
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie TESTS FOR AUDITORY ASSESSMENT
Ähnlich wie TESTS FOR AUDITORY ASSESSMENT (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
TESTS FOR AUDITORY ASSESSMENT
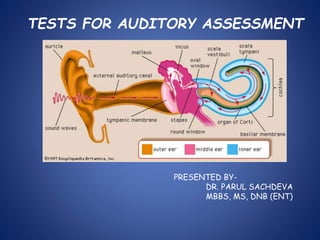
- 1. TESTS FOR AUDITORY ASSESSMENT PRESENTED BY- DR. PARUL SACHDEVA MBBS, MS, DNB (ENT)
- 2. What is sound??? A form of vibration that evokes a sensation of hearing. Travels in the wave form as areas ofcompressions and rarefactions.
- 3. Characteristics of the wave form
- 4. WHAT IS DECIBEL??? Decibel (dB) = 1/10 Bel. Bel is a base10 logarithmic ratio of intensity of given sound to threshold of hearing in normal subjects at 1000Hz. Named after Alexander Graham Bel – the inventor of telephone.
- 5. AUDITORY SYSTEM periperal central Comprising outer, the auditory pathway from Middle, inner ear & the cochlear nuclei till the auditory nerve. Auditory area in cerebral cortex.
- 8. Various tests are divided as – I. Clinical Tests II.Audiometric Tests III.Other Tests CLINICAL TESTS a. Finger friction test b. Watch test c. Speech test d. Tuning fork test
- 9. TUNING FORK TESTS Basic tests for hearing assessment during clinical Examination. Distinguishes conductive from sensorineural Hearing loss. Frequencies used are 256, 512 & 1024 Hz. Should be held 2cm infront of the EAM. A correctly activated one generates about 70dB Amplitude.
- 10. How to hold a tuning fork????
- 11. Method to activate a Tuning fork.
- 12. RINNE’S TEST Generally, AC > BC. Two methods are used- *threshold comparison *relative loudness method (prefered) Rinne’s +ve = AC > BC Rinne’s –ve = BC > AC (AB gap of 15-20 dB) -ve +ve AB Gap 256 Hz 512 Hz 20-30 dB 256, 512 Hz 1024 Hz 30-45 dB 256, 512, 1024 Hz 45-60 dB
- 13. WEBER’S TEST Performed by placing vibrating tuning fork over Forehead, bridge of nose/ incisor teeth. Lateralisation indicates a hearing loss of 15-25 dB With 512 Hz tuning fork. ABSOLUTE BONE CONDUCTION TEST Hearing tested in comparison to the examiner. The Ext. auditory meatus is occluded and bone Conduction is compared.
- 14. SCHWABACHS TEST Here as well, BC is compared with that of examiner’s but meatus isn’t occluded. BING TEST Tests bone conduction & examines the effect of Occlusion of ear canal on hearing. GELLE’S TEST Tests BC, effect of increased air pressure in ear Canal on hearing. (stapes fixation in Otosclerosis).
- 15. INTERPRETATION TEST normal Conducti ve deaf ness SN deafnes s RINNES +ve (AC > BC) -ve (BC > AC) +ve WEBER Not lateralised Lateralised –worse ear Lateralised- better ear ABC Same as examiner Same Reduced SCHWA BACH’S Same as examiner Lengthened Shortened BING +ve-louder on occlusion -ve – no change +ve GELLE’S +ve reduced hearing -ve no change +ve
- 16. PURE TONE AUDIOMETRY PURE TONE- sound sensation produced by fixed single frequency. Subjective test. Most commonly done. High frequencies stimulate d basal turns and lower frequencies the apical region.
- 17. Audiometer is an electronic device which produces pure tones, the intensity of which can be increased or decreased in 5dB steps. This is charted on a graph called AUDIOGRAM.
- 18. AIM IS????? Is there a hearing loss? If yes, conductive/SN? If SN, cochlear/retrocochlear? Degree of hearing dysfunction? HEARING THRESHOLD- minimum sound that a subject may hear for a given tone or frequency. Relative threshold is calculated. Air conduction-125 to 8000 Hz Bone conduction-250 to 4000 Hz.
- 19. SYMBOLS FOR PTA Air conduction Bone conduction
- 20. Mandatory Conditions to perform PTA 1.Calibration of the instrument. -electronic C. be done every 6 months. -biological C. be done before the test is administered to a subject. 2.Noiseless environment. The level of ambient noise can be checked by sound level Meter. 3.Position of headphones. Diaphragm should be over the opening of EAM. Improper placement causes variation of approx 15dB. 4.Proper instructions to the patient.
- 21. In BC , Sound reaches Cochlea in the following manner- *COMPRESSIONAL/DISTORTIONAL sound reaching cochlea causes alt. compression n expansion of the cochlear shell n causing movement ofcochlear fluid. *INERTIAL skull is set into vibration followed by ossicles with a lag. This sets up a relative motion b/w footplate of stapes n cochlear fluid deep to oval window. Vibration of cochlear fluid- sound is heard. *OSSEOTYMPANIC vibrating skull sets column of air in EAM into vibration. These vibrations are transmitted into inner ear just like air conduction.
- 22. Tecniques of air conduction -conventional Hughson-Westlake tecnique modified by Carhart and Jerger. -ASHA MASKING presenting a noise into the non test ear so that the non test ear is acoustically blocked n doesn’t participate in the hearing test. Imp coz if the non test ear (better hearing ear) gets stimulated, it will lead to false threshold for test ear.
- 23. Thus a shadow curve is obtained, meaning a curve which actually shadows the thresholds of better ear. Masking is a necessity during BC, as both cochlea get stimulated to the same level when a sound is presented. In AC, sounds of > 50dB stimulate the non test ear cochlea. WHEN TO MASK ????? INTERAURAL ATTENUATION- loss of a portion of sound energy when it passes from the test ear to cochlea of non test ear. RANGE IS B/W 45- 80 dB HL. IA = CROSS HEARING.
- 24. Whereas in BC, IA = 0 dB. Cross hearing is suspected when; AC (test) – BC (non test) > IA HENCE, During BC, ALWAYS MASK. During AC, MASK IF TESTING AT > 45 dB.
- 25. HOW MUCH TO MASK???? Max Masking = Bt + 45 dB
- 26. HOOD’S Plateau Method of Masking (used clinically) Unmasked AC thresholds found for both ears Non test ear masked ( AC + 15 dB) Test ear presented with sound Not heard, raise by 5dB heard, this is actual threshold Heard tone not heard Raise masking by 5dB raise tone by 5dB till pt starts to hear hears tone Raise masking by 5 dB, if still heard it is the actual threshold.
- 27. For BC, min. masking Bt + ( Am – Bm ) For AC, min. masking At – 45 + (Am – Bm) What sounds to use for masking?? *white noise- equal amount of sound of all frequencies. *narrow band noise (most effective)- has sound 100- 200 Hz above n below the test frequency. *complex noise- made of low frequency plus multiples of test frequency upto 4000 Hz.
- 28. MASKING DILEMMA *when min masking is more than the max masking. *seen in pts with large AB gap. *solution is using insert ear phones to present the masking sound.
- 29. INTERPRETATION Range of Hearing Loss 10 – 25 dB HL = Normal range 26 – 40 dB HL = Mild hearing loss 41 – 55 dB HL = Moderate 56 – 70 dB HL = Moderately Severe 71 – 90 dB HL= Severe Greater than 90 dB HL = Profound Pure tone average is calculated for 500, 1000 and 2000 Hz.
- 30. What we interpret??? AC threshold. BC threshold. AB gap. Requisite masking done? If it matches the clinical findings and tuning fork tests.
- 31. Conductive deafness AC > 30 dB BC < 20 dB AB gap > 25 dB
- 32. Sensorineural deafness AC > 30 dB BC > 20 dB AB gap < 20 dB
- 33. Mixed deafness AC > 45 dB BC > 20 dB AB gap > 20 dB
- 34. SHAPES OF AUDIOGRAMS FOR INTERPRETATION *for CONDUCTIVE lesion -left sloping- inc stiffness; eg otosclerosis -right sloping- secretory; eg secretory OM -large AB gap- ossicular discontinuity -notch at BC HL at 2000 Hz- otosclerosis *for SNL lesion -flat audiogram- atrophy of stria vascularis -descending- lesions in organ of corti. -notch at 4000 Hz- acoustic trauma -ascending curve (slope to left) – early endolymphatic hydrops -trough shaped- congenital SNL lesion.
- 35. Fallacies/Limitations •Inaccurate audiograms-improper technique • improper test condition • improper instrument • improper examiner •Subjective and time consuming test. •Doesn’t identify the nature of pathology.
- 36. USES -Measures threshold of hearing by air&bone conduction; thus degre&type of hearing loss. -Record for future reference. -Essential for prescription of hearing aid. -Find degree of handicap for medicolegal purpose. -Predict speech receprion threshold.
- 37. SPEECH AUDIOMETRY Subjective test which measures hearing sensitivity. Measures two variables- Speech Reception Threshold(SRT). Speech Discrimination Score(SDS). SRT- lowest level in dB HL at which 50% of spondee Words are correctly identified. Interepretation in normal hearing, SRT usually 2dB lesser than avg Of pure tone hearing thresholds at 500&1000 Hz.
- 38. In neural pathology, several dB higher than the pure tone average. SDS-%age of correctly identified words,when words from a specially prepared list called PB word list is presented to te subject. Interpretation Normal= 90-100% Neural lesions= considerably low Roll over ratio=(PBmax-PBmin)/ PB max Cochlear lesions = < 0.40 Neural lesions = > 0.45
- 39. SD Score Ability to understand speech 90-100% Normal 76-88% Slight difficulty 60-74% Moderate difficulty 40-58% Poor < 40% Very poor DRAWBACK in high frequency deafness, SDS becomes poor irrespective of whether it is cochlear or neural.
- 40. BEKESY AUDIOMETRY -Self recording audiometry, not performed now. -Two tracings- continuous and pulsed tone are obtained. Interpretation Type 1-cont n pulsed tones superimposed. normal and conductive deafness. Type 2-cont n pulsed tones superimposed upto 1000 Hz, falls behind pulsed tones after that. cochlear lesions.
- 41. Type 3-continuous falls behind pulsed tones from the very beginning. neural lesions. Type 4- pattern between type 2 and 3. neural lesions. Type 5- tracing for continuous tone above that of pulsed tone. malingerers.
- 42. IMPEDANCE AUDIOMETRY Objective test, widely used. Comprises 3 separate but related tests- *tympanometry *eustachian tube function test *acoustic/stapedial reflex test USES- -objective differentiation b/w conductive & SNHL. -DD in cases of conductive deafness. -measurement of middle ear pressure & evaluation of ET function. -DD of SNHL -Identification of lesion in facial paralysis,brain
- 43. Tympanometry Definition- Measurement of change of impedance of middle ear at the plane of the TM as a result of changes in air pressure in ext. auditory meatus. Principle- When sound strikes the TM, some of it is absorbed and rest reflected. Middle ear acts as an impedance matching device. Equipment has a probe with 3 channels- *deliver tone of 220Hz. *pick up reflected sound via microphone. *bring changes in air pressure in ear canal.
- 45. Tympanogram plotted with compliance as the ordinate(Y axis) n air pressure as abscissa(X axis).
- 46. Interpretation 1.Static compliance= max compliance-compliance at +200mm of H2O. Normal range is 0.35-1.40 ml. Compliance Increased in-ossicular chain discontinuity scarring of TM very large TM post stapedectomy Normal in-ET obstruction
- 47. Decreased in-otosclerosis adhesive/secretory otitis media ME tumors like glomus jugulare ossicular fixation tympanosclerosis 2.Measurement of middle ear pressure. Normal range is -50 to +50 mm of H2O. Negative in-Blocked ET Secretory OM
- 48. Normal in-stapedial otosclerosis ossicular chain discontinuity scarring of TM fixation/adhesions among ossicles Positive in-early acute OM Absent in-adhesive OM perforation of TM artifact patent grommet in TM ext ear canal blocked by cerumen.
- 49. 3. Shape of tympanogram Jerger classified them as follows- Type A- N ears, otosclerosis Type As-N pressure, dec compliance otosclerosis, thickened TM
- 50. Type Ad- N pressure, inc compliance ossicular chain discontinuty/scarrinf of TM Type B-little/no compliance n no sharp peak. OM with effusion/adhesive OM/perforation in TM.
- 51. Type C-negative middle ear pressure with N compliance. ET obstruction.
- 52. Feldman used 3 parameters for interpretation- *peak pressure *compliance/amplitude *type/configuration FALLACY When two types of ME pathology are present togethe static compliance is representative of the more lateral pathology.
- 53. Eustachian Tube Function Test Physiological functions assessed i.e. ventilatory function mucociliary clearance function *WILLIAM’S TEST measures 3 pressures P1-ambient pressure P2-pressure after swallowing P3-pressure after valsalva manouvere P1 is normal air pressure, during swallowing pressure dec n during valsalva inc. Any variation is considered abnormal.
- 54. *TOYNBEE’S TEST -Impedance audiometer is programmed to artificially inc or dec the air pressure in middle ear n record change of air pressure in middle ear, each time the pt swallows. -in perforated drum, as change of pressure during swallowing n recorded as step ladder type graph. -it should be completely neutralized by 3 to 4 swallows or considered abnormal.
- 55. ETT is carried out for min 40s to max 160s. Acoustic/Stapedial Reflex Test In normal hearing it is elicited at 70-105 dB HL.
- 56. ON AFFERENT SIDE sound enters ear- passes through middle ear- reaches cochlea- passes through 8th CN- reaches cochlear nucleus on same side- passes to superior olivary complex in the brain stem. CROSSING OF PATHWAYS OCCUR AND EFFERENT PATHWAY IS BILATERAL. ON EFFERENT SIDE Superior olivary complex- impulse to 7th CN nucleus of both side- passes through facial N.- passes through N. to stapedius- stapedius muscle contracts on both sides and pulls the stapes outwards and upwards. CHANGE IN IMPEDANCE OCCURS IN BOTH I/L N C/L EAR.
- 57. IMP- # of both stapedial crura is probably the only middle ear pathology which does not abolish the reflex. Interpretation -sensitive for middle ear pathology- absent in an ear with slighest of middle ear or tympanic membrane pathology. -cochlear lesions ,are present at comparitively lesser sound intensity levels due to loudness recruitment . -absence/presence in SNL depends on severity as well as the type.
- 58. SPAR It is based on the diff b/w acoustic reflex threshol ds to pure tone vs broadband noise(BBN) &on change in BBN thresholds bt not pure tone thresholds as a result of SNL loss. If a patient’s SPAR value is < 15, high probability of SNL hearing loss. Imp- A correction factor is applied to yield a SPAR value of 20 in normal hearing subjects.
- 59. METZ RECRUITMENT TEST -normal Acoustic Reflex hearing threshold is 70-105 dB above Pure Tone hearing threshold. -In cochlear lesions, gap is reduced due to loudness recruitment. -When range < 60 dB , cochlear lesion be suspected. ACOUSTIC REFLEX DECAY TEST -Change in intensity of acoustic reflex during first 10s of contraction of stapedial muscle, when sustained sound stimulus is presented. -If amplitude falls to less than 50 %- ABNORMAL DECAY- NEURAL/ RETROCOCHLEAR PATHOLOGY.
- 60. III- Other Tests. these include Auditory Evoked Potential Tests i.e. ECoG BERA MLR LLR OAE Tone Decay Tests SISI ABLB
- 61. BERA (Brainstem Evoked Response Audiometry)
- 62. *A non invasive procedure. *More standardized parameters. *No effect of sleep/anaesthesia. -Random electrical activity EEG continuously occurs in brain but sound evoked electrical activity is time specific & occurs at a fixed point of time after sound stimulation. -PTA readings are required to find out the hearing threshold.
- 63. Auditory Pathway Medial geniculate body Inferior colliculus Lateral lemniscus Superior & accessory olive area Dorsal cochlear nucleus Ventral cochlear nucleus Auditory cortex VIIIth nerve I II IV III VI V
- 64. Principle- Sound reaches the cochlea, converts into electric impulse and passes to auditory cortex. BERA evaluates the integrity of this pathway upto the level of lateral leminiscus. Evoked response can be recoreded upto 500ms. Upto 5ms – ECoG Upto 10ms- BERA 10-250ms – MLR 50-250ms- LLR (CERA)
- 65. Types of stimulus- *CLICKS- mixture of all frequencies but more amplification of middle and higher freq sounds with greatest energy at 3 KHz. *TONE PIPS- pure tone sounds of a specific frequency. PREREQUISITES- AC room with good earthing, pt lying down, eyes closed and preferably asleep. A total of 2000- 4000 recordings are done and then averaged and superimposed.
- 66. Method Elicited by click stimulus, 50-60 dB above average pure tone hearing level for 0.1ms. Masking is done with white noise. 3 electrodes are used-
- 67. Active electrode(red)- over the vertex. Reference electrode(white/black)- on mastoid/ear lobe of I/L ear. Ground electrode(green)- over forehead just above nasion /over C/L mastoid. Interpretation Recorded on a graph with amplitude in uV(ordinate) and time (ms) as abscissa.
- 68. WAVE Site Of Neural Generator. I COCHLEAR N. (DISTAL END) II COCHLEAR N. (PROXIMAL END) III COCHLEAR NUCLEUS IV SUPERIOR OLIVARY COMPLEX V LATERAL LEMINISCUS & INFERIOR COLLICULUS VI & VII NOT DEFINITELY KNOWN.
- 69. Wave V- largest & most robust. most reliable & easily identifiable. hallmark-sharp negative deflection immediately following the peak. Last wave to disappear & persists till intensity of stimulus is just about 10dB above avg pure tone hearing threshold. Wave IV- peak just preceding wave V. separately identifiable, present in 50-60% of subjects. If it gets superimposed with wave V, C/L ear is used as reference.
- 70. Wave III- preceding wave IV. upward peak b/w II & IV just beyond 3ms mark on graph. Amplitude= 0.2-0.25uV Present around 3.8ms mark Wave II- immediately preceding wave III. Wave I- sharp peak beyond 1ms mark. Imp to recognize as it gives us an idea –whether stimulus has crossed over from cochlea & distal end of auditory N. Amplitude is approx.= 1.8uV. Latency value = 1.65- 1.75 ms.
- 71. INTERPRETATION The parameters studied- -latency of the wave- absolute, interwave, interaural -amplitude- absolute & relative. -wave form morphology. -latency intensity functions of wave V. Absolute latency of wave V is most important.
- 72. LATENCY Latency of wave V is dependant on the intensity of sound stimulus. intensity of latency of wave V. Sound stimulus Interwave latency b/w wave I & V in Adults = 4ms Children = 5ms Interaural latency of wave V, provided same suprathreshold stimulus has been presented = 0.3s. (correction factor is to be applied if hearing loss at 4000Hz is more than 50dB) High freq hearing loss inc the latency of wave V irrespective of whether a tumor is present/not.
- 73. AMPLITUDE not as constant as the latency, so not a very reliable parameter. WAVE MORPHOLOGY Normal graph has 5-7 peaks, each separated by a time interval of about 1ms. In NEWBORNS 3 peaks ; waves III & IV are inconspicuous. larger wave I and smaller wave V as compared to adults.
- 74. NON CLINICAL FACTORS EFFECTING BERA *stimulus rate. *stimulus phase/ polarity. *intensity of sound stimulus. *binaural/ monaural stimulation. *filter characters of BERA machine. *nature of sound stimuli used. *sex/age of the pt. NORMAL VALUES are for a clinic if- *60dB of suprathreshold stimulus. *stimulus rate of 10- 20 Hz. *rarefaction stimulus polarity. *age b/w 2-60yrs.
- 75. Parameter N in ms Abnormality I to III IPL 2 > 2.4 III to V IPL 2 > 2.4 I to V IPL 4 > 4.4 INTERAURAL LATENCY DIFF OF WAVE V < 0.3 > 0.3 MORPHOLOGY OF WAVE V PRESENT ABSENT
- 76. Clinical Uses- 1.Detection &quatification of deafness in difficult to test pts.(infants, MR, malingerers).For hearing threshold- *subtracting 5/10dB from the pt at which wave V is first identifiable. *multiplying the BERA threshold by 0.6 for readings ranging b/w 1-4 KHz. 2.Objectively determining nature of deafness. (sensory/neural). 3.Identification of site of lesion in retrocohlear pathologies. 4.Study of central auditory disorders. 5.Study of maturity of CNS in newborns.
- 77. FEATURES for a correct BERA tracing- -prominent waves I, III & V. -long negativity following wave V. -wave V be having the largest peak. -approx. 2ms gap b/w waves I & III and between waves III & V.
- 78. DERIVED BAND BERA -objective is to have a response from several discrete segments of the cochlea using click stimulus. -Cochlea arbitrarily divided into 5 discrete segments- 1= above 8000 Hz (extreme basal). 2= 4000- 8000 Hz. 3= 2000- 4000 Hz. 4= 1000- 2000 Hz. 5= 500- 1000 Hz (apical) Click sound and masking noise is given simultaneously to test ear and results obtained.
- 79. ADVANTAGE precise idea of neural activity from all different portions of cochlea is obtained. STACKED BERA is derived by stacking the derived band BERA. Hence, the sensitivity and specificity of the test are very high.
- 80. MLR ( Middle Latency Response) Occurs within first 50ms. Two successive positive peaks- Pa at 25- 35ms Pb at 40- 60ms Detects sound in low freq range. The peaks have some myogenic contribution. Esp from neck- reduces on relaxation of neck muscles. Affected by sleep and anaesthesia.
- 81. MAIN USES are audiological (not neurological) as- *waves are unstable. *contamination by myogenic potential. *neurogenic generators of wave peaks are controversial. ABNORMALITY suggests disorder in thalamo cortical region.
- 82. LLR (Late Latency Response) / CERA Elicited by tone pips of 1000/ 2000 Hz. About 50 stimuli are presented & response averaged by the computer. Within first 250ms of signal onset. It has a negative peak (N1) at 90ms and positive peak (P1) at 180ms. Best recorded when pt is awake & carefully respond ing as wave peaks depend on psychomatic factors like concentration & intelligence. It originates from the cerebral cortex.
- 84. Cohlea acts as a transducer. Elcetrical activity of cochlea and auditory nerve is measured.
- 85. Method Non Invasive Electrode placed on TM Invasive Electrode is a thin needle which is passed via the TM onto the promontory under LA/GA.
- 86. Parameters Measured -Cochlear microphonics( outer hair cell response) -Summating potential -Compound action potential (auditory N. activity) These parameters are measured within the first 5ms of stimulus.
- 87. USES 1. Diagnosis of Meniere’s Disease ratio of SP/AP > 0.45 whereas in normal it is < 0.4.
- 88. 2. Ascertaining hearing thresholds. the level of sound in dB HL at which compound action potential is just recorded. Average pure tone hearing level lies within few dB (5-10) of ECochG thresholds. 3. Monitoring integrity of cochlea and cochlear N. during neuro otological surgical procedures. 4. Helping in interpretation of BERA in cases when wave I isn’t identifiable. #Adv – C/L masking isn’t required.
- 89. Oto Acoustic Emissions(OAE) -They are low intensity sounds produced by outer hair cells of a normal cochlea. -Can be elicited by a very sensitive microphone placed in EAC. -Absent when OHC are damaged. -Thus serve to test cochlear functioning.
- 90. The pathway for OAE OUTER HAIR CELLS BASILAR MEMBRANE PERILYMPH OVAL WINDOW OSSICLES TYMPANIC MEMBRANE EAC
- 92. Spontaneous OAEs -Low intensity, continuous, very narrow band or pure tone sounds. -Detected in 50% of the subjects. -present more frequently in females. -more commonly in right ear. -Its absence doesn’t imply deafness in the tested ear.
- 93. Transient Evoked OAEs -Elicited by click stimuli and tone bursts. -They are not unstable and elicited by sounds of 80- 85dB. -Most commonly employed for neonatal hearing screening. -Response in one ear is suppressed if a sound is simultaneously presented to the other ear. -Do not occur in people with hearing loss >30 dB.
- 94. Distortion Product OAEs -Evoked when two different puretone sounds of two different frequencies are presented simultaneously to the ear.
- 95. f2 =f1 1.22 Frequency of evoked DPOAE is 2f1- f2. The response will represent the cochlear function of the f2 frequency region of cochlea.
- 96. -DPOAEs are absent in pts with SNL hearing loss greater than 40dB. -Absence of DPOAE in higher frequency is a sign of ototoxicity and noise trauma. -The best parameter for identifying hearing loss is the difference between the DPOAE level and the noise floor.
- 98. Hence, TEOAE more sensitive for low v hearing loss. DPOAE for high v hearing loss. TEOAEs usually done using click sounds and DPOAE using pure tone sounds, so more frequency specific.
- 99. Tone Decay Test -to be performed in all cases of SNL deafness esp if U/L. Principle- pathology in auditory nerve causes an abnormally rapid detioration in threshold of hearing of a tone, if tone presented continuously to the ear. Various methods- Carhart’s method - Green’s modified method - Olsen & Noffsinger Test - Rosenberg’s Method - STAT
- 100. Interpretation DECAY RANGE N Decay 0- 5 d Mild Decay 10- 15 dB Mod Decay 20- 25 dB Sev Decay >30 dB=RETRO COHLEAR PATHOLOGY
- 101. ABLB TEST -Can be preformed if there is significant difference in hearing thresholds i.e. 25dB. -The deafer ear is made the reference ear & better ear the variable one. Plotting of Results It is plotted as a laddergram.
- 103. Interpretation -Absence of recruitment- in case of SNL deafness s/o neural pathology. -Complete recruitment- cochlear pathology. -Partial recruitment.
- 104. SISI This test determines the capacity of a pt to detect a brief 1 dB increment in a 20dB suprathreshold tone in various frequencies. 20 as 1dB increments are given. The number detected multiplied by 5 gives the SISI score.
- 105. Interpretation 70-100%= cochlear 0-20% = retrocochlear Limitations pt with very severe deafness (> 85dB) cannot be tested as test done at 20dB suprathreshold level.
- 106. THANK YOU