Pre prosthetic surgery (2)
•Als PPTX, PDF herunterladen•
314 gefällt mir•69,804 views

The document discusses preprosthetic surgery procedures for modifying the oral anatomy to facilitate denture retention. It describes various ridge correction techniques like alveoloplasty and mylohyoid reduction. It also discusses ridge augmentation procedures for both the maxilla and mandible using autogenous bone grafts harvested from different sites or alloplastic grafts like hydroxyapatite. Complications of these surgical techniques are also outlined. The goal of these preprosthetic surgeries is to establish an optimal bony foundation with adequate height, width, and contour of the residual alveolar ridges to support dentures.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Pre prosthetic surgery (2)
Ähnlich wie Pre prosthetic surgery (2) (20)
Pre prosthetic surgery (2)
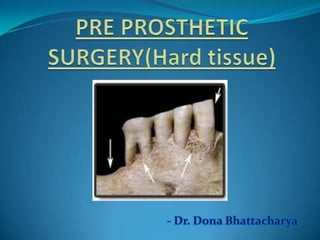
- 1. - Dr. Dona Bhattacharya
- 2. 1. Introduction 2. Objectives 3. Alveolar atrophy 4. Diagnosis & treatment planning 5. Ridge correction procedures a) Alveoloplasty b) Mylohyoid reduction c) Tuberosity reduction d) Genial tubercles reduction e) Removal of tori f) Removal of exostoses g) Removal of undercuts 6. Ridge augmentation 7. Conclusion 8. References
- 3. ∆ Preprosthetic surgery refers to the surgical procedures that can modify the oral anatomy to facilitate the retention of conventional dentures. ∆ According to the Glossary of Prosthodontic Terms (7), preprosthetic surgery is defined as surgical procedures designed to facilitate fabrication or to improve the prognosis of prosthodontic care. ∆ According to Bruce Donoff, preprosthetic surgery is that part of the oral and maxillofacial surgery designed to establish the best hard and soft tissue bases for prosthetic appliances.
- 4. ∆ Elimination of disease ∆ Conservation of oral structures ∆ Provide residual tissue to withstand masticatory forces ∆ Maintain function ∆ Esthetics
- 5. ∆ The term alveolar atrophy refers to the regression of the teeth-supporting, crescent-shaped osseous part of the upper and lower jaw.
- 6. Causes: ∆ Periodontal diseases ∆ Trauma ∆ Pt factors (age, gender, skeletal morphology) ∆ Endocrine & metabolic disorders (hyperparathyrodism,Ca defeciency) ∆ Dietary considerations ∆ Mechanical factors (extractions,removable denture wearers, combination syndrome)
- 7. Patterns of bone loss ∆ The results of Talgren’ s studies indicate that changes under the denture base more often occur in the mandible.(4:1) ∆ The difference in resorption of the jaws increases within the first year of denture wearing, which proves that the mandible cannot resist the strong bite forces under the denture base. ∆ According to Klemetti initially resorption starts on the alveolar part of the mandible, and the rest of the mandible remains unchanged. ∆ Resorption is faster in the labial and buccal parts of the alveolar ridge. (Resorptive Changes of Maxillary and Mandibular Bone Structures; Dubravka Knezovi et al, Acta Stomat Croat 2002; 261-265)
- 8. Class Characteristics Treatment I Alveolar ridge (AR) adequate in height but Hydroxyapatite (HA) alone inadequate in width, usually with lateral deficiency or undercut areas II AR deficient in both height & width and has a HA alone knife edge appearance III AR resorbed to level of the basilar bone, HA alone or mixed with producing concave form on posterior areas of the autogenous cancellous bone mandible and sharp bony ridge form with mobile soft tissue in the maxilla IV Resorption of the basilar bone, producing pencil- HA mixed with autogenous thin, flat mandible or flat maxilla cancellous bone (Mercier,1995)
- 9. Modifications: Class II-no wall defect/buccal wall/multiwall defect Class VI- marginal resection /continuity defect Atrophy of the Residual Alveolar Ridge Following Tooth Loss in a Historical Population; Reich, Karoline et al;"Oral Diseases 17, 1 (2010)
- 10. Functional effects of edentulism: ∆ The maxillomandibular relationship is altered in all spatial dimensions. ∆ Progression toward decreased overall lower facial height, leading to the typical overclosed appearance. ∆ Progressive instability of conventional soft tissue
- 11. Ideal denture base has following characteristics: a) Adequate bony support b) Soft tissue coverage c) No undercuts or protuberances d) No sharp ridges e) Adequate sulci f) Absence of peripheral scar bands g) no muscle fibres to mobilize prosthesis h) No soft tissue folds/hypertrophies i) No neoplastic lesions j) Proper maxillomandibular arch relationships k) Adequate palatal vault/tuberosity notching
- 12. 1. History ∆ Chief complaint ∆ Medical history 2. Physical examination Soft tissues a) Presence of mass b) Tenderness c) Frena d) Mucous membrane e) Muscle movements f) Relation of oral mucosa to gingiva
- 13. Hard tissues a) Undercuts b) Bony prominences c) Sharp ridges d) Ridge form e) Ridge parallelism f) Tuberosity notching Maxillo-mandibular relation Dentition 3. Investigations Radiographic a) Gen condition of dentition b) Bone resorption c) Proximity to imp structures d) Maxillo-mandibular relation Lab investigations
- 14. Patient selection: ∆ General physical status ∆ Age ∆ Anatomic factors
- 15. Preprosthetic procedures Ridge correction • Alveoloplasty • Mylohyoid reduction • Tuberosity reduction • Genial tubercles reduction • Removal of tori • Removal of exostoses • Removal of undercuts Ridge extension • vestibuloplasty Ridge augmentation • Maxillary • Mandibular
- 16. Defined as surgical recontouring of alveolar process History: ∆ Willard(1853) –removal of interdental papilla ,permitting edge to edge closure ∆ Beers(1876): radical alveolectomy ∆ De van(1930): trend towards conservatism had begun ∆ Molt(1923):use of study casts in planning alveolectomy ∆ Dean(1936):interseptal alveoloplasty ∆ Obwegesser(1966):modification of dean’s technique ∆ Michael & Barsoum(1976): study on post operative resorption
- 17. Principles: 1. Optimal ridge contour 2. Permit early construction of dentures 3. Preservation of alveolar bone 4. Broad alveolar ridges 5. Reduction of irregularities 6. Rounding off sharp ridges 7. Preserve cortical bone as much as possible 8. Defer surgery 4-6 weeks in case of severe periodontitis
- 18. Types Alveolar Simple Labial & Dean’s Obwegesser’s compression alveoloplasty buccal cortical intraseptal technique
- 19. ∆ Easiest & quickest method ∆ Involves compression of cortical plates with fingers ∆ Reduction in socket width
- 20. Indications: ∆ Reduction of buccal/labial plate ∆ Extraction of single/multiple teeth Technique: ∆ Single tooth extraction ∆ Multiple teeth extraction ∆ Over erupted teeth
- 22. Principles: a) Reduction of labial/alveolar prominences b) Muscle attachments are undisturbed c) Intact periosteum d) Preserve cortical bone e) Less post-op resorption
- 23. Indications: ∆ immediate dentures ∆ quadrant extraction Technique: Mac Kay’s modification(1964)
- 25. Extreme resorption results in sharp, pointed ridge that cuts into mucoperiosteum on pressure application. Pain occurs on wearing dentures.
- 26. Technique
- 27. Gillies(1956): Mylohyoid ridge should be reduced if found at same or higher level than alveolar process Roberts(1977): Reduction of mylohyoid ridge & extension of posterior lingual denture flange into retromylohyoid fossa Howe(1964): Mylohyoid ridge reduction is the most useful single operation
- 30. Excess tissue in the region of the maxillary tuberosity may become so large that it: ∆ Impinge upon the mandible during mastication. ∆ Interfere with denture construction, insertion and seating Complication of tuberosity reduction -expanded tuberosity in proximity to sinus
- 31. 3 techniques: Removal of tubercle followed by allowing genial muscle to reattach on its own. Removal of tubercle followed by repositioning of muscle with sutures fastened to chin. Removal of tubercle followed by transposition of muscle to inferior border.
- 33. ∆ Torus mandibular is an exostosis found on the lingual surface of the mandible opposite the canine and premolars region. ∆ Present in 8% of the population, with equal frequency in males and females ∆ Usually bilateral, (80% of affected patients), may be single, multiple or lobulated. ∆ Etiology: unknown, functional reaction to masticatory forces.
- 34. Indications for removal: ∆ Tori causing lingual undercuts and interfering with lingual flange extension of the planned prosthesis. ∆ When the mucosal covering is ulcerated. ∆ Large tori interfering with speech and deglutition Technique Complications
- 36. ∆ Torus palatinus present itself as an outgrowth in the midline of the palate. ∆ Shapes (single dome shaped, spindle shaped, nodular, lobular or multiple). ∆ Present in approximately 25% of all females ∆ Etiology unknown ∆ Composed of cortical bone; may have a cancellous component
- 37. Indications for removal: ∆ An extremely large torus filling the palatal vault. ∆ A torus that extend beyond the posterior dam area. ∆ Traumatized mucosa over the torus. ∆ Deep bony undercuts interfering with denture insertion and stability. ∆ Interference with function (speech, deglutition). ∆ Psychological considerations (malignancy phobia).
- 39. Complications: ∆ Haemorrhage ∆ Hematoma formation. ∆ Nasal or antral perforation. ∆ Sloughing and necrosis of palatal tissues. ∆ Fracture of palatine bone.
- 40. Found in maxillary molar region. Preservation of vascular supply: main concern during surgery
- 42. Caused by resorption in apical areas. Treatment: ∆ Excision ∆ Filling of undercut
- 43. Technique
- 45. Indications for Ridge Augmentation Progressive loss of denture stability and retention. Loss of alveolar ridge height, width and decreased vestibular depth and denture bearing area. Considerable basal bone resorption in the mandible, resulting in neurosensory disturbances. Increased susceptibility to fracture of the atrophic jaws. Replacement of necessary supportive bone. Altered interarch relationship
- 46. Ridge Augmentation Maxillary augmentation Mandibular augmentation Superior border Inferior border Onlay Onlay bone Interpositio augmentati augmentation grafting: grafting – Alloplastic Sinus Interpositional Visor nal / on (Iliac (Autogenous or Autogenou Autogenou onlay lift procedu / sandwich osteoto grafting sandwich crest, rib allogenic freeze s, allograft s / allogenic re bone grafts my grafts graft, dried cadaveric and grafts hydroxyapa mandible) alloplastic tite)
- 47. Graft: portion of a tissue or organ that after removal from its origin or donor site is positioned or inserted at a different place with the objective of reinforcing the existing tissues &/or correcting a structural defect.
- 48. Classification According to According to According to embryologic structure source origin Cortical Autograft Membranous Cancellous Allograft Endochondral Cortico- Xenograft cancellous Alloplast
- 49. Autogenous Grafts Distant sites Local sites •Rib •Chin •Iliac crest •Body and ramus •Calvarium •ZM buttress •Fibula •Coronoid •Tibia
- 51. AUGMENTATION OF SUPERIOR BORDER OF MANDIBLE (Davis, 1970) Indications: Remaining bone < 10 mm Ability of patient to tolerate procedure Donor considerations Recipient site
- 52. Kerfing of rib graft
- 54. Augmentation of inferior border of mandible Indications: ∆ Remaining bone < 10 mm ∆ Risk of pathologic # ∆ Management of malunion or non union of # Donor considerations Recipient site
- 55. ADVANTAGES No vestibule obliteration No dehiscence Less pain Better # stabilization 2o sulculoplasty not required Less bone resorption Indicated for pencil thin ridges Easier to perform skin graft vestibuloplasty DISADVANTAGES Scarring Presence of loose submandibular tissue Does not correct superior irregularities
- 56. AUGMENTATION OF MANDIBLE BY PEDICLED FLAPS Horizontal Vertical osteotomy/sandwich osteotomy/visor technique technique
- 57. Horizontal osteotomy (Danielson and Nemarich)/sandwich technique Indication ∆ reasonable amt of bone above mandibular canal ∆ b/l dimension<12-15mm
- 58. Technique Donor site Recipient site Lekkas modification
- 59. Vertical osteotomy (Harle,1975)/visor osteotomy Indications ∆ little bone above mandibular canal Technique
- 61. Combined vertical and horizontal osteotomy (Koomen et al) Advantages: ∆ Less risk of # ∆ Better sup & post repositioning of segment ∆ Correction of mild-moderate AP discrepancies ∆ Increase in amt of augmentation Technique Stoelinga modification
- 63. Bell & mc bride(1977)
- 64. Augmentation with synthetic graft materials: Hydroxyapatite is the prototype of the nonresorbable ceramic bone substitutes. It is a calcium phosphate material having physical and chemical characteristic nearly identical to dental enamel and cortical bone.
- 65. Technique
- 66. Advantages: ∆ Simple surgical technique suitable as an office procedure. ∆ No donor site is required to obtain autogenous bone graft material unless a composite graft is being accomplished. ∆ HA is totally biocompatible and nonresorbable ∆ Composite grafting can easily be accomplished as in severe class III and IV cases. ∆ Vestibular extension after alveolar augmentation is possible after 3 months of primary healing. ∆ Local augmentation is possible such as in bridge pontic areas. ∆ Metallic implant systems through HA augmented ridges are possible.
- 67. Complications: ∆ Dehiscence with extrusion of particles ∆ Abrasion through the mucosa with extrusion of the HA implant ∆ Infection ∆ Abnormal color is noted under the mucosa ∆ Mental nerve neuropathy
- 68. The use of particulate bone with membrane coverage allows for both horizontal and vertical augmentation of the mandible. The membrane is designed to prevent infiltration of the particulate graft with connective tissue and allow bone to infiltrate into the particulate graft mass rather than connective tissue, with the formation of sufficient bone. Disadvantage: ∆ premature exposure of the membrane through the mucosa. ∆ infection Used for ant maxillary combination syndrome
- 69. Grafting bone on the superior surface of the residual alveolar cortical bone is accomplished by first gaining access to the cortical bone, placing and securing a bone graft to the region to be augmented, and closing the soft tissue. Indication: class V Advantage: 1. avoidance of direct damage to the IAN 2. ease of placement of the graft 3. immediate postoperative vertical augmentation. Disadvantage: incision breakdown over the graft can result in a reduction of the long- term augmentation
- 70. Mandibular Tori as a Source for Onlay Bone Graft Augmentation: A Surgical Procedure; Scott D. Ganz JPPA;2007
- 71. After alveolar bone osteotomy,distractor device is placed in transport segment, which remains vascularized via periosteum Latency period(5- 7 days) Bony segment subjected to traction Distraction period(0.5- 1mm/day 1-4 times Activation of tissue growth & regeneration Consolidation period(8-12 weeks) Formation of distraction callus, matures into bone
- 72. Indications: ∆ Moderate-severe alveolar bone defects ∆ Segmental deficiencies ∆ Adjuvant to other grafts ∆ Less b/l width of ridges
- 73. Simple, less resorption, include teeth, implants in transport segment, less time
- 74. Accurate diagnosis of the problem areas during denture construction and determination of the necessity of surgery is accomplished by careful evaluation of the information systematically obtained from the patient. As conservation is the philosophy of surgical patient management. therefore every attempt should be made to preserve as much as oral structures as possible. Proper knowledge of the available surgical procedures helps in achieving the best results.
- 75. 1. Preprosthetic oral & maxillofacial surgery-Starshak & Sanders 2. Textbook of oral & maxillofacial surgery- Laskin vol II 3. Principles of oral & maxillofacial surgery-Peterson 4. Textbook of oral & maxillofacial surgery- Fonseca vol 7 5. Textbook of oral & maxillofacial surgery- Kruger 6. Textbook of oral & maxillofacial Surgery – Archer 7. Textbook of oral & maxillofacial surgery- Killey And Kay 8. Bone grafting in oral implantology: Alfaro
- 76. 9. Alveolar bone grafting techniques for dental implant preparation- OMFS,Aug 2010 10. Sugar,Hopkins et al:A sandwich mandibular osteotomy, BJOMS, 1982, 20:168 11. Interpositional Osteotomy for Posterior Mandible Ridge Augmentation Michael S. Block, DMD,* Christopher J. Haggerty.JOMS 67:31-39, 2009, Suppl 3 12. Distraction implants: a new operative technique for alveolar ridge augmentation Alexander Gaggl, Gfinter Schultes, Hans K~ircherJournal of Cranio-Maxilloj'acial Surge , (1999) 27, 214-221 13. Reconstruction of the severely atrophic mandible with iliac crest grafts and endosteal implants: a report of two cases; O’Connell J.E. ,Galvin M, Journal of the Irish Dental Association 2009; 55 (5): 237-241. 14. Mandibular Tori as a Source for Onlay Bone Graft Augmentation:A Surgical Procedure Scott D. Ganz,JPPAD
Hinweis der Redaktion
- Tuberoplasty,sinus lift