Recent trends in management of undescended testes
•Als PPTX, PDF herunterladen•
53 gefällt mir•11,274 views

summary of UDT and its management from recent articles and books

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Recent trends in management of undescended testes
Ähnlich wie Recent trends in management of undescended testes (20)
Mehr von Awaneesh Katiyar
Mehr von Awaneesh Katiyar (19)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Recent trends in management of undescended testes
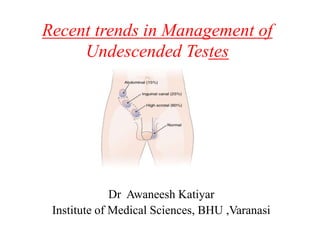
- 1. Recent trends in Management of Undescended Testes Dr Awaneesh Katiyar Institute of Medical Sciences, BHU ,Varanasi
- 2. Introduction • Definition:- Failure of the testis to descend into the scrotum. • Most common genital disorder identified at birth. • Premature infants- 33% • Full term at birth- 2-4% • At age 1 year- 1%
- 3. • Unilateral : Bilateral 68% : 32% • Right : Left 70% : 30% • Palpable : Nonpalpable Testes 80% : 20% Left undescended testis
- 4. Development of testis • Early life of embryo • Germ cells- Primordial germ cells
- 5. • Coelomic epithelium • Medial side of mesonephros • Gonadal ridge- migration of primordial cells(4-6wks)
- 6. • 7th week – testicular differentiation • 8th week testis hormonally active – Sertoli Cell : MIS – Leydig cell : Testosterone • 10-15th week external genital differentiation
- 7. Descent of Testis • The gubernaculum, the guide for testicular descent. • Hormone testosterone and INSL3 peak between 14 and 17 weeks’ - critical for testicular descent.
- 8. Phases of testicular descent Barteczko and Jacob (2000) • Phase 1: 5 weeks - The caudal mesonephros contacts the future gubernaculum at the internal inguinal ring. • Phase 2: 7 weeks -The genitofemoral nerve accompanies the newly formed gubernaculum and processus vaginalis. • Phase 2a: 8 to 10 weeks - Growth of the gubernaculum. • Phase 3: 10 to 12 weeks - Gubernaculum remains a thin cord in both sexes.
- 9. • Phase 3a: 12 to 14 weeks - The testis overrides the genital ducts and contacts the gubernaculum. • Phase 4: 14 to 20 weeks - Migration of the processus vaginalis produce widening of the inguinal canal • Phase 5: 20 to 28 weeks - Release of the distal subcutaneous attachment of the gubernaculum and transinguinal passage of the testis. • Phase 5a : after 7th month – Caudal movement of the testis, regression of the gubernaculum .
- 10. Factor affecting testicular descent Mechanical Hormonal • Gubernaculum • Cranio-gonadal ligament • Intra-abdominal pressure • Inguinal Bursa • Processus Vaginalis • Androgen & its receptor • INSL3 & Its receptor • Estrogens • Anti-Mullerian–Inhibiting Substance • Calcitonin Gene Related Peptide • Epidermal Growth Factor
- 11. Mechanical Factors • Gubernaculum – John Hunter(1762) coined term Gubernaculum. • Important- Mechanical Factor • Mesenchymal band Lower pole of testis to scrotum
- 12. • INSL3 Mediates - Outgrowth phase • Androgen Mediates - Regression phase
- 13. Hormonal Factors Androgen and its receptor • Engle (1931) – Intact hypothalmic-pituitary- testis axis is essential for normal testicular descent. • Cryptorchidism associated with – Hypogonadism – Androgen insensitivity – CAIS
- 14. Estrogens • Estrogens – Impairs gubernacular development and to cause persistence of müllerian duct derivatives. • Gill and associates – increased incidence of cryptorchidism in male offspring of women treated during pregnancy with DES. • Bernstein and colleagues- male infants born to mothers with high levels of free estradiol- had higher frequency of cryptorchidism
- 15. Testicular ascent • In past – considered as misdiagnosis caused by an error in physical examination. • 32%- 50% - in retractile testis. • Typically unilateral (77%) • Identified at mid-childhood. • Located distal to the inguinal canal.
- 16. Lockwood theory of Ectopic testis • Multiple gubernaculum / tails present to anchor testis from base. • When scrotal tail gets ruptured or weakened at any point, • Accessory tails act and pull Ectopic testis
- 17. Positions of the ectopic testis. The ectopic testis can be identified in various positions, as shown. The most common location is the superficial inguinal pouch. Contralateral scrotum Perirenal Peripenile Superficial inguinal Transverse scrotal Femoral Perineal
- 18. Risk Factors for UDT • Maternal & Gestational Factors – Maternal Obesity – Low birth weight – Prematurity (Hakonsen et al, 2014). Maternal smoking- small-to-moderate increased risk for cryptorchidism is present in offspring.
- 19. Genetic Factors • 14% of cryptorchid boys – have positive family history. • Multifactorial pattern transmission • Father affected – 4% • Sibiling affected – 6-10 % • Gene mutation have identified -cryptorchidism – INSL3 – LGR8 – Androgen receptor polymorphism – HOXA10 – HOXD13
- 20. Environmental • Prenatal exposure - endocrine disrupters – DES – Pesticide (DDT) – Nonylphenol – Natural phytoestrogens – Phthalates etc.
- 21. Syndromes Associated with UDT • Reduce androgen production and/or action, such as androgen biosynthetic defects, • Androgen insensitivity • Leydig cell agenesis, • Gonadotropin deficiency disorders. • Klinefelter syndrome (47,XXY)( 1.8%), • Down syndrome (trisomy 21),
- 22. • All cases of classic prune-belly • 80% of those of spigelian hernia • 41% - 54% of cerebral palsy • 15% of myelomeningocele • 16% - 33% of omphalocele, • 5% - 15% of gastroschisis • 19% of imperforate anus • 12% - 16% of posterior urethral valve • 6% of umbilical hernia
- 23. Complications of Undescended Testis Undescended testis Torsion Reduced fertility Trauma Testicular tumor Epididymo -orchitis Inguinal Hernia
- 24. Reduced fertility • Decreased fertility – well known consequence of cryptorchidism. • 10-13% boys with – Unilateral UDT • 33-36% boys with – Bilateral UDT • Retractile testis – Intrinsically normal.
- 25. Investigations • Undescended testis - clinical diagnosis. • Clinically palpable testis – no role of imaging • Non palpable testis – Imaging – Hormonal assessment – Laparoscopy
- 26. Imaging Methods Ultrasonography • Most commonly used study • A meta-analysis of 12 studies low sensitivity (45 %) and specificity (78 %).
- 27. • Other imaging tool like CT scan or MRI is not recommended. • Hazard of ionizing radiation- CT scan. • MRI – overall sensitivity for detection -62% – 55% - totally intra-abominal – 86% - for inguinoscotal • MRI – poor test for atrophied testis
- 28. Diagnostic Laparoscopy • Gold Standard for non-palpable testis. • Possible anatomic finding – The spermatic vessels enters the inguinal canal (40%). – A canalicular or peeping testis (11.2%). – The Spermatic vessels end blindly (9.8%). – A Viable intra-abdominal testis (37%).
- 29. Management of undescended testis • Cryptorchid testis should be treated – between 6 month to 1 year of age. • 12-18 months – histological deterioration of the testis noted. • Testis rarely descends – after 6 months. • Surgical advantage to Orchiopexy- within 6 months specially in high undescended testis.
- 30. Undesceded testis unilateral palpable Non palpable surgery Refer to 6 months Low testis Hormone therapy Failure surgery Normal external Genitalia Hypospadias or ambigous genitalia Diagnostic therapeutic laparoscopy or open surgery Pre-op hormone therapy Hormone therapy failure High testis Not Intersex Refer to 6 months Newborn Older child
- 31. Bilateral Palpable Palpable Intersexual Management by diagnosis Refer to 6 months Hormone therapy for low testis Failure surgery surgery Measure LH, FSH, MIS, hCG stimulation test Positive Negative Laparoscopy or open surgery Probable agonadal consider surgery NonpalpableNonpalpable Undesceded testis
- 32. Non-surgical Only used for palpable or unilateral UDT Surgical Hormonal therapy Palpable Nonpalpable Inguinal / scrotal orchidopexy evaluate High inguinal Intra- abdominal Laparoscopic surgery/ open Management
- 33. Hormonal therapy hCG (human Chorionic Gonadotropin) • Stimulate endogenous secretion of testosterone. • Therapeutic dose – 1500 U/ m2 body surface area twice in a week for 4 weeks (FDA approved). • Total dose should not exceed 15,000 units. • Testicualar descent rate – 25% with hCG – 18 % with GnRH
- 34. • LHRH- 1.2 mg/ day in divided doses intranasal for 4 weeks . • Testicular descent rate –about 20%. • Not FDA approved • Boserelin – superanalogue of LHRH – Small dose- 10µg every other day for 6 months. – Descent rate – 17%
- 35. Hormonal assessment for bilateral Non -palpable testes Cryptorchidism Anorchidism Female Pseudohermaphroditism Karyotype 46,XY 46,XY 46,XX Serum testosterone Baseline Normal Low Variable hCG stimulation test Positive Negative Negative Gonadotropins Normal incresed Normal AMH/MIS Positive Negative Negative Adrenal steroid precursors Normal Normal increased
- 36. Surgical Management • Palpable testes • one stage orchidopexy • Non- palpable testes • Laparoscopy / open • High incidence of congenital inguinal hernia (hernia repair) • Retractile or ectopic testes • Cremasterotomy
- 37. Principles of orchidopexy (described by Bevan in 1899) • Adequate exposure • Herniotomy • Mobilization of cord • Fixation of testis
- 38. Inguinal Orchidopexy • Most commonaly performed – creation of subdartos pouch and placing the testis. • General anesthesia; useful to re-examine the child- previously nonpalpable testis may become palpable. • Groin crease incision is made Careful dissection to expose the external oblique aponeurosis and the external ring.
- 39. (Adapted from Hinman F, Baskin LS. [2009] Hinman’s atlas of pediatric urologic surgery. Philadelphia: Elsevier.)
- 41. • The gubernaculum is divided
- 42. • A high ligation of the hernia sac is performed, and the remaining structures are skeletonised
- 43. • Stephen-Fowler’s technique- – when cord length is still required – soft clamp is applied to the testicular artery – viability of testis is checked. – If it is viable testis can bring down safely to the scrotum.
- 44. Obsolete procedure • Ombredanne’s operation- when testis is passed into the opposite scrotum through an opening on the scrotal septum. • Ladd and gross procedure - after placing the testis in the scrotal pouch, it is fixed by a polypropylene suture into tunica albuginea, across scrotal skin and into the thigh skin outside.
- 45. • Keetley – Torrek procedure - testis is mobilized and is brought into the scrotal pouch first. A pouch is created on the medial aspect of thigh outer to the fascia lata. Testis is delivered from scrotal pouch is placed into the thigh pouch.
- 46. Trans-scrotal Orchidopexy • Testes that are low in the canal believed to be ectopic are good candidates for trans-scrotal approach. • Incisions – Superior scrotal – Low scrotal – Midline scrotal
- 47. Surgery for the Non palpable Testis • Examination under anaesthesia- remains non- palpable. • Laparoscopy - Gold standard Conclusion: Results of open versus laparoscopic orchiopexy procedures (primary or staged) are fairly comparable. However, laparoscopy provides significantly less morbidity.
- 48. • Contraindications to laparoscopy – – Prior abdominal surgery with potential peritoneal adhesions. – A body habitus that will not allow for proper placement of abdominal wall ports.
- 49. • Laparoscopy - best means of identifying intra- abdominal testis, vas and vessels. • If laparoscopy indicates blind-ending gonadal vessels and vas deferens, the patient is said to have vanishing testis syndrome and no further action is necessary
- 50. High left testis Closed internal ring Blind-ending vessels Vas deferens High intra-abdominal testis identified on laparoscopic evaluation. Left testis identified high in the abdomen is associated with a closed internal ring. Vanishing testis noted on laparoscopic evaluation. Note the blind-ending spermatic vessels and vas deferens.
- 51. • If intra-abdominal testis identified consider staged orchidopexy or microvascular transfer. • If vas vessels seen entering inguinal canal, the groin should be explored. • The length of the gonadal vessels is the limiting factor to getting the intra-abdominal testis into the scrotum.
- 52. Conclusion- • Vasa and vessels blind ending above the IR as the only finding that would benefit from laparoscopy only. • If testis is not visualised and vessels are going into IR , surgical exloration is mandatory to avoid clinical as well as legal long term follow up.
- 53. Laparoscopic procedures 1. Primary one-stage orchiopexy with preservation of the spermatic vessels 2.Division of the spermatic vessels as the first stage of a two-stage Fowler-Stephens orchiopexy The second stage of a two-stage Fowler-Stephens orchiopexy can also be performed laparoscopically. 3. Orchiectomy.
- 55. • Mobilization of any structures extending distal to the internal ring, including epididymis/vas and Gubernacular remnant testis
- 56. • Transection of the peritoneum lateral to the vessels and distal to vas. • Proximal mobilization of the vessels while maintaining collateral blood supply between the vas and spermatic vessels if a Fowler-Stephens maneuver becomes necessary ( short spermatic cord) (Adapted from Hinman F, Baskin LS. [2009] Hinman’s atlas of pediatric urologic surgery. Philadelphia: Elsevier.)
- 57. • Initial mobilization of the gubernaculum to be used as a handle for further mobilization of the testis, and minimal use of cautery during this maneuver. • Ability to mobilize the testis to the opposite internal ring has been used as a measure of adequate length for placement in the scrotum but is not predictable in some series. • Once mobilized, the testis is brought through a new hiatus at the level of the medial umbilical ligament or through the existing internal inguinal ring.
- 58. 1. Standard single stage orchidopexy 2. A two-stage Fowler-Stephens orchidopexy The testicular artery is sacrificed. • The rationale is that the testicular arterial supply comes from three sources. • At a 2nd stage (after 6 months of age, when collaterals have formed), the testis is brought down on a wide pedicle of peritoneum containing the remaining vessels.
- 59. Many recent studies supported that laparoscopic Orchidopexy better than open for non palpable techniques.
- 60. Open procedures for Non- palpable testis • Abdominal approach – Transperitonial approach – Extraperitonial approach • Inguinal approach – Extended inguinal approach
- 61. Microvascular testicular autotransplantation • For high intra-abdominal testis • Reserved for older children with internal spermatic artery large enough to be anastomosed to inferior epigastric artery.
- 62. Autotransplantaion of testes using microvascular technique (silber and kelly ) principle: cutting of spermatic vessels and re-anastmosis to inf. Epigastric vs using 10/0 sutures under microscopy.
- 63. Refluo Testicular Autotransplantation • Provides only venous drainage by microvascular anastomosis of testicular veins to inferior epigastric veins • Based on discovery that failure in Fowler- Stephens was due to testicular congestion
- 64. Orchidectomy : Usually reserved for postpubertal men with a contralateral normally positioned testis.
- 65. Postoperative Complications • Haematoma • Infection • Unsatisfactory position (requiring revision), • Ilioinguinal nerve injury • Damage to the vas • Testicular atrophy • Torsion testis.
- 66. CONCLUSION • The etiology of testicular maldescent remains unknown. • Knowledge of hormonal correlation with undescended has improved. • For palpable testis - Inguinal Orchidopexy remains gold standard.
- 67. • Recent advancement in laparoscopic tool has significantly changes management of UDT. • Diagnostic Laparoscopy, replaces all imaging modalities including Ultrasonography & MR. • Open Orchidopexy to Laparoscopic Orchidopexy for non palpable testis.