Shoulder arthroscopy
•Als PPTX, PDF herunterladen•
8 gefällt mir•4,164 views

1. Shoulder arthroscopy is a surgical technique where a tube-like instrument is inserted into the shoulder joint to inspect, diagnose, and treat conditions. 2. Common indications for shoulder arthroscopy include diagnostic evaluation, repair of labral tears, rotator cuff repairs, loose body removal, and subacromial decompression. 3. Standard portals include the posterior, anterior, and lateral portals. Additional portals such as the 5 o'clock and 7 o'clock portals are used for specific procedures while avoiding neurovascular structures.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Shoulder arthroscopy
Ähnlich wie Shoulder arthroscopy (20)
Mehr von Dr Madhavan Paramanantham
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Shoulder arthroscopy
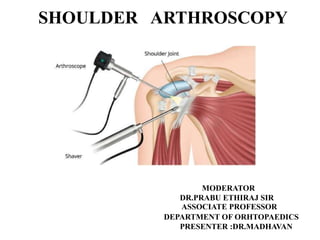
- 1. SHOULDER ARTHROSCOPY MODERATOR DR.PRABU ETHIRAJ SIR ASSOCIATE PROFESSOR DEPARTMENT OF ORHTOPAEDICS PRESENTER :DR.MADHAVAN
- 2. INTRODUCTION • Arthroscopy: A surgical technique in which a tube- like instrument is inserted into a joint to inspect, diagnose, and treat . • It is most commonly performed in patients with diseases of the knees, shoulders ,elbow ,wrist and ankle . Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 3. • The first ever use of arthroscopy was performed in 1918 orthopedic surgery by Dr Kenji Takagi(1888-1963) a Japanese orthopedic surgeon by using Charrier number 22 cystoscope in cadaver knee joint HISTORY
- 4. • In 1931 American surgeon Michael Burman examined 25 shoulders in cadaver using arthroscope • Initially it was used for diagnostic purpose • Now with well established training and skills labs , shoulder Arthroscopy is used for treatment as well!
- 5. • Painful syndromes in the shoulder , altered function, and signs and symptoms of instability and associated with internal derangement are frequent in the shoulder Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 6. • For conditions which can not be controlled by conservative managements such as • Developmental • Traumatic • Degenerative • Inflammatory conditions Resulting pain instability disability arthroscopic treatment is performed by a skilled surgeon to tackle such conditions
- 7. INDICATIONS 1. Diagnostic 2.Labral/SLAP repair 3.Rotator cuff repair or debridement
- 8. 4.Loose body removal 5.Subacromial decompression 6.AC joint pathology
- 9. 7.Distal clavicle resection 8.Release of suprascapular nerve entrapment 9.Release of scar tissue /contractures
- 11. BASIC ARTHROSCOPIC KIT • Arthroscopy • Light source and cable • Camera system and monitor with recorder • Arthroscopic probe • Arthroscopic grasper • Arthroscopic scissor • Arthroscopy cautery • Arthroscopic Punches (basket forcepes 2.7 mm upcutting right and left Rotatory ) • Motorized shaver
- 14. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 18. Wissinger rod
- 23. Esch JC, Baker CL Jr. Arthroscopic surgery: the shoulder and elbow. Philadelphia, PA: JB Lippincott, 1993:38 The angle of inclination is 0°, 30°, or 70° relative to the arthroscope axis. The angular field-of-view cone is oriented along the axis of the angle of inclination
- 24. Rotating the arthroscope’s field of view enhances arthroscopic viewing by creating overlapping circular images with a 30° arthroscope (center). With a 0° arthroscope (top), the field of view is unchanged with rotation. With a 70° arthroscope (bottom), rotation occurs around a central blind spot. (Illustration by Susan Brust.)
- 25. PATIENT POSITION Two basic positions Lateral Decubitus “Beach chair” (Most commonly used) Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 27. LATERAL DECUBITUS POSITION • The patient is placed in the lateral decubitus position with the affected shoulder exposed and is supported by a vacuum beanbag and kidney rest. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 29. All pressure points Padded with a pillow Acromion, ASIS, Below knee, lateral malleolus and one or more pillows between the knees and ankles. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 30. By tilting the patient 20 to 30 degrees posteriorly, glenoid will be parallel to the floor 1. Less traction: Decrease the risk of neurapraxia of the brachial plexus 2. Accentuation of tears in the glenoid labrum as it pulled away from their beds 3. Improved arthroscopic access to the inferior third of the glenoid labrum and capsule. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 31. Vertical and longitudinal traction, with most of the traction applied vertically to distract the glenohumeral joint without subluxing it inferiorly • 10 to 13 lb of traction is applied • 30 to 60 degrees of abduction • 20 to 30 degrees of forward flexion • 23% and 30%: neurapraxia after excessive arm traction. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 33. BEACH CHAIR POSITION The benefits of the “beach chair” position 1. Interscalene block 2. Faster and easier positioning 3. Reduced risk of neurapraxia 4. Less distortion of intra articular capsular anatomy, 5. Improved mobility of the patient’s arm 6. Ease in orientation 7. Surgical manipulation in the subacromial space 8. Ease in conversion to an open surgical procedure.
- 34. COMPLICATIONS 1. Difficulty in working from posterior portals 2. Stroke 3. Death due to hypotensive episodes Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 40. CONTRAINDICATIONS 1. Local skin conditions 2. Remote infections that might spread to the joint 3. Associated co-morbidity Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 41. CONTROL OF BLEEDING DURING ARTHROSCOPY • One method of controlling bleeding is to add 1 mL of 1 : 1000 epinephrine to each 3L bag of irrigant • A systolic-to-pump pressure gradient of approximately 30 mm Hg should be maintained • Elevation of the fluid bags 3 feet above the level produces a similar pressure gradient of 66 mm fluid flow pressure Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 42. • It has been recommended that this pressure be maintained at 49mmHg or less below the systolic blood pressure to preserve the clarity of view • An isotonic solution, such as saline (0.9%, 300mOsm/L) or lactated ringer's (273 mOsm/L), is commonly used and safely proven for joint irrigation during arthroscopy
- 43. FLUID EXTRAVASATION • Established portals should be maintained by an interchangeable cannula system while instruments are being exchanged • Lo and Burkhart evaluated 53 patients immediately after shoulder arthroscopy and found an average fluid weight gain of 8.7 lb. Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 44. PORTAL PLACEMENT Before making arthroscopic portals, a thorough understanding the local anatomy is necessary to prevent damage to neurovascular structures
- 45. AXILLARY NERVE 1. Passes ~ 7 cm below tip of acromoium 2. At risk if the posterior portal is made too inferior SUPRASCAPULAR NERVE At risk if the posterior portal is made too medial NEUROVASCULAR ANATOMY
- 46. • The axillary nerve • Cephalic vein • Suprascapular artery and nerve Are the structures most at risk during shoulder arthroscopy Meyer M, Graveleau N, Hardy P, Landreau P: Anatomic risks of shoulder arthroscopy portals: Anatomic cadaveric study of 12 portals. Arthroscopy 2007; 23(5):529-536
- 47. • The axillary nerve travels posterior to the coracoid and inferior to the lateral border of the subscapularis medial to the musculotendinous junction • The nerve has been reported to be from 3 to 7 cm from the lateral acromion
- 49. • The suprascapular nerve (SSN) arises from the upper trunk of the brachial plexus, traveling through the posterior triangle of the neck • The suprascapular artery runs with the nerve until it reaches the suprascapular notch • The nerve lies 3 cm (range, 2.5 to 3.9 cm) medial to the supraglenoid tubercle at the suprascapular notch
- 51. Standard Portal Placement Posterior portal Indication : Primary viewing portal used for diagnostic arthroscopy Location and technique 1.Posterior soft point 1.5 cm inferior and 2 cm medial to the posterolateral corner of the acromion towords coracoid 2.Pass between infraspinatus (suprascapular nerve) and teres minor (axillary nerve) 3.First portal placed 4.Direct anteriorly towards tip of coracoid
- 53. Anterior central portal(Matthews) Indication :To View and do subacromial decompression Location & technique 1. Lateral to coracoid process and anterior to AC joint 2. Portal passes between pectoralis major (medial and lateral pectoral nerves) and deltoid (axillary nerve) This portal is usually placed under direct supervision from the posterior portal with aid of spinal needle
- 54. coracoid process
- 55. Lateral portal Indication :For subacromial decompression Location & technique 1. Located 1-2 cm distal to lateral edge of acromium 2. Portal passes through deltoid (axillary nerve) Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 56. 2CMS DISTAL TO TIP OF ACROMION
- 57. ADDITIONAL PORTALS Portal Location indication 5 o’clock portal Anteroinferior transubscapularis Bankart repair 7 o’clock portal Posteroinferior Posterior labral repair, loose body removal Neviaser portal Superior, posterior to acromioclavicular joint Suture passage during slap repair and rotator cuff repair Portal of wilmington Posterolateral, 1 cm lateral to posterolateral acromion Anchor insertion during slap repair and rotator cuff repair Paxton ES, Backus J, Keener J, Brophy RH. Shoulder arthroscopy: Basic principles of positioning, anesthesia, and portal anatomy. J Am Acad Orthop Surg 2013;21:332-342
- 58. • The 5 o’clock, 7 o’clock, and anteroinferior portals are safely created using an inside- out technique 1. Posterior portal 2. Anterior central portal 3. Antero lateral portal 4. Postero lateral portal 5. Supero lateral portal 6.Anterosuperior portal 7.7 o’clock portal 8.Axillary pouch portal 9.Neviaser portal 10.portal of Wilmington 11. Trans rotator cuff portal
- 59. (5 o'clock) portal: Davidson Indication : Anterior labral repair & Bankart lesions Inside out technique: 1. Located slightly inferior to coracoid 2. This portal is usually placed under direct supervision from the posterior portal with aid of spinal needle 3. Located lateraly an average of 13 mm from axillary A, 15 mm from axillary N, and 17 mm from cephalic V Davidson PA, Tibone JE: Anteriorinferior (5 o’clock) portal for shoulder arthroscopy. Arthroscopy 1995;11(5):519-525
- 60. • Bankart lesion is an avulsion of the anterior labrum and anterior band of the IGHL from the anterior inferior glenoid.
- 63. ANTEROINFERIOR PORTAL(WOLF) • Indication : Bankarts lesion • Technique :Inside out • The arthroscope sides off the inferior edge of corocoid tip
- 64. ANTERIOSUPERIOR(WOLF) • Indication :Biceps tenotomy ,SLAP repair Bankarts lesion • Technique :Inside out and outside in • The arthroscope sides mid distance between corocoid and acromion
- 65. ANTEROLATERAL (ELMANNS) • Indication :subacromion decompression • Technique : outside in • 2cms below the lateral edge of acromion in its elongation anterior edge
- 66. POSTEROLATERAL (ELMANNS) • Indication :Subacromion decompression • Technique : Outside in • 2cms below the lateral edge of acromion in its elongation of posterior edge
- 67. superior Nevasier (supraspinatus) portal Indication: Anterior glenoid visualization, SLAP repairs And rotator cuff repair Location & technique: Outside in 1.Located just medial to lateral acromion 2.Goes through supraspinatus muscle 3.The suprascapular nerve and artery are only 3 cm from the supraglenoid tubercle and are at risk when using the Neviaser portal Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990; 6(4):301-305.
- 68. course of the suprascapular nerve along the posterior scapula. In a cadaver study by Bigliani et al line A, the distance from the supraglenoid tubercle to the suprascapular notch, averaged 3.0 cm (range, 2.5 to 3.9 cm); line B, the distance from the supraglenoid tubercle to the base of the scapular spine, averaged 2.5 cm (range, 1.9 to 3.2 cm); and line C, the distance from the midline posterior glenoid rim to the base of the scapular spine, averaged 1.8 cm (range, 1.4 to 2.5 cm) Suprascapular notch Supraglnoid tubercule Midline posterior glenoid Base of scapular spine
- 69. NEVIASER PORTAL
- 70. SUPERIOR SUPRASCASPULAR NERVE PORTAL (LAFOSSE ) • Indication : Suprsascapular never entrapment release • Technique: 1. Outside in 2. 7cm medial to the lateral border of acromion
- 72. 7 o'clock portal Davidson Indication: Posterior labral repair and loose body removal location & technique: Outside in 1. 3 to 4cms inferior, 1cm lateral to the posterior lateral acromion edge 2. The structures at risk are the the axillary nerve, and the posterior circumflex humeral artery Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 75. Wilmington portal • Indication: SLAP lesions ,acromioclavicular joint pathology and subacromial impingement,Rotator cuff tear location & technique: Outside in 1. 1cm anterior and 1cm lateral to the posterior lateral corner of acromion Burkhead WZ Jr, Scheinberg RR, Box G: Surgical anatomy of the axillary nerve. J Shoulder Elbow Surg 1992;1(1):31-36
- 76. TRAN ROTATOR CUFF (O’BRIEN) Indication: Rotator cuff repair and subacromial decompresion Technique :outside in 1. 1 cm posterior and 2 cm lateral to the anterolateral corner of the acromion 2. To the 11-o’clock position in the glenoid labrum medial to the rotator arch
- 82. PRECAUTIONS 1. Avoid chondral injury by using blunt obturators (Do not plunge!) 2. Avoid rotator cuff tendon tears during posterior portal placement by internal rotation of the humerus 3. Minimize risk of neurovascular injury by placing the anterior portal lateral to the coracoid and humerus in adduction when creating anterior portal Canale, S T, James H. Beaty, and Willis C. Campbell. Campbell's Operative Orthopaedics. Philadelphia, PA: Elsevier/Mosby, 2013
- 83. • Awareness of the axillary nerve is important in portal placement anteriorly, posteriorly, and laterally. • Posteriorly, the suprascapular nerve and circumflex scapular artery are approximately 2 cm from the portal site. • Later portals, which are used to work on the glenohumeral space, should be directed to enter medial to the rotator arch
- 89. Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 90. 10 steps visualizing from posterior port 1.Biceps tendon and superior labrum: • Evaluate both surfaces of intra articular segments • There should be no fraying • Grasping tool to pull and to check for any damage to biceps tendon • Evaluate anterior and posterior pully Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 91. • Vinculae biceps : mesentery like synovium Should not mistaken for tear Rare cases • Biceps tendon is partically or completely encased by synovial tissue and capsule • Bifid biceps one portion attached to supragleniod and another to rotator cuff • Some times to completely to rotator cuff • Complete absence of biceps tendon with no history of trauma with normal function Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 96. VINCULAE BICEPS
- 98. BIFID BICEPS
- 100. SUPERIOR LABRUM • Inspect the superior labrum and palpate the attachment to the glenoid • If the superior labrum is damaged or loosely attached, pull on the biceps tendon with a probe to determine whether the labrum will arch away from superior glenoid Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 102. • In young patients: The edge of the labrum intimately attached • Patients mature: Labrum separates from the cartilage so that by age 40 to 50 most people have a prominent cleft under the superior labrum (MENISCOID APPEARCNCE ) Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 103. MENISCOID APPERANCE
- 104. • Acute trauma in a younger individual (15 to 30 years of age) can result in avulsion of the superior labrum and biceps anchor • The tissue below the superior labrum will be frayed, torn, and irregular • chronic degenerative conditions of the glenohumeral joint or biceps tendon will cause the superior labrum to appear damaged • suggesting a type 2 SLAP lesion
- 107. 2.The Posterior Labrum and Posterior Capsular Recess • The posterior labrum should be smooth and is usually tightly fused to the glenoid surface • The outer edge of the healthy labrum is higher than the cartilage edge, creating a chock block–like border • multidirectional instability, the labrum can be hypoplastic
- 108. HYPOPLASTIC POSTERIOR LABRUM IN MULTIDIRACTIONAL INSTABILITY
- 109. 3.The Inferior Axillary Recess, the Inferior Capsular Attachment to the Humeral Head • Scope tip positioned in the axillary pouch, the bevel is rotated in an arc from inferior to superior to see the inferior capsule • Smooth with a delicate synovial covering will be present • There may be small normal fenestrations near the attachment to the head Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 110. • Early chondromalacia lesions or osteophytes are seen in this position • In adhesive capsulitis the inferior Capsule is contracted and closing off the pouch will be present • Inferior capsular attachment tear to the humerus : seen in traumatic dislocation, especially with luxatio erecta. Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 111. Axillary recess with smooth synovial covering , articular cartilage of humerus
- 112. 4.Inferior Labrum and Glenoid Articular Surface • The normal inferior labrum is smoothly fused with the cartilage • Congenital laxity, the labrum may appear deficient or flat • Torn inferior labrum always associated with anterior instability • “Thin spot” : Inferior half of the glenoid which is Normal • superior pole of the glenoid may also become thinner with aging: Normal
- 113. The articular surface of the glenoid is slightly concaved with a thin area in the center
- 114. 5. Supraspinatus Tendon of the Rotator Cuff • Rotate the bevel of the arthroscope upward to the 11, 12, and 1 o’clock positions to visualize the undersurface of the supraspintatus tendon as it attaches into the humeral head • The rotator cuff tendon is covered by layer of capsule and synovium Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 115. • “Rotator cuff ridge” or “cable: it’s a capsule thikening perpendicular biceps tendon • A rich vascular supply above the lateral border of the rotator cuff ridge known as the rotator cuff crescent
- 116. The supraspinatus tendon attaches to the humeral head adjacent to the articular cartilage. The rotator ridge or cable is a capsular band extending from the anterior edge of the cuff to the posterior humeral head enclosing the area called the crescent.
- 117. 6.The Posterior Rotator Cuff insertion the “Bare Area” of the Humeral Head 1. The rotator cuff in this posterior area frequently appears fenestrated with openings in the superficial layers 2. The “bare area” of the humerus is a portion of the head that is devoid of articular cartilage 3. Located adjacent to the posterior lateral rotator cuff attachment 4. 2 to 3 cm in size
- 118. 1. Within this area there can be deep pits representing vascular channels in the bone 2. We should not confuse this bare area with a post- dislocation osteochondral fracture known as the Hill-Sachs lesion. 3. The Hill-Sachs lesion is found in a more medial location Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 119. The bare area of the humeral head is located adjacent to the infraspinatus attachment to the humeral head and may have multiple blood vessel channels
- 120. 7. Articular surface of humeral head 1. Rotate the bevel of the scope both clockwise and counterclockwise to visualize globe of the humeral head 2. Center of the humeral head break down in chondrolysis, osteochondritis, or degenerative arthritis 3. Blistering of the cartilage is a sign of impending chondral breakdown Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 121. The globe of the normal humeral head is smooth with firm articular cartilage.
- 122. 8. Anterior-Superior Labrum, the Superior Glenohumeral Ligament, Subscapularis Tendon, and the MGHL In 14% of normal patients, there will be an opening or sublabral foramen beneath the labral attachment Know as cleft which is normal
- 123. • Anterior-superior labral detachment is the so-called Buford complex • Variant occurs in approximately 2.5% of shoulders. There are three features included in the complex: (1) There is a thick cord- like MGHL (2) The MGHL attaches to the superior labrum just anterior at the base of the biceps anchor (3) Absence of labral tissue on the anterior-superior glenoid Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 124. The Buford complex is easily confused with anteriorsuperior Labral detachment.
- 125. • Anatomic variations region of anterosuperior labrum and MGHL has wide anatomic variability –Attached labrum with broad MGHL is most common –Sublabral hole with cordlike MGHL –Buford complex • Has absent labrum and cordlike MGHL
- 127. • The subscapularis tendon is a very prominent landmark demarcating the inferior boundary of the anterior-superior triangle. Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 128. The superior glenohumeral ligament attaches to the Lateral edge of the subscapularis tendon.
- 130. 9.Includes the Anterior-Inferior Labrum 1. Rotate the bevel inferiorly to visualize the entire anterior-inferior labral attachment to the glenoid 2. 95% of cases, the labrum has a smooth attachment to the glenoid cartilage 3. “meniscoid type” in which the articular edge of the labrum is separated from the glenoid cartilage Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 131. The anterior-inferior labrum and the attachment of the anterior- inferior ligaments are best seen when viewing from the anterior portal
- 132. 10. Anterior-Inferior Capsule and ligament 1. The anterior capsular ligaments insert into the labrum and are firmly attached with it to the neck of the glenoid. 2. The capsular tissues are smooth and covered with a thin synovial membrane Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 134. Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 135. 11. Posterior Labrum and the Capsule insertion in to the humeral head 1. To evaluate the posterior-inferior labrum 2. Firmly attached at the periphery 3. Posterior capsular recess cannot be well-visualized but capsular laxity can be assessed by pinching a fold of capsule with a pincer clamp 4. Tear in the capsule called as Reverse Humeral Avulsion Of The Glenohumeral Ligament “RHAGL” lesion Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 136. 1. Reverse Humeral Avulsion Of The Glenohumeral Ligamen “RHAGL” lesion opposite to HAGL 2. HAGL is inferior gleno humeral ligament injury
- 144. The posterior capsule can be seen attaching to the posterior aspect of the humeral head
- 145. 12. Posterior-Superior Capsule and the Posterior Aspect of the Rotator Cuff 1. The normal surface of the rotator cuff is smooth, with regular vascularity 2. The posterior attachment of the rotator cuff ridge or cable arches to attach to the humeral head Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 147. 13.The Anterior Labrum and the Attached Anterior-Inferior Ligament to the Humeral Head 1. To evaluate the anterior-inferior labrum 2. Assess the status and quality of the supporting ligaments, labrum, and capsular tissue when evaluating for instability 3.The labrum can be palpated with a probe passed through a posterior portal to assess the security of the attachment to the glenoid
- 148. The lateral humeral attachment of the anterior capsule must be evaluated by turning the scope bevel to view in a lateral direction
- 149. 14.Includes the Anterior Attachment of the MGHL and the Subscapularis Recess 1. The superior edge of the subscapularis tendon must be carefully evaluated for fraying below the level of the glenoid rim, the so-called Frayed Upper Subscapularis with Impingement (FUSSI) lesion 2. Loose bodies are present in the shoulder, they will be located in the subscapularis recess 3. The anterior attachment of the MGHL crosses the tendon to insert into the labrum or glenoid neck
- 150. The subscapularis recess may have several compartments that can hide loose bodies.
- 151. The attachment of the MGHL into the labrum or glenoid neck is seen crossing the subscapularis tendon
- 152. 15.Attachment of the Subscapularis Tendon , the Anterior Surface of the Humeral Head, and the Adjacent Biceps Tendon 1. Tip of the arthroscope follows the leading edge of the subscapularis tendon up to its attachment into the humerus at the lesser tuberosity 2. Visualize the anterior articular surface of the humeral head. 3. There is sometimes a normal “bare area” similar to that found on the posterior humeral head
- 153. • This area should not be confused with an anterior humeral head defect found in conjunction with posterior instability Snyder, S. J. (2015). Shoulder arthroscopy. Philadelphia: Wolters Kluwer Health.
- 154. The anterior surface of the humeral head is an important area to evaluate the subscapularis attachment
- 155. Summary
- 156. • Thank you