Arteries of Head and Neck
•Als PPTX, PDF herunterladen•
12 gefällt mir•2,002 views

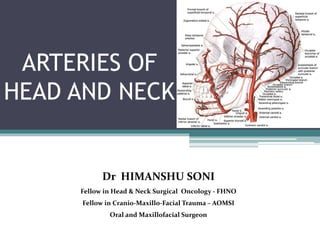
Head and Neck receives the majority of its blood supply through the carotid and vertebral arteries.
![Contents
INTRODUCTION
• Embryology and Development
• Carotid system
• Internal carotid artery
• External carotid artery
[ branches , relations, applied significance in head and
neck surgery]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Arteries of Head and Neck
Ähnlich wie Arteries of Head and Neck (20)
Mehr von Himanshu Soni
Mehr von Himanshu Soni (14)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Arteries of Head and Neck
- 1. ARTERIES OF HEAD AND NECK Dr HIMANSHU SONI Fellow in Head & Neck Surgical Oncology - FHNO Fellow in Cranio-Maxillo-Facial Trauma – AOMSI Oral and Maxillofacial Surgeon
- 2. Contents INTRODUCTION • Embryology and Development • Carotid system • Internal carotid artery • External carotid artery [ branches , relations, applied significance in head and neck surgery]
- 3. DEFINITION BLOOD VESSELS-These are cell lined tubes and spaces which surround the tissues and provide continuous perfusion of body fluids. • It consists of three layers 1 Tunica intima 2 Tunica media 3 Tunica adventitia Arteries: A vessel in which blood flows away from the heart, in the systemic circulation carrying oxygenated blood. -Dorland’s Pocket Medical Dictionary 27th Edition
- 5. THE BASIC CONDUCTING SYSTEM HEART ARTERIES ARTERIOLES CAPILLARIES/ SINUSOIDS VENULES VEIN
- 6. EMBRYOLOGY • During the fourth and fifth weeks of embryological development, when the pharyngeal arches form, the aortic sac gives rise to arteries – the aortic arches. • The aortic sac is the endothelial lined dilation, it is the primordial vascular channel from which the aortic arches arise. • In the initial stage there are pairs of aortic arches, which are numbered I, II, III, IV, and V.
- 7. Aortic arches are short vessels connecting ventral and dorsal aortae on each side they run within branchial (pharyngeal) arches are based gradually in the 4th and 5th week, in 6 pairs in total. The first, second and fifth pairs soon disappear AORTIC ARCHES
- 8. The ventral part of the aortic sac ,left horn and the left fourth arch artery, form the “Arch of Aorta”. The right horn of the aortic sac forms the brachia- cephalic or innominate artery. The right fourth arch artery forms the proximal part of the right subclavian artery. On the left side, the subclavian artery is derived entirely from the seventh cervical intersegmental artery. As the right third and fourth arch arteries arise from the right horn of the aortic sac, the common carotid and subclavian arteries becomes branches of brachia- Cephalic artery. The external carotid artery arises as a bud from the third arch artery. The pulmonary arteries are derived from the part of sixth arch arteries. DEVELOPMENT OF ARTERIES
- 9. ARCH OF AORTA Branches of Arch of Aorta 1. Left Subclavian artery. 2. Left Common Carotid artery. 3. Brachiocephalic trunk. -Right subclavian artery. -Right common carotid artery. 9
- 10. VARIATIONS IN THE BRANCHES OF THE ARCH OF AORTA COMMON ORIGIN OF BRACHIOCEPHALIC AND CCA COMMON STEM FOR THE RIGHT VESSELS LEFT VERTEBRAL FROM AORTA RIGHT SUBCLAVIAN ARISES FROM BELOW AORTIC ARCH
- 11. INTRODUCTION • The arteries of the oral apparatus and adjacent regions are, with few exceptions, branches of the external carotid artery. • Only parts of the nasal cavity and the upper parts of face are supplied by the internal carotid artery. • The external carotid artery sometimes termed as facial carotid while internal carotid artery is termed as cerebral carotid.
- 12. COMMON CAROTID ARTERY Right CCA is a branch of brachiocephalic artery & it begins in the neck behind the right sternoclavicular joint. Left CCA is a branch of the arch of aorta & it begins in the thorax in front of trachea, little left to the center of the manubrium. At the level of the upper border of thyroid cartilage the artery dividing into the external and internal carotid arteries.
- 13. Relations Of The Common Carotid Artery • Anterolaterally: skin, fascia, sternocleidomastoid muscle, sternohyoid, superior belly of omohyoid. • Posteriorly: transverse processes of the lower four cervical vertebrae, prevertebral muscles, sympathetic trunk, vertebral vessel in the lower part of the neck.
- 14. • Medially: larynx, pharynx, trachea, esophegus, thyroid gland. • Laterally: internal jugular vein, vagus nerve posterolaterally. Relations Of The Common Carotid Artery
- 16. VARIATIONS IN COMMON CAROTID ARTERY BIFURCATIONS
- 17. Carotid Sinus- • The termination of CCA or beginning of the internal carotid artery shows a slight dilatation known as carotid sinus. • Acts as a baroreceptor (pressure receptor) & regulates blood pressure. Carotid sinus hypersensitivity (CSH) is an exaggerated response to carotid sinus baroreceptor stimulation. It results in dizziness or syncope from transient diminished cerebral perfusion. For these individuals, even mild stimulation to the neck results in marked bradycardia and a drop in blood pressure
- 18. • Small, oval reddish brown structure situated behind the bifurcation of CCA. • Receive nerve supply from glossopharyngeal & vagus nerve. • Act as a chemoreceptor & responds to change in the O2 & CO2 content of blood. Carotid Body
- 19. Carotid Pulse: Common carotid can be compressed against the carotid tubercle of transverse process of C6 vertebra (carotid tubercle of CHASSAIGNAC) about 4 cm above the sternoclavicular joint. . Carotid Body Paragangliomas are vascular lesions. These lesions splay apart the internal (ICA) and external carotid arteries (ECA), and as it enlarges, it will encase, but not narrow the ICA and ECA. Head Neck Pathol. Dec 2009; 3(4): 303–306. APPLIED SIGNIFICANCE
- 20. INTERNAL CAROTID ARTERY • Origin- at the upper border of thyroid cartilage, at the disk of third and fourth cervical vertebra and ascend to reach the base of the skull where it enters the carotid canal Branches • Cervical part in the neck • Petrous part in the petrous temporal bone • Cavernous part in the cavernous sinus • Cerebral part in relation to base of brain
- 21. • It ascends vertically in the neck from its origin to the base of skull to reach the lower end of the carotid canal. This part is enclosed in carotid sheath along with internal jugular and vagus nerve. • No branches arises from the internal carotid artery in the neck. Cervical Part
- 22. Petrous Part Branches- 1) Carotico-tympanic- enter middle ear & anastomose with ant. & post. Tympanic branches 2) Artery of the Pterygoid Canal- anastomose with greater palatine artery Within the petrous part of the temporal bone, in the carotid canal runs upward forward & medially at right angle.
- 23. Cavernous Part Within the Cavernous Sinus • Branches 1) Artery to trigeminal ganglion 2) Superior & inferior Hypophyseal artery
- 24. Cerebral Part Lies at the base of the brain after emerging from the cavernous sinus Branches 1.Ophthalmic. 2.Anterior Cerebral. 3.Middle Cerebral. 4.Posterior Communicating. 5. Anterior choroidal On angiogram, this part of internal carotid artery show ‘S’ shaped figure (carotid siphon)
- 25. Central artery of retina- first branch of ophthalmic Lacrimal artery- largest branch Post & ant ciliary Supraorbital- supplies skin of forehead Ant & post. Ethmoidal- supplies ethmoidal sinus Medial palpebral- supplies eyelids Dorsal nasal- supplies the nose. a) Zygomaticofacial artery- • It is branch of lacrimal branch of the ophthalmic artery. • Enters the face through the zygomaticofacial foramen. • Supplies the area of the face over the zygomatic bone. OPHTHALMIC ARTERY
- 26. CIRCLE OF WILLIS
- 27. • It lies anterior to the internal carotid artery. • Chief artery that supply the face and front of the neck. COURSE & RELATION • It begins in the carotid triangle at the level of upper border of thyroid cartilage (C3-C4). • It runs upward & slightly backwards ,laterally & terminates behind the neck of the mandible by dividing into- - Maxillary artery - Superficial temporal artery EXTERNAL CAROTID ARTERY
- 28. • Anteromedial to the ICA in its lower part. • Anterolateral to the ICA in its upper part. In 15% ECA originates lateral to the ICA, this variation occurs more frequently on the right (3:1) a) In the carotid triangle- Superficially- Cervical branch of facial nerve Hypoglossal nerve superior thyroid veins Deep to the artery- Wall of pharynx Superior laryngeal nerve Ascending pharyngeal artery
- 29. b) Above the carotid triangle- Lies deep in the substance of the parotid triangle. Superficially—Retromandibular vein Facial nerve Deep to the artery—ICA Structures passing between ECA and ICA Styloglossus Stylopharyngeus IXth nerve Pharyngeal branch of Xth nerve Styloid process
- 30. BRANCHES
- 31. Superior Thyroid Artery First branch Arises just below the level of the greater cornu of the hyoid bone It runs downwards and forwards deep to the infrahyoid muscles to the upper pole of the thyroid gland.
- 32. Branches
- 33. Applied Anatomy • The artery and the external laryngeal nerve are close to each other higher up, but diverge near the gland. To avoid injury to the nerve, the superior thyroid artery is ligated as near to the gland as possible.. • Intra-arterial infusion chemotherapy for laryngeal and hypopharyngeal cancers. • Origin and branching pattern of STA is highly variable. A total of 25 angiograms were evaluated, including 14 right and 11 left. On the right side, STA was noted to arise from ECA in 10 (71.5%), bifurcation of CCA in 3 (21.5%), and CCA in 1 (7%) patient. Left STA was seen to arise from ECA in 8 (72.5%), bifurcation of CCA in 2 (18.5%), and internal carotid artery (ICA) in 1 (9%) patient. Type III branching pattern (non-bifurcation, non-trifurcation) was found to be the most frequent (52%).
- 34. Lingual Artery Origin : Lingual Artery arises from the ECA opposite the tip of greater cornu of the hyoid bone Course- is divided into 3 parts by the hyoglossus muscle. First part of artery lies in the carotid triangle Second part of artery- lies deep to the hyoglossus muscle which separates it from the hypoglossal nerve Third Part or deep part- runs upwards along the anterior margin of the hyoglossus
- 35. Suprahyoid Br- it runs along the hyoid’s upper border Dorsal Lingual Br- arise medial to the hyoglossus to supply tongue, palotoglossal arch, tonsil, soft palate and epiglottis. Sublingual Artery- supplies the sublingual gland, mylohyoid and the lingual and gingival mucous membrane. Deep lingual artery- Terminus of the lingual artery. Passes along the ventral aspect of the tongue, accompanied by the lingual nerve, to its apex. Branches
- 36. Applied Anatomy • During the surgical removal of the tongue, the first part of the artery is ligated before it gives of any branch to the tongue or tonsil. • Submandibular gland is palpated first and extent is noted • Incision is made from little below and external to symphysis menti curving down to point near cornu of hyoid bone then again extending upward to terminate below and in front of angle of mandible. • Skin, superficial fascia, platysma and deep fascia are separated • The submandibular gland which is exposed is separated from its deep attachments and retracted upward on to the face. • This exposes the digastric triangle, mylohyoid and anterior belly of digastric anteriorly, posterior belly of digastric posteriorly, hyoglossus muscle as floor.
- 37. Applied Anatomy • Running along the floor we get hypoglossal nerve and ranine veins which are then displaced upwards and digastric tendon downwards. • A small transverse blunt incision is made on the hyoglossus muscle (along the fibers) parallel to the ranine vein • Lingual artery comes into view once the whole thickness of the muscle is divided.
- 38. Applied Anatomy • Variation in origin of lingual artery has been documented in various articles. Lingual artery arising from common carotid Common lingual-facial trunk
- 39. FACIAL ARTERY Facial artery is the chief artery of the face Origin : Arises from the ECA just above the greater cornu of the hyoid bone It has two parts, cervical part in the neck and facial part. At the antero-inferior angle of the masseter muscle, it can be palpated here and is called as an “anesthetist's artery” Tortuous course—In neck allows free movements of pharynx during deglutition, on face -- free movements of mandible , lips, & cheek during mastication & facial expressions, escapes traction & pressure during movements
- 40. Branches of Cervical part 1. Ascending palatine artery- supplies to the levator veli palatini, superior pharyngeal constrictor and neighboring muscles, soft palate, tonsils, and auditory tube. 2. Tonsillar- supply the palatine tonsil and the posterior tongue. 3. Submental artery- Arises from the facial artery near the anterior border of the masseter muscle. it accompanies the mylohyoid nerve, and supplies the submental triangle and sub lingual salivary gland. 4. Glandular branches that supplies submandibular salivary gland and submental lymph nodes.
- 41. Branches Of Facial Part 1. Superior labial- passes superficial to the orbicularis oris muscle, supplies to upper lip & antero-inferior part of nasal septum. 2. Inferior labial- Originates near the corner of the mouth, passes deep to the depressor anguli oris muscle, and pierces the orbicularis oris muscle, supplies to lower lip. 3. Lateral nasal- to the ala & dorsum of nose. 4. Angular – supplies the lacrimal sac and orbicularis oculi.
- 42. APPLIED ANATOMY • Facial Artery Compression: Applying pressure to the facial artery as it passes over the inferior border of the mandible just anterior to the angle will diminish blood flow to that side. oCan be injured –during operative procedures on lower premolars & molars, if instrument enters the cheek at inferior vestibular fornix., also while attempt to open a buccal abscess or mucocoele.
- 43. Ligation Of Facial Artery • The facial artery can be easily exposed at the point where it crosses the lower border of the mandible to pass from the submandibular region into the face. • Contracted masseter muscle is used as a landmark Procedure • The incision is made at least half inch below the border of the mandible and parallel to it. • The skin, platysma muscle, and deep fascia are cut, and then the soft tissues are bluntly retracted upward until the palpating finger can feel the pulse of the facial artery. • The artery then can be isolated, tied and cut.
- 45. ASCENDING PHARYNGEALARTERY A small branch arises from medial side of ECA Long, slender vessel, deeply seated in the neck It runs vertically upwards between the side wall of the pharynx, the tonsil, the medial wall of the middle ear and , the auditory tube.
- 46. Branches • Pharyngeal arteries- supply the constrictors and the stylopharyngeus. It gives minute branches to the tonsil and one to auditory tube. • Inferior tympanic artery - supply the tympanic cavity’s media wall. • Meningeal branches are small vessels to the nerves, duramater and adjacent bone, entering the cranium through the foramen lacerum, jugular foramen and hypoglossal canal.
- 47. Applied anatomy • Trauma- The ascending pharyngeal artery plays an important role in the healing process of Le Fort I osteotomies, because it supplies the attached posterior palatal soft-tissue pedicle and also in closure of cleft palates. • Epistaxis- Ascending pharyngeal artery Embolization plays an increasing role in the management of epistaxis • High-Grade Head and Neck Tumors- Intra-arterial embolization i.e. Super selective microcatheter infusion of the ascending pharyngeal artery is necessary for successful embolization • Vascular Lesions- At the skull base, the ascending pharyngeal artery can be a major feeder to arteriovenous fistulas or arteriovenous malformations. . • Collaterals to Agenetic or Occluded Internal Carotid Artery- The ascending pharyngeal artery can function as collaterals to an agenetic internal carotid artery The ascending pharyngeal artery can also be recruited in case of an occluded internal carotid artery
- 48. Small and arises above the posterior belly of digastric It runs upwards and backwards deep to the parotid gland, crosses the base of the mastoid process and ascends behind the auricle. POSTERIOR AURICULAR ARTERY
- 49. Branches • Stylomastoid artery- enters the stylomastoid foramen to supply the facial nerve, tympanic cavity mastoid antrum and air cells and semi auricular canals. • Auricular branch- ascending deep to auricular posterior ramifies on the cranial aspect of the auricle; some branches pierces thin, others curve round it to supply its lateral aspect. • Occipital branch- passes laterally across the mastoid process turning back over the Sternocleidomastoid to supply the occipital belly of the occipital frontalis and scalp above and behind the ear, it anastomoses with the occipital artery.
- 50. Arises from the posterior part of the external carotid, opposite the facial artery. Ends in the posterior part of the scalp May arise from Internal carotid artery. • Relations: • Posterior belly of digastric muscle • Atlas and mastoid process • Trapezius and sternocleidomastoid muscle OCCIPITALARTERY
- 51. Branches IN THE CAROTID TRIANGLE • STERNOMASTOID BRANCHES – Two. Upper branch accompanies the accessory nerve and lower branch arises near the origin of the occipital artery. Supplies sternomastoid muscle. IN THE POSTERIOR TRIANGLE and SCALP REGION: • AURICULAR BRANCH: Passes superficial to the mastoid process to reach and supply the back of the auricle. • MASTOID BRANCH:–Enters cranial cavity through mastoid foramen, supplies mastoid air cells
- 52. Branches • MENINGEAL BRANCH – Ascends with the internal jugular vein and enters the skull through jugular foramen & condylar canal, supplies dura of posterior cranial fossa. • MUSCULAR BRANCH-Supply the Digastricus, Stylohyoideus, Splenius, and Longissimus capitis. • DESCENDING BRANCH- divides into a superficial and deep portion. -The superficial portion runs beneath the Splenius, giving off branches which pierce that muscle to supply the Trapezius -The deep portion runs down between the Semispinales capitis and colli.
- 53. APPLIED ANATOMY Ligation of occipital artery Indication- wound of the vessel (stab, gun shot etc) and cirsoid aneurysm of scalp Steps- An oblique incision 2 inches long extending from the tip of the mastoid process towards the external occipital protuberance is made. The superficial structures are separated and the sternocleidomastoid insertion is exposed. The occipital artery is found lying in the space between the mastoid process and the transverse process of atlas under posterior belly of digastric Then the needle is passed and is ligated
- 54. Larger of the two terminal branches Arises behind the neck of the mandible, and is imbedded in the substance of the parotid gland It supplies the deep structures of the face MAXILLARY ARTERY
- 56. Branches 1st part (mandibular) : Lies medial to mandible, passes between the ramus of the mandible and the sphenomandibular ligament, where it lies parallel to and a little below the auriculotemporal nerve; it crosses the inferior alveolar nerve, and runs along the lower border of the lateral pterygoid. BRANCHES Deep auricular artery Anterior tympanic artery Middle meningeal artery Accessory meningeal artery Inferior alveolar artery
- 57. Largest artery that supplies the dura It ascends between the sphenomandibular ligament and the lateral pterygoid muscle between the two roots of the auriculotemporal nerve to the foramen spinosum through which it enters the middle cranium Divides into two branches, anterior and posterior. Middle meningeal artery (medidural artery)
- 58. BRANCHES ANTERIOR BRANCH OR FRONTAL BRANCH: Crosses the great wing of the sphenoid, reaches the groove, in the sphenoidal angle of the parietal bone, and then divides into branches which spread out between the dura mater and internal surface of the cranium. POSTERIOR BRANCH OR PARIETAL BRANCH: Curves backward on the squama of the temporal bone, and divides into branches which supply the posterior part of the dura mater and cranium.
- 59. APPLIED ANATOMY • It get injured in head injuries resulting in extradural hemorrhage. • The frontal or anterior branch is commonly involved. The hematoma presses the motor area, giving rise to hemiplegia of the opposite side. • The anterior division can be approached surgically by making hole in the skull over the pterion, 4 cm above the zygomatic arch. • Rarely parietal or posterior branch is implicated, causing contra lateral deafness. In this case hole is made 4 cm above and 4 cm behind the acoustic meatus.
- 60. Inferior Alveolar Artery ( inferior dental artery): COURSE: Descends with the inferior alveolar nerve to the mandibular foramen on the medial surface of the ramus of the mandible. It runs along the mandibular canal accompanied by the nerve, and opposite the first premolar tooth divides into two branches, incisor and mental. The incisor branch is continued forward beneath the incisor teeth as far as the middle line, where it anastomoses with the artery of the opposite side; The mental branch escapes with the nerve at the mental foramen, supplies the chin, and anastomoses with the submental and inferior labial arteries.
- 61. BRANCHES BEFORE ENTERING MANDIBULAR CANAL: • Lingual branch to the tongue. • Mylohyoid branch to the mylohyoid muscle. WITHIN THE MANDIBULAR CANAL: Branches to the mandible Branches to the roots of each teeth upto midline(dental branches) Incisor branch anastomoses with the branch from opposite side. AFTER EMERGING FROM MENTAL FORAMEN: mental branch escapes with the nerve at the mental foramen, supplies the chin, and anastomoses with the submental and inferior labial arteries
- 62. 2nd part (pterygoid part) : Artery runs forward & upward superficial to the lower head of the lateral pterygoid muscle
- 63. 3rd part (pterygopalatine): Terminal portion of the artery passes between the two heads of the lateral pterygoid muscle
- 64. Infraorbital Artery ORIGIN: Arises just before maxillary artery enters the pterygomaxillary fissure. COURSE;It runs along the infraorbital groove and canal with the infraorbital nerve, and emerges on the face through the infraorbital foramen, beneath the infraorbital head of the Quadratus labii superioris.
- 65. LITTLE’S AREA or KIESSELBACH’S PLEXUS -Near the anteroinferior part or vestibule of the septum. -Contains anastomoses between • Superior labial branch of facial artery • Branch of sphenopalatine artery • Anterior ethmoidal artery • Greater palatine artery This is common site of bleeding from nose or epistaxis. Prevention – pressure pack, Silver nitrate pack if fails Surgical ligation of sphenopalatine artery or ECA or ethmoidal arteries.
- 66. APPLIED ANATOMY OF MAXILLARY ARTERY • Surgeries involving condyle- Injury to maxillary artery can occur as it lies medial to condyle. • Can be used as arterial donor in repair of ICA dissections and aneurysms, due to close proximity of the artery to the cranial base. • Control of epistaxis---If epistaxis is not controlled after nasal packing,it can be controlled by ligating IMA via endonasal , transantral or intraoral approach.
- 67. LIGATION OF MAXILLARY ARTERY Two approaches: • 1.Transantral approach • 2.Intraoral approach
- 68. TRANSANTRAL APPROACH • Transmaxillary approach by Calwell Luc method. • Most widely used for controlling posterior epistaxis. • PROCEDURE • Incision is made at canine mucobuccal fold. • Following an incision into the soft tissue over the maxillary sinus, the bony face of this sinus is exposed.
- 69. • Fenestration of the bony face of the maxillary sinus • Anterior wall of maxillary sinus is removed taken special care not to damage the infraorbital nerve.
- 70. • Posterior wall of sinus is identified and laterally based mucosal u flap is elevated. • Position of posterior wall is removed to gain access to pterygopalatine fossa and branches of maxillary artery.
- 71. • In most cases branches are visualized by operating microscope. • Descending palatine and Sphenopalatine are important for ligation.
- 72. INTRAORAL APPROACH • It provides access to the 1st and 2nd parts of the maxillary artery without opening the maxillary sinus. • It does not require any microscope to operate. • The site of ligation is more proximal than transantral approach so more chance of collateral circulation and failure.
- 73. PROCEDURE • Incision at upper gingivo buccal sulcus at the level of 2nd and 3rd molars and continued inferiorly along the ramus of mandible. • Buccal pad of fat is retracted medially or removed and attachments of temporalis muscle to the coronoid process is identified. • Blunt dissection reveals the maxillary artery which is clipped or ligated
- 74. It begins in the substance of the parotid gland, behind the neck of the mandible Divides into two branches, a frontal and a parietal COURSE: It runs vertically upwards crossing over the root of the zygomatic process -about 5 cm. above this process it divides into two branches, a frontal and a parietal. SUPERFICIAL TEMPORAL ARTERY
- 75. • Relations.—As it crosses the zygomatic process, it is covered by the Auricularis anterior muscle, and by a dense fascia. • It is crossed by the temporal and zygomatic branches of the facial nerve, and is accompanied by the auriculotemporal nerve, which lies immediately behind it.
- 76. Transverse facial branch Anterior auricular branch Frontal branch Parietal branch Zygomatic- orbital branch Middle temporal branch Branches
- 77. APPLIED ANATOMY • Control of temporal haemorrhage. • Placement of incisions in craniotomy • In reduction of zygomatic arch fractures – Gilli’s approach Temporal arteritis occur when one or more arteries become inflammed, swollen, and tender.
- 78. LIGATION • A 2cm incision is placed in the temporal region at an angle 45 degree to the zygomatic arch, between two branches of the superficial temporal artery and parallel to the anterior branch. • This exposes the artery with auriculo temporal nerve lying in front and temporal vein behind
- 79. EXTERNAL CAROTID ARTERY LIGATION Can be done in carotid triangle or in retromandibular fossa. INDICATION: Bleeding from oral malignancies Diminishment of blood supply to the area of the tumor bed Involvement of vessel or major branch in tumor Injuries causing carotid blow-outs SPECIAL INSTRUMENTS: Vascular loops and sutures Vascular clamps
- 80. LANDMARKS 1)Upper border of thyroid cartilage 2)Carotid bulb 3)Internal jugular vein 4)lower border of mandible 5)Anterior border of sternocleidomastiod muscle
- 81. CONSIDERATIONS BEFORE LIGATION- -To Obtain control of CCA below bifurcation before ligation. -Be certain that vagus nerve, IJV, hypoglossal nerve and superior laryngeal nerve are identified . -Bradycardia is common with carotid bulb manipulation. So1% lidocaine without epinephrine may be injected into the areolar tissue around bulb.
- 82. Procedure INCISION: • A horizontal skin incision is outlined and crosshatched at the level of hyoid bone and submandibular gland, two to three fingerbreadths below the angle of the mandible. • It is placed in a skin crease. • The posterior border of the incision is over the SCM.
- 83. • Dissection is carried through skin, platysma, then anterior border of SCM is identified and retracted posteriorly. • A clamp is used to dissect anterior to the muscle parallel to great vessels ,to identify carotid sheath. • The CCA is carefully separated from other contents of sheath. • The IJV, vagus nerve and ansa hypoglossi are retracted posteriorly.
- 84. • Usually at this place a vesicular loop is placed loosely around CCA to obtain control. • Then dissection is carried up along the CCA to the bifurcation area. • At this point hypoglossal nerve is identified crossing the branches, it should be preserved.
- 85. -ECA is usually anterior and superficial to ICA but not always. -A 2-0 silk tie is placed between the superior thyroid and lingual arteries. -The wound is closed in layers after the removal of vesicular loop from CCA .
- 86. COMPLICATIONS: -Damage to vital structures. -Retrograde thrombus formation. -Persistence of bleeding due to collateral flow. -Rarely blindness may occur if ophthalmic artery arises from middle meningeal artery of ECA.
- 87. LIGATION IN RETROMANDIBULAR FOSSA: Done when there are maxillary artery injuries. • Skin incision--- at line starting at the tip of mastoid process , circling the mandibular angle, continuing forward below the mandible one inch. • Skin & posterior fibers of platysma are cut, the retromandibular vein or EJV is located, tied. • Branches of great auricular nerve cut -- permit mobilization of cervical lobe of parotid gland.
- 88. • Attachment of parotid capsule to the anterior border of sternomastoid severed with scalpel. Parotid gland is retracted . • post. Belly of digastric, stylohyoid muscle is visible. Above this stylomandibular ligament can be palpated if lower jaw of the patient is pulled forward. • This movement--- widens the entrance into retromandibular fossa , tenses the stylomandibular ligament. • Pulsations of ECA are felt , isolated & tied.
- 89. ARTERIES OF NECK Subclavian artery&its branches. Vertebral artery Internal thoracic artery Thyrocervical trunk ◦ Inferior thyroid artery ◦ Transverse cervical artery ◦ Suprascapular artery Dorsal scapular artery Costocervical trunk ◦ Deep cervical artery ◦ Superior intercostal artery
- 90. The Subclavian System of Arteries ORIGIN – • Right subclavian art. Arises from the brachiocephalic trunk. • Left subclavian art. arises from the arch of aorta.
- 91. THE SUBCLAVIAN ARTERIES The left subclavian artery arises from the arch of the aorta and after a short course in the thorax it enters the neck. The right suclavian artery arises from the brachiocephalic (innominate) artery. In the neck the scalenus anterior muscle crosses in front of the artery and subdivides it into three parts – first, second and third. The first part extends from its origin to the medial border of the scalenus anterior, the second part lies under the cover of the scalenus anterior while the third part extends from the lateral border of the scalenus anterior or the outer border of the first rib where it is continued as the axillary artery. The first portion of the left subclavian artery is longer than the right.
- 92. Branches of Subclavian • Vertebral, • Internal thoracic • Thyrocervical trunk. • Costo cervical trunk. • Dorsal scapular artery.
- 93. Vertebral Artery 93 • Origin-- from the upper surface of the first part of SC A.passes through- - foramina transversaria of upper six cervical vertebrae, winds backward around the lateral mass of atlas,enters the cranial cavity through foramen magnum, and at the lower border of pons. unites with similar artery of opposite side forms-- the basilar artery. BLOODSUPPLYTOHEAD ANDNECK
- 94. Branches 94 • Cervical branches – ◦ spinal branches – enter the vertebral canal through intervertebral foramina ; supplies spinal cord,meninges, vertebra. ◦ muscular branches – from 3rd part ; supply sub-occipital muscles. B] cranial branches ◦ meningeal branches ◦ posterior spinal artery ◦ ant. Spinal artery., ◦ post. Inferior cerebellar artery, ◦ medullary arteries. BLOODSUPPLYTOHEAD ANDNECK
- 95. Internal ThoracicArtery 95 • Arises from the inferior surface of 1st part of SCA, opposite the origin of thyrocervical trunk.,2cm above the sternal end of clavicle. • BRANCHES --- • Pericardico-phrenic artery. • Mediastinal branches. • Pericardial branches • Sternal branches • Ant. Inter-costal artery. • Perforating artery. • Musculo-phrenic artery. • Superior epigastric artery. BLOODSUPPLYTOHEAD ANDNECK
- 96. Thyro Cervical Trunk 96 • Arises from the upper surface of 1st part of SCA, just distal to the origin of vertebral art. •3 branches : inferior thyroid art. asc. Cervical art. inf laryngeal art. tracheal, oesophageal, laryngeal br. Transverse cervical art. suprascapular art. BLOODSUPPLYTOHEAD ANDNECK
- 97. Costo-Cervical Trunk 97 •Arises from the back of 1st part of SCA on left side2nd part of same art. On rt. Side. Branches – • deep cervical artery • superior intercostal art. BLOODSUPPLYTOHEAD ANDNECK
- 98. Dorsal ScapularArtery 98 Arises from 3rd part of SCA. Passes laterally b/w upper & middle or middle & lower trunks of bracheal plexus. supply the rhomboids & enters in formation of scapular anastamoses. BLOODSUPPLYTOHEAD ANDNECK
- 99. CLINICAL SIGNIFICANCE • Pulse and bleeding • The subclavian arteries have little clinical significance. However, its third part can serve as a useful site for locating arterial pulsations as it lies superficially and can be compressed against the first rib. Also, because of its close relation to the first rib, compression of the subclavian artery against the rib can be used to control bleeding in the upper limb. • Obstruction • Furthermore, like most major arteries, obstruction of the subclavian artery can lead to thrombosis and this can occur following trauma. A syndrome known as Subclavian Steal Syndrome occurs when the blood from the vertebral artery is shunted to the subclavian artery distal to the obstruction in the lumen, depriving the circle of Willis of its posterior input, resulting in specific clinical features. These are: • dizziness • vertigo • imbalance • visual disturbances • hemisensory dysfunction • However, this condition is usually asymptomatic and affects less than 9% of people suffering from occlusion of the subclavian artery.
- 100. SUBCLAVIAN STEAL Occlusion of SCA proximal to origin of vertebral artery results in vertebral acting as collateral to the other arm& stealing flow from the basilar artery.
- 101. COLLATERAL CIRCULATION Definition: It is an accessory circuit which consist of preexisting anastomoses between branches of arteries,when one occludes then these channels become patent above or below the site of occlusion.
- 102. FACTORS AFFECTING COLLATEARAL FLOW Pressure gradient across the site of occlusion Anatomic site of block Rate of occlusion Extent of occlusion Sympathetic activity
- 103. COLLATERALS AFTER LIGATION OF CCA Through subclavian artery, inferior thyroid superior thyroid arteries. Either side of face – ECA. Deep cervical, transverse cervical and occipital arteries anastomoses. Circle of Willis
- 104. REFERENCES • GRAY’S ANATOMY- 39TH EDITION • NETTER’S- COLOUR ATLAS OF ANATOMY • HEAD AND NECK ANATOMY- W.H HOLLINGSHEAD • SICHER’S AND DUBRUL’S ORAL ANATOMY • JOURNAL OF HEAD NECK PATHOLOGY 2009 • INDIAN JOURNAL RADIOLOGY AND IMAGING 2014 • HANDBOOK OF OPERATIVE SURGERY AND SURGICAL ANATOMY- KARUNA K CHATTERJI • PETERSON’S PRINCIPLES OF ORAL AND MAXILLOFACIAL SURGERY
- 105. Thank you