ABRUPTIO PLACENTAE (2) with animation
•Als PPTX, PDF herunterladen•
32 gefällt mir•12,772 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie ABRUPTIO PLACENTAE (2) with animation
Ähnlich wie ABRUPTIO PLACENTAE (2) with animation (20)
ABRUPTIO PLACENTAE (2) with animation
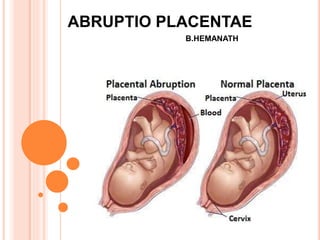
- 2. DEFINITION Abruptio Placentae(syn. Accidental haemorrhage, Premature placental separation): It is one form of APH where bleeding occurs due to premature separation of normally situated placenta.
- 3. TYPES Revealed Concealed or complete separation Mixed Marginal separation Partial separation Pre-placental separation Couvelaire uterus
- 4. TYPES
- 6. ETIOLOGY Predisposing factors • Hypertension in pregnancy • High Birth order • Advanced Age of mother • Smoking • Poor Socio Economic Status • Malnutrition Other Etiological Factors • Trauma • Sudden uterine decompression • Short Cord • Supine Hypotension syndrome • Placental Anomaly • Folic Acid deficiency • Placenta implanted over septate uterus • Torsion of uterus • Cocaine abuse • Thrombophilias • Prior abruption
- 7. PATHOGENESIS Etiological factors Haemorrhage into decidua basalis and hematoma formation Degeneration and necrosis of decidua basalis with adjacent placenta Rupture of basal plate forming communication b/w hematoma and intervillous space Fluid and blood percolate into myometrium upto serous coat(couvelaire uterus) Sometimes serosa split open and blood enters into peritoneal cavity
- 8. PATHOLOGY Usually retro placental hematoma not evident It is evident only after expulsion by features like depression on maternal surface with clot areas of infarction Couvelaire uterus Dark port wine colour Sub peritoneal petechial haemorrhages Free blood in peritoneum sometimes Other Organs Liver – fibrin knots in sinusoids Kidneys – ATN and ACN Shock proteinuria
- 9. CLINICAL GRADING Grade 0 • No Clinical Features. Diagnosis made after placental inspection following delivery Grade 1 • Vaginal bleeding slight • Uterus minimal tenderness • Maternal BP and fibrinogen levels normal • FHS good Grade 2 • Vaginal bleeding mild to moderate • Uterus tenderness present • Maternal pulse increased and fibrinogen levels decreased • Foetal distress or death Grade 3 • Vaginal bleeding severe • Uterus tenderness marked • Shock occurs • Foetal death is a rule associated with anuria coagulation defect
- 10. CLINICAL FEATURES: Revealed Mixed (Concealed predominate) Symptoms Abd. Discomfort followed by vaginal bleeding Acute abdominal intense pain followed by slight vaginal bleeding Character of bleeding Dark colour continuous Blood stained serous discharge continuous General condition Proportionate to visible blood loss Disproportionate shock usually present Uterine ht. Proportionate to GA Disproportionately enlarged Uterus feel Normal with local tenderness Tense, tender and rigid Fetal parts Easily identified Difficult FHS Present Absent UO Normal diminished
- 11. CLINICAL FEATURES: LABORATORY Revealed Mixed (Concealed predominate) HB% Low proportionate to blood loss Markedly lower disproportionate to blood loss Coagulation Profile Unchanged Variable changes Urine for protein May be absent Usually present
- 12. ULTRASONOGRAPHY To rule out placenta praevia but not diagnostic Early haemorrhage is hyperechoic or isoechoic Negative findings do not exclude placental abruption
- 14. DIFFERENTIAL DIAGNOSIS Revealed With placenta praevia With indeterminate bleeding Mixed or Concealed With rupture uterus With rectus hematoma With appendicular perforation With volvulus
- 15. PROGNOSIS Depends on Clinical types Degree of placental separation Interval b/w placental separation and baby delivery and efficacy of treatment Bleeding is almost always maternal
- 16. o Prevention • Elimination of known factors • Correction of anaemia • Prompt detection and institution of therapy to avoid complications o Treatment • At home:-treated as said in placenta praevia and shifted immediately to well equipped hosp. • At hosp :- Assessment of case Emergency measures Management options a) Definitive b) Management of complications c) Expectant management MANAGEMENT
- 18. THANK YOU