≥3x normal with symptoms or >5x normal without symptoms: – stop all anti-TB medications and evaluate patient – refer patient to doctor for clinical evaluation – try to rule out other causes of acute liver disease – if severely ill, may start 3 non-hepatotoxic drugs – after AST <2 times upper limit of normal — rechallenge drugs one-by-one starting with drugs that are not hepatotoxic 56PATKI
- 57. ANTI-TB DRUGS Possible mechanism of the liver injury Drug Acetyl agent Acetyl hydrazine - intermediate Acylating agent Liver cell necrosis 57PATKI
- 58. streptomycin • Use restricted to certain infections in combination with other drugs. • Given by deep IM inj- 0.5 – 1 gm /day. • Uses – 1. Bacterial endocarditis 2. Tularemia , Brucellosis 3. Plague 4. Tuberculosis 03/27/19 58PATKI
- 60. Antitubercular TherapyAntitubercular Therapy Short course chemotherapy-Short course chemotherapy- Regimen of 6-9 months treatment In 1997 WHO framed clear cut guidelines for different category of TB treatment . All regimen have initial intensive phase -2 3 months to rapidly kill the TB bacilli & bring sputum conversion & afford symptomatic relief followed by continuation phase last 4-6 months for elementary remaining bacilli
- 61. Antitubercular TherapyAntitubercular Therapy Categories:Categories: Category I –New ( untreated ) smear +ve pulmonary TBNew ( untreated ) smear +ve pulmonary TB -New smear –ve pulmonaryTB with extensiveNew smear –ve pulmonaryTB with extensive parenchymal involvementparenchymal involvement -New cases of severe forms of extra- pulmonary-New cases of severe forms of extra- pulmonary TB e.g.-TB e.g.- meningitis , miliary TB , pericarditismeningitis , miliary TB , pericarditis -B/L or extensive pl. effusion , intestinal orB/L or extensive pl. effusion , intestinal or genitourinary TBgenitourinary TB
- 62. Antitubercular TherapyAntitubercular Therapy ((Revised National Tub. Control programmeRevised National Tub. Control programme In India in 1997— DOTs –follow thrice wklyIn India in 1997— DOTs –follow thrice wkly regimen to ↓ cost & it is more practicalregimen to ↓ cost & it is more practical ) WHOWHO : - 2HRZE(S) (initial phase)-daily - 4HR or 6HE (continuation phase,)daily total duration 6-8 months6-8 months RNTCP :RNTCP : 2H3R3Z3E3 + 4H3R3 -2H3R3Z3E3 + 4H3R3 -total duration- 6month6month
- 63. Antitubercular TherapyAntitubercular Therapy Category II -Smear +ve failure ,relapse & interrupted Tt casesSmear +ve failure ,relapse & interrupted Tt cases -Relapse- cured TB Patient again become sputum +ve-Relapse- cured TB Patient again become sputum +ve -Tt after interruption –interrupted Tt x 2month →return to-Tt after interruption –interrupted Tt x 2month →return to sputum + ve casesputum + ve case WHO:WHO: Initial phase –dailyInitial phase –daily 2 HRZES +1 HRZE2 HRZES +1 HRZE Continuation phaseContinuation phase –5HRE -5HRE - total 8 monthotal 8 month RNTCP:RNTCP: Initial phase -2H3R3Z3E3S3 +1H3R3Z3E32H3R3Z3E3S3 +1H3R3Z3E3 Continuation phase -5H3R3E35H3R3E3 –total 8 months
- 64. Antitubercular TherapyAntitubercular Therapy Category III New cases of smear –ve pulmonary TB with limitedNew cases of smear –ve pulmonary TB with limited parenchymal involvement or severe form of extraparenchymal involvement or severe form of extra pulmonary TB .pulmonary TB . e.g.-Lymph node TB Unilateral pleural effusion Bone (excluding spine ) Peripheral joint & skin TB
- 65. Antitubercular TherapyAntitubercular Therapy WHO :WHO : Initial phaseInitial phase -2HRZ (daily) Continuation phaseContinuation phase - 4HR or 6HE (daily) Total duration-6-8 monthsTotal duration-6-8 months RNTCP : Initial phase -Initial phase -2H3R3Z3 ( daily ) Continuation phase -Continuation phase -4H3R3 ( daily ) Total duration- 6 monthsTotal duration- 6 months
- 66. CATEGORY-WISE TREATMENTCATEGORY-WISE TREATMENT (WHO1997 & RNTCP1997(WHO1997 & RNTCP1997) TBTB CategoryCategory Initial PhaseInitial Phase (daily /3xper week)(daily /3xper week) ContinuationContinuation PhasePhase (daily/3xper week)(daily/3xper week) TotalTotal DurationDuration i. 2 HRZE(S)/ 2H3R3Z3E3 4 HR/ 4H3R3 or 6HE 6 8 ii. 2 HRZES+ 1HRZE / 2H3R3Z3E3S3+1H3R3Z3 E3 5 HRE or 5H3R3E3 8 8 iii. 2 HRZ/ 2H3R3Z3 4 HR/4 H3R3 or 6 HE 6 8
- 68. PATKI 68
- 69. PATKI 69 Steroid side effects CUSHINGOID : Cataracts Ulcers Skin: striae, thinning, bruising Hypertension/ Hirsutism/ Hyperglycemia Infections Necrosis, avascular necrosis of the femoral head Glycosuria Osteoporosis, obesity Immunosuppression Diabetes
- 70. PATKI 70
- 72. PATKI 72
- 73. PATKI 73
Hinweis der Redaktion
- Multi drug Resistance = MDR
- Overview: [Review content of slide] Lecture/module includes International Standards for Tuberculosis Care 7, 8, and 10 Standards 7 & 8 refer to both pulmonary and extrapulmonary TB, although most of the public health issues relate to pulmonary TB. Differences in the treatment of extrapulmonary TB are presented later in this session [Image credit: World Lung Foundation Image Library, Pierre Virot]
- First-line therapy includes two treatment regimens: category I (and III) for new patients, and category II for re-treatment patients who may have TB resistant to one medication Second-line therapy is treatment for patients with TB resistant to more than one drug and will be covered in Module 10 on Chronic and MDR-TB
- They are called first-line because of their effectiveness, fewer side-effects and they are less costly than the drugs listed as second-line Five drugs are considered first-line: The first four are used in category I regimens; streptomycin is added to the category II regimen Standard abbreviations for each of these medications are shown The Caribbean TB Guidelines for the Prevention, Treatment, Care and Control of Tuberculosis advises the use of treatment regimens recommended by WHO and all Stop TB partners
- This table shows the relative activities of the first line antituberculosis drugs Isoniazid has the most potent early bactericidal effect and is also effective in preventing resistance, but has less sterilizing effect Rifampicin has a weaker early effect but is more potent than isoniazid in its sterilizing activity Pyrazinamide is only effective as a sterilizing agent. [Note: relatively poor agent for prevention of drug resistance] Streptomycin has an intermediate effect in all three activities as does ethambutol Source: Mitchison DA. The action of anti-tuberculosis drugs in short-course chemotherapy. Tubercle. 1985;66:219-25
- Standard 8 continued: [Read Standard] This portion of standard 8 addresses the continuation phase regimens The major points from the slide are that it is preferable to use rifampicin throughout the continuation phase, although isoniazid and ethambutol may be used in some circumstances The reason for this alternative continuation phase regimen is to reduce the likelihood of resistance to rifampicin developing when treatment cannot be supervised effectively A review of the outcomes of treatment of TB in patients with HIV infection clearly shows that TB relapse is minimized by the use of a regimen containing rifampicin throughout a six-month course. Thus, the 6 month regimen containing rifampicin throughout the entire course is preferable in patients with HIV infection to minimize the risk of relapse; however, the patient’s HIV stage, the need for, and availability of, antiretroviral drugs, and the quality of treatment supervision/support must be considered in choosing an appropriate continuation phase of therapy Second, the shortest total duration of treatment is 6 months. Although regimens of less than 6 months have been evaluated in clinical trials, a Cochrane systematic review on this topic, and a more recent review found that regimens &lt;6 months have an unacceptably high rate of relapse. The current international standard, therefore, is a regimen administered for a minimum duration of 6 months [Gelband H., et al. Regimens of less than six months for treating tuberculosis. Cochrane Database Syst Rev 2000(2):CD001362; and Santha T, et al. What is the optimum duration of treatment? In: Friedan TR,ed. Toman’s tuberculosis. Case detection, treatment and monitoring, 2nd Edition. Geneva: WHO,2004]
- Treatment recommendations for persons not previously treated. This slide presents in tabular form the information contained in Standard 8 and also indicates that streptomycin can be substituted for EMB [Interactive option: Ask participants about what their standard practice is locally for the initiation and continuation phases of treatment.] [World Health Organization. Treatment of Tuberculosis: Guidelines for National Programmes, Third Edition. Geneva: World Health Organization, 2003.]
- The evidence base for currently recommended anti-TB drug dosages derives from human clinical trials, animal models, pharmacokinetic and toxicity studies. The evidence on drug dosages and safety and the biological basis for dosage recommendations have been extensively reviewed in publications by the WHO, The Union, the ATS, the CDC, and IDSA Intermittent administration of anti-TB drugs enables supervision to be provided more efficiently and economically with no reduction in efficacy. The evidence on effectiveness of intermittent regimens was reviewed recently. These reviews, based on several trials, suggest that anti-TB treatment may be given intermittently 3 times a week throughout or twice weekly in the continuation phase without apparent loss of effectiveness However, the WHO and The Union do not recommend the use of twice-weekly intermittent regimens because of the potentially greater consequences of missing 1 of the 2 doses Treatment of TB in special clinical situations such the presence of liver disease, renal disease, pregnancy, and HIV infection may require modification of the standard regimen or alterations in dosage or frequency of drug administration [For further guidance in these situations: World Health Organization. Treatment of Tuberculosis: Guidelines for National Programmes, Third Edition. Geneva: World Health Organization, 2003; ATS/CDC/IDSA Statement: Treatment of Tuberculosis. American Thoracic Society/Centers for Disease Control/Infectious Diseases Society of America, Am J Respir Crit Care Med 2003; 167(4):603-62.]
- Review the slide content Liver-sparing regimens: these are the regimens recommended in the 2003 WHO TB Treatment Guidelines and the Interim Caribbean TB Guidelines 2SHRE/6HR = Initial phase includes 2 months strep, INH, RIF and ethambutol; continuation phase with 6 months INH and RIF Alternate/optional regimen 2SHE/10HE = 2 months strep, INH and ethambutol in the initial phase followed by 10 months INH and ethambutol in the continuation phase. Note: other liver-sparing regimens using only one hepatotoxic drug or no potentially hepatotoxic drugs can be found in the American Thoracic Society, CDC, and Infectious Diseases Society of America document titled Treatment of Tuberculosis published in 2003. These can be downloaded from the CDC, Division of TB Elimination website under guidelines.
- Patients on TB treatment should be monitored for clinical, not laboratory, signs of toxicity (covered in greater detail in Module 7B on Monitoring) Usually lab tests are only done if there are symptoms or signs to suggest a problem, therefore, most laboratory confirmed hepatitis will be in symptomatic patients In the absence of any symptoms, however, ALT or AST up to 5 times normal can be tolerated without stopping or changing therapy
- In hepatotoxicity, stop all TB drugs until the patient improves Admit ill patients to the hospital Try to rule out other causes of acute liver disease before attributing it to the TB treatment Alcohol? Acute viral hepatitis? In cases of severe TB when it would be dangerous to halt all treatment, the doctor may consider using a “liver sparing regimen” (e.g., Ethambutol, strep, and a fluoroquinolone) The drugs that are not hepatotoxic, like strep and ethambutol, can be started together at full doses. Then add rifampicin in gradually increasing doses over several (5-7) days. If tolerated, then add isoniazid in gradually increasing doses (over 5-7 days). If these are tolerated, then PZA is the likely cause of the original hepatotoxicty and should be avoided. If hepatitis recurs with one of the drugs on challenge, then it must be discontinued and a regimen devised for the patient excluding the hepatitis-causing drug The process of reintroducing drugs and creating a new regimen is best done by an experienced doctor