LSCS in Chorioamnionitis at ICCOB 2021 Ahmedabad 181221
•Als PPTX, PDF herunterladen•
1 gefällt mir•640 views

Chorioamnionitis in pregnancy leads to PPROM, Preterm labour, maternal and fetal sepsis. Deliver is imminent. LSCS do not improve the fetal outcome in such patients.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie LSCS in Chorioamnionitis at ICCOB 2021 Ahmedabad 181221
Ähnlich wie LSCS in Chorioamnionitis at ICCOB 2021 Ahmedabad 181221 (20)
Mehr von Niranjan Chavan
Mehr von Niranjan Chavan (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
LSCS in Chorioamnionitis at ICCOB 2021 Ahmedabad 181221
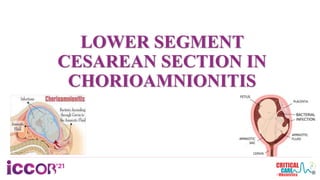
- 1. LOWER SEGMENT CESAREAN SECTION IN CHORIOAMNIONITIS
- 3. INTRODUCTION Chorioamnionitis or intraamniotic infection is an acute inflammation of the membranes and chorion of the placenta, typically due to ascending polymicrobial bacterial infection in the setting of membrane rupture.
- 4. Diagrammatic representation of sources of chorioamnionitis Tita AT, Andrews WW. Diagnosis and management of clinical chorioamnionitis. Clin Perinatol. 2010; 37(2):339- 354. doi:10.1016/j.clp.2010.02.003
- 5. Risk Factors • Prolonged labour • Nulliparity • Internal monitoring of labour • Multiple vaginal exams • Meconium-stained amniotic fluid • Smoking, alcohol or drug abuse
- 6. Risk Factors • Immune-compromised states • Epidural anaesthesia • Colonization with group B streptococcus • Bacterial vaginosis • Sexually transmissible genital infections and vaginal colonization with ureaplasma.
- 8. • Around 96% of cases are due to ascending infection, the remainder arise from haematogenous dissemination due to maternal septicaemia. Chorioamnionitis is usually polymicrobial. • The most common causes of chorioamnionitis are mycoplasmas, E. coli, group B streptococci and anaerobic bacteria. • Genital mycoplasmas are the most commonly isolated organisms associated with chorioamnionitis Causative Agents
- 9. Clinical Features • The key clinical findings associated with clinical chorioamnionitis include a. Fever(95–100% cases) b. Maternal tachycardia (>100/min) in 50-80%cases c. Fetal tachycardia (>160/min) in 40-70%cases and d. Uterine fundal tenderness and purulent or foul amniotic fluid in 4- 25% cases
- 10. • The combination of maternal fever and maternal and/or fetal tachycardia are strongly suggestive of intrauterine infection and should be treated accordingly. • Uterine fundal tenderness and a foul odour to the amniotic fluid are reported in only 4–25% of cases of chorioamnionitis, Purulence or foul odour of amniotic fluid are more likely to be present with severe or prolonged infection and may be organism-specific.
- 11. • Although PPROM is a major risk factor for clinical chorioamnionitis, it is noteworthy that together with preterm labor, PPROM frequently is the consequence of sub-clinical chorioamnionitis.
- 13. CBC : Maternal leukocytosis (variously defined as WBC >12,000/mm3 or >15,000/mm3) or the presence of a left shift or bandemia (>9%) often supports the diagnosis of chorioamnionitis. • Other laboratory parameters including high levels of • C-reactive protein (CRP), • Lipopolysaccharide binding protein (LBP), • soluble intercellular adhesion molecule 1 (sICAM 1) and • Interleukin 6 have been associated with a higher risk of chorioamnionitis in the setting of PPROM or preterm delivery
- 14. ORGANISMS CAUSING CHORIOAMNIONITIS • Chorioamnionitis is a polymicrobial infection most often due to ascending genital microbes; over 65% of positive amniotic fluid cultures involve two or more organisms. • Ureaplasma urealyticum 47% • Mycoplasma hominis 30% • These fastidious organisms provoke a robust inflammatory reaction affecting both maternal and fetal compartments, particularly in preterm gestations
- 15. • Gardnerella vaginalis (25%) • Bacteroides (30%), • Group B streptococcus (GBS, 15%) • Escherichia coli (8%) • Listeria monocytogenes (chorioamnionitis is the result of hematogenous spread of bacterial or viral infection to the placenta)
- 16. • An entity of “aerobic vaginitis”, (distinguished from bacterial vaginosis in that it represents a strong host immune response to aerobic vaginal flora typically comprised of GBS and E. coli) has been associated with ascending chorioamnionitis, PPROM and preterm birth.
- 17. Differential Diagnosis • Pyelonephritis • Influenza • Appendicitis • Pneumonia • Thrombophlebitis • Round ligament pain • Colitis • Connective tissue disorders • Placental abruption
- 18. Diagnostic Criteria: Lab Investigations
- 19. Clinical diagnosis is based on both maternal and fetal signs and symptoms: • Maternal pyrexia • Maternal tachycardia • Uterine tenderness • Offensive vaginal discharge • Fetal tachycardia.
- 20. Maternal Complications • 2 to 3-fold increased risk for cesarean delivery • 2 to 4-fold increase in endomyometritis • Wound infection • Pelvic abscess, • Bacteremia • Postpartum hemorrhage( due to dysfunctional uterine muscle contractions as a result of inflammation) • Very rarely: septic shock, disseminated intravascular coagulation, adult respiratory distress syndrome and maternal death
- 21. Fetal Complications • FIRS: is the fetal counterpart of the systemic inflammatory response syndrome (SIRS). • Since clinical parameters analogous to those defining SIRS are difficult to ascertain in the fetus, FIRS was originally defined by elevation of cord blood IL-6 in the setting of preterm labor and PPROM but can also occur in term gestations. • The histopathologic hallmarks of FIRS are • funisitis and • chorionic vasculitis
- 22. Fetal complications • FIRS has also been linked to preterm labor culminating in perinatal death and is associated, particularly among preterm neonates, with multi-organ injury, including chronic lung disease, periventricular leucomalacia and cerebral palsy. • Fetal exposure to genital mycoplasmas (U. urealyticum and M. hominis) has been associated with a fetal and neonatal systemic inflammatory response syndrome and pneumonia.
- 23. LSCS in Chorioamnionitis Management • The optimal antibiotic regimen for treatment of clinical chorioamnionitis has not been well-studied and current recommendations are based largely on clinical consensus . • Intravenous administration of ampicillin every 6 hours and gentamicin every 8–24 hours until delivery is the typical regimen. • If cesarean delivery is performed, clindamycin every 8 hours (or metronidazole) is often added for anaerobic coverage. • Optimal treatment should also include administration of a single intravenous additional dose of antibiotics after delivery (<5% failure rate); • Further oral antibiotic treatment is not beneficial in most cases.
- 24. Supportive measures • Antipyretics: This is particularly important during the intrapartum period since fetal acidosis in the setting of fever has been associated with a marked increase in the incidence of neonatal encephalopathy. • Treating intrapartum fever with antipyretics may also be helpful in reducing fetal tachycardia thereby avoiding the tendency to perform cesarean for a non-reassuring fetal status.
- 25. Women with clinical chorioamnionitis were more likely to have a cesarean delivery than those without clinical chorioamnionitis, and the risk of cesarean delivery varied significantly by hospital location, teaching status, and U.S. region.
- 26. • The first-line antimicrobial regimen for the treatment of clinical chorioamnionitis is ampicillin combined with gentamicin, which should be initiated during the intrapartum period. • In the event of cesarean delivery, patients should receive clindamycin at the time of umbilical cord clamping.
- 27. Optimal management of clinical chorioamnionitis includes antibiotic therapy and delivery. However, shortening the time between diagnosis and delivery by the performance of cesarean section in the setting of broad-spectrum antibiotic administration has been shown not to improve outcomes.
- 28. • Intraamniotic infection is a common condition noted among preterm and term parturient. Recognition of intrapartum intraamniotic infection and implementation of the treatment recommendations are essential steps that can effectively minimize morbidity and mortality for women and newborns. • Timely maternal management together with notification of the neonatal health care providers will facilitate appropriate evaluation and empiric antibiotic treatment when indicated. Intraamniotic infection alone is rarely, if ever, an indication for cesarean delivery.
- 29. • Chorioamnionitis is an indication for delivery; augment if not in established labour • Broad spectrum intravenous antibiotics • Reduce pyrexia with paracetamol and keep well-hydrated • Send Complete Blood Count, • Blood Cultures, • Low vaginal swab and • Mid-stream Urine for analysis.
- 30. Conclusion • Chorioamnionitis is a common infection of pregnancy, typically occurring in the setting of prolonged membrane rupture or labor. • It may be diagnosed clinically based on signs such as maternal fever, microbiologically based on amniotic fluid culture obtained by amniocentesis, or by histopathologic examination of the placenta and umbilical cord. • Chorioamnionitis is associated with postpartum maternal infections and potentially devastating fetal complications including premature birth, neonatal sepsis and cerebral palsy. •
- 31. Conclusion • The main preventative strategy is administration of antibiotics to women with preterm premature rupture of membranes which reduces the incidence of clinical chorioamnionitis, prolongs the time to delivery and improves neonatal outcomes. • Optimal management of clinical chorioamnionitis includes antibiotic therapy and delivery. • However, shortening the time between diagnosis and delivery by performance of cesarean section in the setting of broad spectrum antibiotic administration has been shown not to improve outcomes.
- 32. REFERENCES • Tita AT, Andrews WW. Diagnosis and management of clinical chorioamnionitis. Clin Perinatol. 2010;37(2):339-354. doi:10.1016/j.clp.2010.02.003 • Eschenbach DA. Ureaplasma urealyticum and premature birth. Clin Infect Dis. 1993;17 (Suppl 1):S100–6. • Soper DE, Mayhall CG, Dalton HP. Risk factors for intraamniotic infection: a prospective epidemiologic study. Am J Obstet Gynecol. 1989;161:562. • Newton ER. Chorioamnionitis and intraamniotic infection. Clin Obstet Gynecol. 1993;36:795. • Yoon BH, Romero R, Moon JB, et al. Clinical significance of intra-amniotic inflammation in patients with preterm labor and intact membranes. Am J Obstet Gynecol. 2001;185:1130. • Bommarito KM, Gross GA, Willers DM, Fraser VJ, Olsen MA. The Effect of Clinical Chorioamnionitis on Cesarean Delivery in the United States. Health Serv Res. 2016;51(5):1879-1895. doi:10.1111/1475- 6773.12447 • Bailit, J. L. , Gregory K. D., Reddy U. M., Gonzalez‐Quintero V. H., Hibbard J. U., Ramirez M. M., Branch D. W., Burkman R., Haberman S., Hatjis C. G., Hoffman M. K., Kominiarek M., Landy H. J., Learman L. A., Troendle J., Van V. P., Wilkins I., Sun L., and Zhang J.. 2010. “Maternal and Neonatal Outcomes by Labor Onset Type and Gestational Age.” American Journal of Obstetrics and Gynecology 2020 (3): 245