Management of hodgkin lymphoma.pptx123
•Als PPTX, PDF herunterladen•
5 gefällt mir•1,139 views

management of hodgkins lymphoma

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Management of hodgkin lymphoma.pptx123
Ähnlich wie Management of hodgkin lymphoma.pptx123 (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Management of hodgkin lymphoma.pptx123
- 1. MANAGEMENT OF HODGKIN’S LYMPHOMA • PRESENTER:- DR ABDUL WAHEED • Post graduate • Skims srinagar kashmir
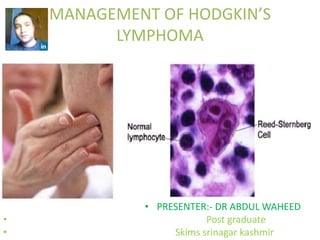
- 2. INTRODUCTION • Are group of cancer which originates from reticuloendothelial system • It was named after thomas hodgkin who first described it in 1832 • Dorothy reed and carl stenberg first described the malignant cells of hodgkins lymphoma called reed sternberg cells. • Hodgkins lymphoma was the first cancer which could be successfully treated by radiation therapy and also by combination chemotherapy.
- 3. Anatomic disribution of disease • >80% of patient present with invovement of cervical nodes; > 50% have mediastinal disease,12% with axillary nodes ;and 9 percent with inguinal nodes. • Involvement of the spleen is dependent on histologic subtype. • It is involved in 60 percent of mixed cellularity and lymphocyte-depleted cases compared with 34 percent of nodular lymphocyte predominant and nodular sclerosis cases. • Isolated extra lymphatic involvement in the absence of nodal disease is rare.
- 4. Theories for anatomic distribution • Contiguity’’ theory of kaplan and rosenberg and the ‘suscepitibility’ theory of smithers. • In support of the former ,most cases of hodgkins lymphoma appear to spread via lymphatic channels to contiguous lymphatic structures in a predictable nonrandom pattern. • Controversy has surrounded the mode of spread of spleen ,which lacks affrent lymphatics. • When four or more lymph node regions were involved ,possibility of spread by hematogenous distribution appeared more likely • Disseminated disease is more common in mixed cellularity and lymphocyte-depleted cases ,consistent with the presence of reported vascular invasion.
- 5. NATURAL HISRTORY • HODGKINS lymphoma arises in a single node or chain of nodes and spread first to anatomically contiguous lymphoid tissue. • Visceral involvement by hodgkins lymphoma may be secondary to extension from adjacent lymph nodes. • Haematogenous spread occurs to liver or multiple bony sites. • It rarely involves the gut associated lymphoid tissue such as waldeyer ring, peyers patches, upper aerodigestive tract, cns and skin. • Mechanism of spleen involvement is unclear but all pts with hepatic and bone involvement are associated with splenic involvement.
- 6. Epidemiology • Incidence of HL in the UK and USA is 2.7–2.8 per 100 000 per year, with roughly 1700 new cases diagnosed in the UK every year • Lower in developing countries, India 1-1.6/100000 • 8th most common in males and 7th in females • Males>females 1.2:1 • Bimodal 20-35 and 55 years • Younger patients have nodular sclerosis • It is rare in children younger than 10 yr • But <10 years Mixed cellularity is common
- 7. 0 20 40 60 80 100 120 140 160 180 YEAR2009 YEAR2010 YEAR2011 YEAR2012 YEAR2013 YEAR2014 YEAR2015 130 157 112 120 126 143 163 LYMPHOMA LYMPHOMA
- 8. ETIOLOGY • Environmental: Increased risk- wood, meat workers, farmers • Ataxia telangiectasia associated with immunodeficiency syndrome • Assosiated with Viral-EBV infection mainly with mixed cellularity • Genetic predisposition:increased incidence in Jews and also among first-degree relatives. • Siblings 2-5 fold increased risk; in siblings of the same sex there is as much as a 9 fold increased risk. • Higher socioeconomic status • Associated with infectious mononucleosis .incidence is about 2.55 times higher. • Prolong use of human growth hormone
- 9. • There is increasing evidence connecting the prevention of apoptosis and survival of HRS cells to the activation of the nuclear factor kappa B (NFκB) transcription factor-signaling pathway. • Constitutive NFκB is required for proliferation and survival of Hodgkin’s lymphoma tumor cells. • The cause of the constitutive activation of NFκB is probably multifactorial and may include amplification of the REL gene, mutations in NFκB inhibitors, and somatic mutations in the novel tumor suppressor gene TNFAIP3. • There is an inverse relationship between EBV infection and inactivation of A20, the protein encoded by the TNFAIP3 gene, suggesting that they may represent alternative pathways of pathogenesis. • One of the regulators of apoptosis that is expressed in dependence of NFκB is cIAP2, a direct inhibitor of caspase 3, suggesting that HRS cells are protected from caspase 3-induced apoptosis by cIAP2. • Another NFκBdependent regulator of apoptosis is CD95, which has been shown to be up-regulated in HRS cells.
- 10. Clinical Presentation • Nontender lymph nodes enlargement ( localised ) – neck and supraclavicular area 60-80% – mediastinal adenopathy 50% – other ( abdominal, extranodal disease ) • systemic symptoms (B symptoms) 30% – fever – night sweats – unexplained weight loss (10% per 6 months) • other symptoms – fatigue, weakness, pruritus – cough , chest pain, shortness of breath, vena cava syndrome – abdominal pain, bowel disturbances, ascites – bone pain – Alcohol induced pain over involved lymph nodes – Nephrotic syndrome ,erythema nodosum,cerebellar degenration.
- 11. Staging evaluation for Hodgkin’s Disease • Essential – physical examination – documentation of B symptoms – laboratory evaluation • complete blood count, ESR • liver function tests • renal function tests • lactate dehydrogenase – chest radiograph AP & Lat 60% have intrathoracic involvment >1/3rd tarns thoracic diameter at the diaphragm >35% of the thoracic diameter at T5-T6 – ultrasonography – CT scan of chest, abdomen and pelvis: standard – pathologic documentation by hemopathologist
- 12. PET SCAN • Pet scan has become an integral component of intial staging • Information provided by pet has been recently incorporated in the lymphoma guidelines for response evaluation after completion of treatment. • Useful for follow up study to evaluate masses, dx of early recurrence and predicting outcome • It has a specificity of 90-95%
- 13. Role of PET • PET can be used in combination with CT scan staging, end-of-treatment and interim assessments, & follow-up surveillance • PET at diagnosis upstaged 13–24% more patients than did CT scan. • Distinguish between fibrotic tissue and residual active disease • interim assessment after initial cycles of chemotherapy, with the aim of identification of which patients are cured and which need escalation of treatment Danish & Italian groups indicated interim PET as a good predictor of response in HL • GHSG HD 15 – advanced HL residual lymphoma >2.5cm underwent PET • PET-Negative – no RT Positive - IFRT • There are several unresolved questions relating to the reproducibility and quality control of 1⁸F-FDG PET and the standardised interpretation of minimum uptake.
- 15. Bone marrow biopsy less commonly put into practice. overall involvement of bone marrow in hodgkins lymphoma is 5%. Indicated in pts with – b symptoms. – clinical evidence of sub diaphragmatic disease. – stage IIB to IV disease. – Recurrent disease.
- 16. • Essential under certain circumstances(complementary) – liver biopsy – gallium scan – technetium bone scan – bone radiographs – MRI – bipedal lymphangiogram – staging laparotomy • Useful but not essential tests – cell-surface marker phenotypic analysis – gene rearrangement analysis
- 17. Staging Classification Ann Arbor modified by Cotswolds • Stage I: involvement of single lymph node region or lymphoid structure • Stage II: involvement of two or more lymph node regions on same side of diaphragm • Stage III: involvement of lymph node regions or structures on both sides of diaphragm III1: with splenic hilar, celiac,portal nodes III2: with para-aortic, iliac,mesenteric nodes • Stage IV: involvement of extranodal site(s) A. Asymptomatic B. Symptomatic (B symptoms) X. Bulky disease ( > 1/3 widening of mediastinum, > 10cm max.dimension of nodal mass) E. Involvement of a single, localised, extranodal site
- 19. Pathology • Hodgkin lymphomas are defined as lymphomas containing one of the characteristic types of RS cells in a background of nonneoplastic cells; cases are sub classified according to the morphology and immunophenotype of the RS cells and the composition of the cellular background. • RS or diagnostic cells—represent the body of the tumour: they measure 20–60 μm in diameter and display a large rim of cytoplasm and at least two nuclei with acidophilic or amphophilic nucleoli, covering more than 50% of the nuclear area. • only 0.1% to 1% of the entire cell population in all subtypes of classic HL • Can be seen in NHL, IM, carcinomas and sarcomas. • Lymphocyte-predominant subtype of HL, HRS cells consistently express B- cell specific surface antigens (CD19, CD20), in classic HL HRS cells express the activation marker CD30, and in the majority of the cases CD15 • L&H cells have vesicular, polylobated nuclei and distinct but small, usually peripheral, nucleoli without perinucleolar halos. • CHL and LPHL represent monoclonal, B-cell derived disorders.
- 20. Diagnosis of HL require : 1. Identification of characteristics neoplastic cells, classic RS cells and several elements including lacunar cells, mononuclear cells and pleomorphic variants and lymphocytic histiocytic cells 2. background of non-malignant lymphocytes, plasma cells, neutrophils, eosinophils, histiocytes and stromal elements. 3. disruption of nodal architecture.
- 21. Classification Jackson and Parker Lukes and Butler Rye Conference REAL Classification WHO Classification 1944 1966 1966 1994 1997 Paragranuloma (10%) Lymphocytic and/or histiocytic, nodular Lymphocytic and/or histiocytic, diffuse(15%) Lymphocyte predominant Nodular lymphocyte predominant(5%) Classic HL Lymphocyte-rich classic HL Lymphocyte predominant, nodular Classic HL Lymphocyte-rich classic HL Granuloma (80%) Nodular sclerosis Mixed cellularity Nodular sclerosis Mixed cellularity Nodular sclerosis Mixed cellularity Nodular sclerosis Mixed cellularity Sarcoma (10%) Diffuse fibrosis(5%) Reticular Lymphocytic depleted(rare) Lymphocyte depleted Lymphocyte depleted Unclassifiable classic HL
- 22. Comparison Antigen Classic HL(RS cells) Nodular lymphocyte predominant(L&H cells) Pattern Diffuse, interfollicular, nodular Nodular, at least in part Tumor cells Diagnostic RS cells; mononuclear or lacunar cells L&H or popcorn cells Background Lymphocytes, histiocytes, eosinophils, plasma cells Lymphocytes, histiocytes Fibrosis Common Rare CD20 Occasionally + Usually + Other B-cell antigens Usually - Usually + CD30 + - CD15 Usually + - CD45 - + EBV in RS cells +(50%) - CD57+ T cells - + Ig expression Absent Present
- 23. Risk factors for early stage HL Group Risk Factors Treatment Groups EORTC Large mediastinal mass Favorable: stage I-II without risk factors Age > 50 yr Unfavorable: stage I-II with one or more Elevated ESR, B symptoms* risk factors 4 or more involved regions GHSG (Germany) Large mediastinal mass Favorable: stage I-II without risk factors 3 or more involved regions Intermediate: stage I or stage IIA with 1 Elevated ESR, B symptoms* or more risk factors Extranodal disease Stage IIB with elevated ESR and 3 or more involved regions ECOG AND NCI-C Histology (MC, LD) Favorable: stage I-II without risk factors (USA) Age >40 y Unfavorable: stage I-II with one or more Elevated ESR or B symptoms risk factors 4 or more involved regions NCRI(UK) Bulky disease, B symptoms Early stage=no adverse factors; advanced stage =≥1 risk factor
- 25. INTERNATIONAL PROGNOSTIC SCORE FOR ADVANCED HODGKINS LYMPHOMA • Serum albumin <4 g/dL 1.49 • Hemoglobin <10.5 g/dL 1.35 • Male gender 1.35 • Stage IV disease 1.26 • Age >45 y 1.39 • WBC >15,000/mm3 1.41 • Lymphocyte count <600/mm3 1.38 or <8% WBC
- 27. Treatment • Most patients with HL are cured with first-line therapy. • The main challenges are to reduce the toxic effects of treatment while maintaining excellent outcomes, and to improve survival for patients with poor-risk, refractory, or relapsed disease. • Gilbert, a Swiss radiotherapist, in the 1920s. He began to advocate treatment to apparently uninvolved adjacent lymph nodes. • Peters- 1930, Princess Margaret Hospital, limited HL could be cured with aggressive radiation therapy
- 28. • For each risk group, typical standard treatment approaches are being defined: • Early favorable stages: classical HL,IA-IIA ABVD X4CYCLE or standford v 2cycle with IFRT • NLP HL ,IA-IIA IFRT alone IB-IIB Full course chemotherapy • Early unfavorable stages: moderate amount of chemotherapy (typically four cycles) plus IF-RT • Advanced stages: Bulky disease stage I-II (typically 6 cycle ABVD ) OR Standford v for 3 cycle with RT to bulky site. STAGE III-IV OR WITH B SYMPTOMS;- ABVD X 6-8cycle (or standford v or BEACOPP)
- 29. Favourable Prognosis Stage I to II A Classic Hodgkin Lymphoma • Historically, patients with favourable presentations of stage I to II Hodgkin lymphoma were candidates for treatment with radiation therapy alone, with curative intent and expectations. • The treatment volume generally included the mantle and para-aortic fields, as well as the spleen. • Results in single-institution and cooperative group trials included 10-year survival rates of 90% and freedom from relapse rates of 80%. • These results are excellent, but the appearance of late risks of radiation therapy, including secondary neoplasia and cardiovascular disease, resulted in a shift of management to the use of combined-modality therapy
- 30. • The current treatment of choice for these patients is abbreviated chemotherapy plus limited (IF) irradiation. • The results of the HD-10 trial of the GHSG suggest that patients with very favourable presentations may be treated with just two cycles of ABVD, followed by 20-Gy IFRT (8-year survival [OS], 95.1%; freedom from treatment failure [FFTF], 85.9%; progression-free survival [PFS], 86.5%). • Bonadonna et al.80: ABVD times four followed by IFRT (12-year OS, 94%; freedom from progression [FFP], 94%), although the radiation dose may be reduced to 30 Gy. • The NCCN and the European Society for Medical Oncology (ESMO),the most commonly employed treatment for favorable presentations of stage I to IIA Hodgkin lymphoma is combined-modality therapy with chemotherapy plus IFRT. The expected FFP is 90% to95%. Selected patients may be treated with chemotherapy alone.
- 32. Stage IB or IIB Hodgkin Lymphoma • Approximately 15% to 20% of patients with stage I or II disease have B symptoms. • These patients are managed in a fashion analogous to those with stage III to IV disease. • However, given the limited anatomic extent of disease in stage I to II, one can make a strong argument to include consolidative involved-field irradiation for these patients, as is recommended by the ESMO and NCCN.
- 33. Stage III to IV Disease • The use of combined-modality therapy in stage III to IV disease has a rationale. • Randomized clinical trial conducted by the Cancer and Leukemia Group B. Patients with stage IIIA, IIIB, or IV Hodgkin lymphoma were randomly assigned to treatment with MOPP (six to eight cycles), MOPP/ABVD (12 months), or ABVD (six to eight cycles). The results of treatment with MOPP/ABVD and ABVD were equivalent, and both were superior to MOPP alone. Among the 115 patients treated with ABVD chemotherapy, the complete response rate was 82%, the 5-year FFS was 61%, and OS was 73%. • Italian multi-institutionaL STUDY that compared an initial treatment strategy of ABVD (four to eight cycles) with BEACOPP (four escalated plus four baseline), which took into account the possibility of autologous stem cell transplant as salvage therapy, there was no significant difference in 7- year freedom from second progression or OS (89% vs. 84%), and severe adverse events were more likely in the BEACOPP group.
- 34. • The EORTC–Groupe Pierre-et-Marie Curie H34 (20884) trial.122 In this trial, patients were treated with six to eight cycles of nitrogen mustard, vincristine, procarbazine, prednisone, Adriamycin, bleomycin, and vinblastine chemotherapy, and those who achieved a complete response were randomized to no further therapy versus 25-Gy IFRT. No differences in FFTF or OS were identified. A detailed evaluation of causes of death revealed an unusually high risk for secondary myelodysplasia in the group of patients randomized to combined-modality therapy. • The ECOG E2496 trial compared management with ABVD versus Stanford V for patients with advanced-stage or locally advanced disease. There was no difference in 5-year FFS (73% for ABVD, 71% for Stanford V) or OS (88% for ABVD, 87% for Stanford V).
- 35. • A general conclusion regarding the role of combined-modality therapy compared with chemotherapy alone for patients with stage III to IV disease is that patients who achieve a complete response to a full course of conventional chemotherapy have no proven benefit from the addition of chemotherapy. • irradiation is often added to such programs on a selected basis, especially for bulky disease.
- 36. Role of RT in advanced stage • Retrospective analysis of data from the UK suggested that this strategy improved PFS and OS. • EORTC trial randomly assigned patients in complete remission after MOPP–ABV to IFRT or no RT, and showed no significant differences in FFS or OS between the two groups. • However, patients with partial remission after chemotherapy benefited from consolidation RT, leading the investigators to recommend consolidation IFRT only to such patients.
- 38. Stage I to II A Nodular Lymphocyte-Predominant Hodgkin Lymphoma • Patients with limited presentations of nLPHD may achieve long-term disease-free survival after treatment with involved- field or slightly extended field irradiation alone. • The usual dose is 30 to36 Gy • The retrospective review of experience with nLPHD in the GHSG, there was no significant difference in response induction, freedom from treatment failure, or overall survival for involved-field irradiation versus extended-field irradiation versus combined-modality therapy • From single-institution studies, the EORTC and GHSG adopted involved field irradiation alone, dose ∼30 Gy, as the standard treatment for these patients, which also conforms with the guidelines of the ESMO and NCCN.
- 41. Radiation Therapy Techniques • The principal objective of RT in HL is to treat involved and contiguous lymphatic chains to a dose associated with a high likelihood of tumour eradication. • RT is the most effective single therapeutic agent for treating HL. • Optimal irradiation technique includes pretreatment simulation and requires the use of MV photon beams, fields individually contoured to the patient's anatomy and tumor configuration, an adequate dose, multifield fractionated treatment, and portal film verification during therapy. • Careful attention must be paid to every detail of therapy in order to maximize outcome and minimize risks
- 42. • For many years wide field RT alone was treatment of choice for early favorable HL. • CR were high but OS was not satisfying. • CMT were superior to RT alone. • Presently RT alone: stage 1, IIA NLPHL without risk factors women younger than 40 years of age with clinical stage IA NS or NLPHL and ESR less than 50 mm/h. • GHSG & EORTC in this group of patients revealed no substantial outcome differences b/w 30Gy IFRT & 30Gy EFRT or CMT. • The range of dose considered acceptable according to NCCN guideline is • 20-30 Gy in non bulky. • 30-36 Gy in bulky sites of disease.
- 43. The Mantle • All of the major lymph node regions above the diaphragm • Position Supine, head fully extended • Arms : Akimbo, Above head • UB:bisected the mandible and passed through the mastoid process. • lateral margins: to flash the axillae • The inferior axillary margins: at the level of the inferior tips of the scapulae. • • LB: T10-11 interspace
- 44. Shielding • Lung blocks designed to provide ~1 cm margin around the mediastinal contours and also encompass the pulmonary hilar lymph nodes. • The superior most point of the lung blocks not higher than the inferior tip of the head of the clavicle. • Tops of the lung blocks tapered laterally, often parallel to the projection of a posterior rib, in order to expose the high axillary/infraclavicular LNs. • Occipital region and spinal cord- posteriorly • Larynx – anteriorly at 20Gy • Humeral head – Ant & Post • Spinal cord shielding if calculated cord dose>40Gy • If no med. LAP entire cardiac silhoutte 15Gy, place a block at ventricular apex • After 30-35 Gy subcarinal (5 cm below carina) block to shield additional pericardium and myocardium
- 45. SUBDIAPHRAGMATIC HL • Classic subdiaphragmatic irradiation field for HL- inverted-Y. which include RP,PELVIC lymph node and spleen. Field : Inverted-T /Y • Target volume: PA, iliac, both groin & femoral LN • AP/PA opposed fields Borders: UB- LB of T10 Inferiorly, the pelvis field should extend to at least the lesser trochanters or 3cm below ischial tuberosity. Lateral margin:- are set 1.5-2 cm lt to widest point of bony pelvis Dose- 30Gy/20#/4wks • Scrotum shielded • Kidney shielding done after 12# • Para-aortic boost- 7.5Gy/5#/1wk
- 46. • Ovaries - medial or lateral transposition via laparoscopy • Ovaries marked with radiopaque sutures or clips and relocated medially and as low as possible behind the uterine body. • Shielding- A double-thickness (10HVL) midline block • When the ovaries are at least 2 cm from the edge of this block, the dose is decreased to 8% of that delivered to the iliac nodes • Lateral transposition - Iliac wings. • Testes - No shield then dose 10% of delivered dose • Testicular shield can reduce this dose to 0.75% to 3.0%
- 47. At present • The full mantle is rarely treated. • Fields includes just the mediastinum and supraclavicular areas. • Cervical fields need not extend all the way to the mandible, unless there are involved high cervical nodes. • The axillae are generally not treated unless they are involved. Two dimensional design field- • UB: at the top or bottom of the larynx (depending on the extent of supraclavicular disease), • lateral borders: set at the coracoid processes of the scapulae (to include approximately two-thirds the length of the clavicle), and 1-cm margins beneath the clavicles. 3DTP commonly employed. • GTV : the involved lymph nodes • CTV: involved lymph node regions and adjacent regions considered at risk (extended CTV) are outlined on cross-sectional images . • The CTV will generally extend 2-5 cm proximal and distal to intial PET orCT positive disease. The PTV expansion is then ~1cm. • Blocking with MLCs is employed, with isodose plan review to ensure a dose range of 95% to 105% to the PTV.
- 49. 1.MANTLE FIELD 2.MINI MANTLE 3.MODIFIED MANTLE
- 50. Total nodal radiotherapy Extended field radiotherapy Involved field radiotherapy Involved site radiotherapy
- 51. IFRT – nodal site + 3-5 cm margin
- 52. PARA AORTIC FIELD • Paraaortic field covers the paraaortic, celiac, splenic and hepatic portal lymph nodes as well as splenic pedicle or spleen. • Upper border- matched with mantle. • Inferior border –at the L4-L5 interspace. • Lateral border- edges of transverse process or about 1.5-2cm lat to border of vertebral bodies(width of 8-10cm).
- 53. PELVIC FIELD • SUPERIOR BORDER- matched with paraaortic field(upper border of L5) • INFERIOR BORDER- lower border of ischial tuberosity. • LATERALLY- field shaped with blocks to spare iliac wing bone marrow without compromising coverage of iliac lymph nodal chain. • Central block-4cm block extending from the inferior edge of field and superiorly to sacroiliac joint to protect bladder and rectum.
- 54. Proton Beam Therapy • There is also significant potential advantage of protons over photons (either 3D conformal radiation therapy [3DCRT] or IMRT) in the management of Hodgkin lymphoma. • The use of proton beam therapy can be associated with decreased dose to the gut, bone marrow, and other organs but is especially advantageous with respect to mediastinal treatment. • With proton therapy, there can be maximal sparing of the esophagus, lungs, and cardiac subunits, thereby minimizing risk to those organs, • while at the same time avoiding low-dose exposure to the breasts and lungs, minimizing potential risks and complications of therapy related to those organs.
- 55. CHEMOTHERAPY
- 56. CHEMOTHERAPY • The initial successful drug combination for treating Hodgkin lymphoma was nitrogen mustard, vincristine, procarbazine, and prednisone (MOPP), reported by DeVita et al.69 from the National Cancer Institute in 1970. The acute toxicities of treatment at that time were significant. • The most successful of these is ABVD, which includes doxorubicin, bleomycin, vinblastine, and dacarbazine. ABVD has replaced MOPP as the gold standard of chemotherapy for Hodgkin lymphoma. This is based largely on the results of an intergroup trial that compared MOPP, ABVD, and MOPP/ABVD • More recently, in an effort to reduce toxicity, the Stanford V regimen which almost always includes a component of radiation, was developed as an alternative to ABVD. • As another approach, in an effort to enhance efficacy, the German Hodgkin Study Group (GHSG) developed the BEACOPP regimen, which may be administered in a baseline, escalated, or 14-day scheduling.
- 57. Combined-Modality Therapy • Combined-modality therapy has become the most common form of general management for patients with Hodgkin lymphoma. • Important considerations include the sequence of therapy, the selection of irradiation fields, the decision to irradiate all involved sites, only initially “bulky” sites, or only sites that have not responded completely to chemotherapy, the prescription of dose, and potential overlapping toxicities. • Treatment is almost always initiated with chemotherapy. • This has the advantages of treating all sites of disease at the outset (especially important in stage III or IV) and reducing bulky disease to facilitate subsequent irradiation (especially in the mediastinum). • The irradiation dose used in combined-modality studies in adults ranges from 20 to 36 Gy.
- 58. RT alone Versus CMT in Favourable Early HL Trial Treatments Outcome OS EORTC H7 10-y EFS* 10-y OS STNI (36-40 GY) 6 EBVP+IF RT (36-40 GY) 78 92 92 92 SWOG# 9133 3-y EFS* 3-y OS STNI (36-40 GY) 3CT† STNI 81 94 96 98 GHSG HD7‡ 7-y FFTF* 7-y OS EF RT 30 GY (IF 40GY) 2 ABVD EF RT 30 GY (IF 40 GY) 67% 88% 95% 94% EORTC/GELA H8 4-y EFS* 4-y OS STNI 36 GY (IF 40 GY) 3MOPP/ABV IF RT (36 GY) 77% 99% 95% 99%
- 59. Chemotherapy alone ECOG/NCI 4y-FFP OS 1A, IIA 4ABVD – STNI 93% 94% 6ABVD-noRT 87% 96% MSKCC 5yr 5yr 1A,1B, IIA, IIB 6ABVD-RT 86% 97% 6ABVD-noRT 81% 91% • Chemotherapy is better
- 60. Combined-Modality Treatment Trial Treatments Outcome OS MILAN Group* 12-y EFS 12-y OS 4ABVD STNI 30 GY (IF 36-40) 87% 96% 4ABVD IF RT (36-40 GY) 91% 94% GHSG HD 10 8-y EFS: 87% 8-y OS :94.5% 2ABVD IF RT 30 GY 2ABVD IF RT 20 GY less toxic 4ABVD IF RT 30 GY 4ABVD IF RT 20 GY EORTC-GELA H9F 4-y EFS† 4-y OS 6EBVP IF RT 36 GY 87% 98% 6EBVP IF RT 20 GY 84% 98% 6EBVP 70% 98% • *Early favorable and unfavorable groups. • 2cycles ABVD & IFRT 20-30Gy better than 4-6cycles CCT & EFRT or >30Gy IFRT
- 61. CMT in Unfavorable Early Stages HL Trial Treatments Outcome OS EORTC-GELA H8-U 10-y EFS* 10-y OS 6MOPP/ABV IF RT (36- 40 GY) 4MOPP/ABV IF RT (36- 40 GY) 4MOPP/ABV STNI (36-40 GY) 84% 88% 87% 88% 85% 84% GHGS HD 8 5-y FFTF 5-y OS 2COPP/ABVD EF RT 30 GY (bulk 40 GY) 2COPP/ABVD IF RT 30 GY (bulk 40 GY) 86% 84% 91% 92% EORTC H7U 10-y EFS* 10-y OS* 6EBVP IF RT (36 GY) 6MOPP/ABV IF RT (36 GY) 68% 88% 79% 87% EORTC-GELA H9U 4-y EFS 4-y OS 4ABVD IF RT 30 GY 6ABVD IF RT 30 GY 4 BEACOPP IF RT 30 GY 89% 94% 91% 95% 96% 93% (toxicity)
- 62. Trial Treatments Outcome OS GHSG HD-11 5-y FFTF 86% 5-y OS 94.5% 4ABVD IF RT 30 GY 4ABVD IF RT 20 GY 4BEACOPP IF RT 30 GY 4BEACOPP IF RT 20 GY Standard Inferior More toxic HD14 4ABVD IF RT 30 GY 2BEACOPPesc+2AB VD IF RT 30 GY 89.3% 94.7%
- 63. Toxicity Radiotherapy- depend on the field treated Acute- Vomiting, diarrhea, BM suppression, Herpes zoster(10-15%) Chronic: peptic ulcer, hemorrhage, diarrhea, intestinal obstruction Infertility Endocrine dysfunctions Hyposplenism Dental caries
- 64. Second malignancy: lymphoma: DLBCL (RR 5.5 to 14.0) 5 years solid tumors (RR 2.3 to 2.9) 7 to 10 years Lung, stomach, colon, pancreas, Breast, cervix, ovary, vulva, prostate, testis, kidney, bladder & NHL • 18.5 times greater than the general population. • 30 year cumulative risk of 18% for male patients and 26% for female patients • UK study: risk of breast cancer was estimated to be 29% (95% CI 20.2–40.1%) in patients who received 40 Gy mediastinal irradiation before age 25 years. • Screening with yearly mammography or MRI from 8 years after treatment or at age 25 years (whichever is later). • US guidelines recommend yearly screening from 10 years after treatment or at 40 years of age (whichever is earlier).
- 65. Chemotherapy • Emesis • Anorexia • BM suppression – more with intense regimens • Infertility MOPP- 86-100% BEACOPP-87-93% females:- 50% ABVD- <5% <5% • Neuropathy • Cardiomyopathy- adriamycin: >450mg/m2 • Pulmonary- bleomycin : >200mg/m2 • Second malignancy –alkylating agents- leukemia : AML: 1.4-11.5% (10yr), MDS, NHL, lung cancer • Negligible with ABVD • BEACOPP: AML, myelodysplasia • Psychosocial problems, fatigue, marital difficulties, and employment
- 66. Efficacy & toxicity of single agent in HL Drug Response CR(%) Toxicity Chlorambucil 60% 16 Myelosuppression, teratogenesis Cyclophosphamide 54 12 Myelosuppression, hemorrhagic cystitis, N, sterility Nitrogen mustard 63 13 N, V, Myelosuppression, thrombophlebitis, alopecia Predenisolone 61 0 Cushing’s syndrome, peptic ulceration, psychiatric disturbance, DM Procarbazine 69 38 N, myelotoxicity, neuropsychiatric disturbance, teratogenesis, Vinblastine 68 30 Myelotoxicity, neurotoxicity(infrequen t) Vincristine 64 36 Neurotoxicity
- 67. Drug Dose (mg/m2) Route Schedule (days) Cycle Length (days) MOPP 21 Mechlorethamin e 6 IV 1, 8 Oncovin (vincristine) 1.4 IV 1, 8 Procarbazine 100 PO 1-14 CR-74% Prednisone 40 PO 1-14 COPP 28 Cyclophosphamid e 650 IV 1, 8 Oncovin (vincristine) 1.4 IV 1, 8 CR-72% Procarbazine 100 PO 1-14 Prednisone 40 PO 1-14
- 68. ABVD 21 Adriamycin (doxorubicin) 25 IV 1, 15 Bleomycin 10 IV 1, 15 CR-73% Vinblastine 6 IV 1, 15 Dacarbazine 375 IV 1, 15
- 69. MOPP/ABV Hybrid 28 Mechlorethamine6 IV 1 CR- 81% Oncovin (vincristine) 1.4a IV 1 Procarbazine 100 PO 1-7 Prednisone 40 PO 1-14 Adriamycin (doxorubicin) 35 IV 8 Bleomycin 10 IV 8 Vinblastine 6 IV 8 BEACOPP (baseline) 21 Bleomycin 10 IV 8 Etoposide 100 IV 1-3 Adriamycin (doxorubicin) 25 IV 1 Cyclophosphami de 650 IV 1 Oncovin (vincristine) 1.4a IV 8 Procarbazine 100 PO 1-7 Prednisone 40 PO 1-14
- 70. Stanford V 12WK Mechlorethamin e 6 IV Wk 1, 5, 9 Adriamycin (doxorubicin) 25 IV Wk 1, 3, 5, 7, 9, 11 Vinblastine 6 IV Wk 1, 3, 5, 7, 9, 11 Vincristine 1.4a IV Wk 2, 4, 6, 8, 10, 12 Bleomycin 5 IV Wk 2, 4, 6, 8, 10, 12 Etoposide 60 IV Wk 3, 7, 11 Prednisone 40 IV Wk 1-10 q.o.d. G-CSF PO Dose reduction or delay
- 71. Increased-dose BEACOPP Cyclophosphami de 1250 IV 1 Adriamycin 35 IV 1 Etoposide 200 IV 1-3 Procarbazine 100 PO 1-7 Prednisone 40 PO 1-14 Oncovin (vincristine) 1.4a IV 8 Bleomycin 10 IV 8 G-CSF SC From d 8
- 72. Special situations • Elderly patients poorer survival than do younger patients • comorbidities, • toxic effects of treatment, • reduced treatment intensity • <70year: ABVD • Drug combinations that seem to be more tolerable for older adults include , procarbazine, Alkeran, and vinblastine, and vinblastine, bleomycin, and methotrexate (used primarily for stage I to II). • With respect to the radiation therapy, patients may need to be treated with slower fractionation programs and observed carefully for signs of weight loss or general decline in performance status. • New drugs may have role
- 73. PEDIATRIC PATIENTS • Most contemporary programs for the management of pediatric Hodgkin lymphoma are based on clinical staging and use chemotherapy alone or combined-modality therapy with lowdose irradiation because higher doses of irradiation are associated with unacceptable risks for growth impairment and late effects. • To limit growth effects, irradiation doses should not exceed 15 to 25 Gy. • Children treated with these programs, all stages combined, are reported to achieve 5-year OS rates of approximately 90% and relapse-free rates of at least 80%.
- 74. Pregnancy • HL one of the most common cancers reported in pregnancy. • To avoid radiation exposure, staging should be with ultrasonography or whole-body MRI • Radiotherapy should generally be avoided because of the risk of teratogenicity. • On the basis of data from small case series, treatment with ABVD seems to be safe, especially in the second and third trimesters. • Other treatment options include observation or symptom control with steroids or vinblastine alone until delivery. • However, the potential increased risk of relapse or refractory disease with this approach should be considered.
- 75. HIV/AIDS • In the era of highly active antiretroviral therapy, the management and disease-specific prognosis of patients with coexisting HIV/AIDS and HL are the same as for patients with HL without HIV/AIDS.
- 76. Relapsed or refractory disease and salvage chemotherapy • 10% of patients with early-stage disease • 20–30% with advanced disease will be refractory to, or relapse after, initial treatment. Outlook of patients with relapsed disease depends on • time to relapse(TTR) • stage at time of relapse • performance status. TTR 5yr OS(%) <3mo 26 3-12mo 46 >1yr 71
- 77. STAGE I AND II In general, patients who were treated initially with irradiation alone for stage I to II disease should receive chemotherapy as the primary salvage treatment. The efficacy of combination chemotherapy in this setting is similar to that achieved when chemotherapy is used in the primary management of advanced disease (rate of long-term freedom from relapse of 60% or better). The role of irradiation in combination with salvage chemotherapy has not been defined but is quite reasonable to consider if relapse is in a previously unirradiated site. More problematic is the management approach to patients who present initially with stage I to II disease and are treated with chemotherapy alone, In these patients, relapse may be restricted to initial sites of disease and be quite limited. It is possible that in this situation programs using irradiation alone, or at least emphasizing the use of radiation, may be safe and effective, especially given the success in treating some patients with initially advanced disease and limited relapse using this approach.
- 78. STAGE III AND IV • For patients who present initially with stage III to IV disease and relapse after achieving a complete response to chemotherapy or combined- modality therapy, the standard salvage therapy is high-dose chemotherapy with autologous hematopoietic cell rescue. • The long-term PFS rate for these patients is expected to be approximately 50%. • Favourable prognostic factors in this group include a longer duration of response to primary therapy and absence of extranodal disease.
- 79. Salvage CT should ideally introduce drugs that were: • not used in the original treatment, • should be reasonably non-toxic, and • should not impair subsequent harvest of haemopoietic stem cells Most widely used are: • ESHAP (etoposide, methylprednisolone, cytarabine, and cisplatin), • DHAP (dexamethasone, cytarabine, and cisplatin), • IVE(ifospha mide, etoposide, and epirubicin), and • ICE(ifosphamide, carboplatin, and etoposide) • Everolimus (only for CHL) • GCD (gemcitabine, carboplatin, dexamethasone) • GVD (gemcitabine, vinorelbine, liposomal doxorubicin) • patients not responding to first-line salvage CT, an alternative salvage regimen : mini-BEAM (carmustine, etoposide, cytarabine, and melphalan) can be effective as a bridge to transplantation in many patients.
- 80. Stem Cell Transplantation • The use of autologous bone marrow or peripheral blood stem cells (PBSC) to support intensification of chemotherapy as salvage treatment has changed the options available for relapsed patients . • Autologous transplantation involves the replacement of hematopoietic stem cells that have been irreversibly injured by HDCT or radiotherapy. • This can be accomplished, either with bone marrow cells obtained by multiple aspirations from the posterior iliac crest under anesthesia or with PBS collected by apheresis. • The use of PBSC has surpassed the use of bone marrow, and PBSC are now almost exclusively used. • The advantage of using PBSC includes avoiding general anesthesia and more rapid hematopoietic reconstitution.
- 81. Newer drugs- For relapse after or are unsuitable for allogeneic haemopoietic SCT: • Gemcitabine: median duration- 6mo • Rituximab in CD-20+ • BRENTUXIMAB VEDOTIN, is an anti-CD30 monoclonal antibody linked to an antitubulin agent. BV has demonstrated efficacy in CD30+ lymphomas, including Hodgkin lymphoma and anaplastic large-cell lymphoma. It is approved for patients who have had disease recurrence after stem cell transplantationan Phase 1: ORR – 86%, CR – 25% in 3 lines of previous CT Phase 2: ORR – 75%, CR – 34% in 4 lines of previous CT Other active drugs: • immuno -modulatory agent- lenalidomide, • the mammalian target of rapamycin inhibitor- everolimus • pandeacetylase inhibitor- panobinostat. • Bortezomib (a proteasome inhibitor) has poor activity when used alone, but could have a role in combination with other drugs.
- 82. Conclusion • Today most patients with Hodgkin’s lymphoma are cured and current developments are likely to lead to further, if small, improvements in overall survival because of both improved tumour eradication and reduction of late effects. • Because of the success of the treatment of Hodgkin’s lymphoma, proof of further advances will require very large trials with long-term follow-up, and international collaboration will be essential.
- 83. THANK YOU