Weitere ähnliche Inhalte
Ähnlich wie Causes and treatment of oedemajhuuhu (20)
Kürzlich hochgeladen (20)
Causes and treatment of oedemajhuuhu
- 1. 156 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
Department of
Cardiology, Hull York
Medical School,
University of Hull,
Castle Hill Hospital,
Cottingham HU16 5JQ,
UK (A. L. Clark,
J. G. F. Cleland).
Correspondence to:
A. L. Clark
a.l.clark@hull.ac.uk
Causes and treatment of oedema in patients
with heart failure
Andrew L. Clark and John G. F. Cleland
Abstract | Oedema is one of the fundamental features of heart failure, but the pathophysiology of oedema
varies. Patients present along a spectrum ranging from acute pulmonary oedema to gross fluid retention
and peripheral oedema (anasarca). In patients with pure pulmonary oedema, the problem is one of acute
haemodynamic derangement; the patient does not have excess fluid, but pulmonary venous pressure rises
such that the rate of fluid transudation into the interstitium of the lung exceeds the capacity of the pulmonary
lymphatics to drain away the fluid. Conversely, in patients with peripheral oedema, the problem is one of
fluid retention. Understanding the causes of oedema will enable straightforward, correct management of the
condition. For patients with acute pulmonary oedema, vasodilatation is important to reduce cardiac filling
pressures. For patients with fluid retention, removing the fluid, using either diuretics or mechanical means,
is the most important consideration.
Clark, A. L. Cleland, J. G. F. Nat. Rev. Cardiol. 10, 156–170; published online 15 January 2013; doi:10.1038/nrcardio.2012.191
Introduction
A striking feature of most patients presenting with heart
failure (HF) is the presence of pulmonary oedema, peri
pheral oedema, or both. Cardiogenic congestion usually
responds well to diuretic therapy, leading to neglect of both
its importance and its cause. The term ‘congestive heart
failure’ has fallen out of favour as patients do not usually
have congestion other than during acute episodes of
HF. Improved understanding of the pathophysiology
of oedema might allow treatments to be used more
effectively, and point the way to new therapeutic targets.
The clinical behaviour of patients with oedema falls
along a spectrum ranging from pulmonary oedema at
one end to peripheral oedema at the other. Patients with
predominant pulmonary oedema are breathless ‘puffers’
and those with predominant peripheral oedema are fluid-
loaded ‘bloaters’. Most patients presenting with severe
HF will lie somewhere along this spectrum. Importantly,
many patients have both pulmonary and peripheral
oedema, but the pathophysiology of the two conditions
is distinct.
HF is a common reason for admission to hospital. In
England and Wales in 2006–2007, there were more than
250,000 deaths and hospital discharges for HF.1–3
Data
from the national audit of HF hospital admissions in the
UK suggest that breathlessness at rest, presumably indi
cating pulmonary oedema, was present in 28% of patients
on admission, with ‘greatly limited exercise capacity’
present in a further 40%, and 43% had moderate or
severe oedema.2,3
Many trials of patients with acute HF
have included patients with little evidence of breathless
ness at rest (Table 1); thus, the evidence-based informa
tion for treating acute pulmonary oedema in particular is
limited. A lot is now known about the best management
of patients with chronic HF, but little attention has been
paid to the management of oedema since the advent of
loop diuretics in the 1960s. New pharmaceutical develop
ments have re-awakened interest in oedema and acute
HF. In this Review, we aim to describe what is known
about the pathophysiology of cardiogenic oedema, and
to discuss how knowledge of the pathophysiology can
guide treatment.
Pulmonary oedema
Pathophysiology and presentation
Acute pulmonary oedema usually presents as a drama
tic medical emergency. The typical patient presents
with a short history (measured in minutes or hours) of
very severe breathlessness. Fluid accumulation in the
lungs results in impaired gas exchange and consequent
hypoxia. Generally, the patient coughs up the oedema
fluid as pink, frothy sputum, and will struggle to speak.
The patient usually needs to sit upright and any attempt to
lay them flat might cause further distress and can be fatal.
Generalized sympathetic nervous system activation results
in tachycardia, cold skin, pallor, sweating and, often, in
systemic (and if measured, pulmonary) hypertension.
Usually, acute pulmonary oedema has a precipitant—
acute ischaemia or myocardial infarction and arrhythmias
(particularly atrial fibrillation) are common contributors,
and acute mitral regurgitation is less so. Chest infection
can both cause, and be a complication of, pulmonary
oedema.4–6
Other causes include a high dietary salt load
and uncontrolled hypertension.
Competing interests
J. G. F. Cleland declares associations with the following
companies: Amgen and Novartis. A. L. Clark declares an
association with Novartis. See the article online for full details
of the relationships.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 2. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 157
The pathophysiology of acute pulmonary oedema is
best understood as a haemodynamic phenomenon. In
the normal circulation, the Frank–Starling mechanism
holds: As the load on the left ventricle increases prior to
theonsetofsystole,sodoestheworkoftheheartduringthe
subsequent contraction (Figure 1). The preload is equiva
lent to the end-diastolic (or filling) pressure in the left
ventricle, and is the same as the left atrial pressure and
pulmonary venous pressure at the end of diastole (in the
absence of mitral valve stenosis).
Another relationship described by Starling explains the
net flow of fluid across a capillary in terms of the forces
acting across the capillary wall.7
Although the balance of
forces changes along the length of the capillary, the major
factor causing the fluid to move out of the capillary is
the difference between the hydrostatic pressure within the
capillary and the lower pressure in the surrounding
interstitial fluid. Opposing this movement is the colloid
osmotic pressure within the capillary, which is mainly
provided by albumin. The colloid osmotic pressure is
higher than the osmotic pressure in the interstitium and
thus tends to keep the fluid in the capillary. A protec
tive mechanism is provided by lymphatic wash-out
of any albumin that reaches the interstitium, result
ing in an increase in the osmotic pressure gradient
between the capillary and the interstitium, which seems
to reduce transudation of fluid.8
In addition, some
resistance to transudation of fluid is provided by the
alveolar–capillary basement membrane.
In the normal circulation, fluid is continuously
transuded from the capillaries into the interstit
ium, and fluid crossing into the interstitial space
is removed by the lymphatic system. The pulmo
nary capillary wall is relatively impervious to fluid,
and the tight apposition of the pulmonary capil
lary and alveolar membranes (the alveolar–capillary
basement membrane) enables efficient gas transfer.
Even if fluid escapes from the capillaries into the
interstitium, provided that it does not spill over into
the alveoli, lymphatic drainage will clear the fluid and the
patient is unlikely to experience breathlessness at rest.
In the failing left ventricle, the curve relating the end-
diastolic pressure to left ventricular work moves down
and to the right. The filling pressure (preload) in the
left ventricle required to deliver a given amount of work
increases. As the left ventricular filling pressure rises,
so does the pressure in the left atrium and pulmonary
capillaries. As hydrostatic pressure increases, capillary
wall tension increases as the fourth power of the radius of
the capillaries, increasing the rate of transmural filtration.
At the same time, lymphatic drainage into the systemic
veins could be impeded by increases in systemic venous
pressure. Eventually, a tipping point is reached when the
capacity of the lymphatic system to remove fluid from
the interstitium is exceeded, and fluid starts to accumulate
in the airspaces of the lungs (alveolar oedema).
Elegant experiments in dogs have demonstrated the
presence of such a critical tipping point. Beyond
the threshold, there is a near-linear relation between the
increase in left atrial pressure and the rate of oedema
formation (Figure 2).9
A reduction in plasma protein
levels reduces the threshold at which oedema starts to
accumulate. Notably, in acute pulmonary oedema the
total amount of fluid in the body does not increase and
the effect of impaired cardiac function leading to haemo
dynamic changes results in fluid moving to the ‘wrong’
body compartment. Indeed, some evidence suggests that
the fluid extravasation into the alveoli results in a reduc
tion in blood volume during acute pulmonary oedema,
which then increases back to normal levels during
successful treatment.10
Key points
■■ Oedema is one of the fundamental features of heart failure
■■ Clinical trial data to guide best practice in managing cardiac oedema are lacking
■■ Acute pulmonary oedema is characterized by accumulation of fluid in the air
spaces, not by fluid overload
■■ Acute pulmonary oedema is best treated as a haemodynamic problem
using vasodilators
■■ Peripheral oedema is characterized by an excess of total body water
■■ Peripheral oedema is best treated by removing fluid, either with diuretics
or mechanically
Table 1 | Trials of patients with acute heart failure
Study
name
Intervention Mode
of action
Mean
patient
age
(years)
Women
(%)
Systolic
blood
pressure
(mmHg)
Heart
rate
(per
min)
Respiratory
rate
(per min)*
LVEF
(%)*
β-blocker
use (%)
Digoxin
use (%)
Time
to study
inclusion
30-day
mortality
(%)
VERITAS63
Tezosentan Endothelin
antagonist
70 40 131 81 26 [24] 29
[40]
48 21 24 h 4
SURVIVE87
Levosimendan Calcium
sensitizer
67 28 116 84 NR 24
[30]
51 NR NR 13
EVEREST180
Tolvaptan Vasopressin
antagonist
66 26 120 80 NR 28
[40]
70 46 48 h 5
ASCEND68
Nesiritide Natriuretic
peptide
67 34 124 82 23 40
in 81
NR NR 48 h 4
PROTECT187
Rolofylline Adenosine
antagonist
70 33 124 80 21 32
[any]
76 28 24 h 15
3CPO43‡
C-PAP NA 78 57 161 114 33 [20] NR NR NR NR 16
*Numbers in square brackets denote the upper limit permitted by the trial design. ‡
3CPO trial included ‘puffers’; the other trials included ‘bloaters’. Abbreviations: C‑PAP, continuous positive
airways pressure; LVEF, left ventricular ejection fraction; NA, not applicable; NR, not reported.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 3. 158 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
A patient with acute pulmonary oedema classically pre
sents with a high left ventricular filling pressure and high
systemic vascular resistance.11
Some patients present with
pulmonary oedema owing to uncontrolled hypertension.
In these cases, the problem is an increase in the left ven
tricular afterload and consequent rise in filling pressure
required to maintain cardiac output. Hypertension, which
can occur as a result of an acute salt load or a phaeo
chromocytoma, might cause recurrent episodes of ‘flash’
pulmonary oedema; that is, very abrupt onset of episodes.
Such events are commonly associated with hypertension
and, in particular, with renal artery stenosis.12
Flash
pulmonary oedema often happens in the presence of
normal left ventricular systolic function, highlighting the
involvement of the neurohormonal system in the genesis
of acute pulmonary oedema.13
Angiotensin II seems to
have a particularly important role in flash pulmonary
oedema. When infused into renal arteries at a low perfu
sion pressure (mimicking renal artery stenosis), angio
tensin II causes marked systemic hypertension, salt and
water retention, and pulmonary oedema.14
The role of abnormalities in the pulmonary vascula
ture, the alveolar–capillary membrane, and the alveo
lar wall itself in the development of acute pulmonary
oedema is not clear. Some evidence suggests that high
catecholamine levels, as seen in patients with a phaeo
chromocytoma, may cause an increase in pulmonary
capillary permeability resulting in pulmonary oedema
without a great increase in left ventricular filling pres
sure.15
In high-altitude pulmonary oedema, capillary
stress fracture can contribute to the development of
oedema, although the major cause of pulmonary oedema
is excessive hypoxia-induced pulmonary hypertension.16
In adult respiratory distress syndrome, damage to the
alveolar–capillary membrane caused by inflammation,
infection, trauma, or toxins might cause pulmonary
oedema to develop even if the left atrial pressure is not
increased.17
Some researchers have drawn attention
to the possible contribution of a generalized inflam
matory state, resulting in endothelial dysfunction in
patients with chronic HF.18
However, there is no good
evidence that such mechanisms have a major role in the
development of acute cardiogenic pulmonary oedema.
Another potential contributor to pulmonary oedema
formation is sleep-disordered breathing, which is
very common in patients with HF.19
Recurrent airway
obstructions have been shown to precipitate pulmo
nary oedema in a dog model.20
In addition, patients
with sleep apnoea have a higher salt intake than those
without.21
The induction of negative alveolar pressure
during airway obstruction could increase transudation
of fluid into airspaces. Distinguishing between arousal
from sleep apnoea and paroxysmal nocturnal dyspnoea
is difficult; the relationship between the two conditions is
not yet clear.
Intriguingly, some patients with chronic HF can toler
ate extremely high left atrial pressures that would provoke
severe pulmonary oedema in an otherwise healthy person.
This observation might indicate increased pulmonary
lymphatic drainage,22
particularly in patients with mitral
stenosis.23
Alternatively, the alveolar–capillary membrane
may become thickened, reducing pulmonary microvas
cular permeability.24,25
Such changes are consistent with
the observation that the diffusing capacity of the alveolar–
capillary membrane is reduced in patients with chronic
HF.26
Increases in pulmonary arteriolar tone could reduce
pulmonary blood flow and capillary distension, protecting
the lung from oedema. In healthy individuals, little smooth
muscle is present in the precapillary pulmonary arterioles,
but in the setting of chronic disease, smooth muscle cell
hypertrophy occurs, enabling powerful vasoconstriction.25
Left ventricular preload
Leftventricularwork
Figure 1 | The Frank–Starling law of the heart. In the
healthy heart (blue line), increasing preload results in
greater ventricular work. In the failing heart (red line),
the curve moves down and to the right. Thus, to attain
a particular amount of left ventricular work, the required
filling pressure is greater (indicated by arrow).
0 10 20 30
Left atrial pressure (mmHg)
Rateofoedemaformation
50
0
6
4
3
2
1
7
5
40
Figure 2 | The correlation between increasing left atrial
pressure and the rate of development of pulmonary
oedema. No oedema forms until left atrial pressure
reaches a critical threshold (around 25 mmHg), and
thereafter, left atrial pressure is directly related to the rate
of oedema development. Permission obtained from Walters
Kluwer Health © Guyton, A. C. Lindsey, A. W. Effect of
elevated left atrial pressure and decreased plasma protein
concentration on the development of pulmonary oedema.
Circ. Res. 7, 649–657 (1959).9
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 4. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 159
Treatment
An X‑ray of the chest shows why acute pulmonary
oedema is a medical emergency. Fluid initially collects
in the interstitial spaces, resulting in stiff lungs and an
increase in the work of breathing. Subsequently, the air
spaces are filled with fluid, leading to gross impairment
of pulmonary gas exchange (Figure 3).The prognosis is
bleak following acute pulmonary oedema, with an in-
hospital mortality of 10–20%, varying greatly with age
and presence of comorbidity.6
The 1‑year mortality is
at least 20% in patients with the lowest blood pressure
(systolic 100 mmHg) at admission.27
These data conceal
the outcome for more severely affected patients. In the
EFICA study28
of patients admitted to high-dependency
units with acute severe HF (82% of whom had pulmo
nary oedema), mortality was 27.4% at 4 weeks and 46.5%
at 1 year, but when preadmission deaths were included,
mortality was 43.2% and 62.5% at the two time points,
respectively. These data highlight the potential impor
tance of delivering treatment to patients with severe HF
as quickly as possible.
The evidence-based information for the treatment
of patients with acute pulmonary oedema is minimal,
particularly compared with that for the management of
chronic HF. Patients often present in the middle of the
night with acute severe symptoms, which makes their
recruitment into clinical trials difficult. Consequently,
the following discussion is based on many small studies
and is not definitive. Few randomized trials have been
able to allocate patients to different interventions within
6 h of presentation, and yet surveys show that most
patients have already responded symptomatically to
conventional treatment within that time frame.29
Quicker
relief of symptoms would be welcomed by all clinicians
and patients, but designing studies with intervention
within the first 2 or 3 h of presentation is difficult.
Although large, randomized, controlled trials have
been conducted in patients with acute HF, few of these
individuals had severe pulmonary oedema. Many
patients were comfortable at rest, and only developed
symptoms during slight exertion. Most patients were
‘bloaters’, rather than ‘puffers’ (Table 1). In many studies,
haemodynamic end points, such as left ventricular filling
pressure, but not symptoms, morbidity, or mortality, have
been measured. Haemodynamic end points might be
easier to achieve and could also be biased by the investi
gators’ judgement about patients’ symptoms. Perhaps
crucial to the success of new therapies, particularly for
acute severe pulmonary oedema, is the timing of treat
ment administration. The information about the timing
of intervention is often not available from trials. Early
intervention, when symptoms are most severe, might
lead to rapid resolution of symptoms, but would require a
study to be conducted during a time window of 6 h from
presentation or an even shorter duration. Alternatively,
delaying intervention until patients have failed conven
tional treatment would identify those with recalcitrant
symptoms requiring novel therapies.
The immediate aims of management include the
relief of anxiety and improvement in oxygenation whilst
instituting medical therapy in an attempt to reverse
the haemodynamic cause of pulmonary oedema. As the
problem is not so much one of excess fluid, but of fluid
in the wrong body compartment, the key strategy is to
drive fluid from the lung tissues back into the circula
tion. This aim can be achieved either by reducing pulmo
nary capillary hydrostatic pressure, increasing lymphatic
drainage by reducing systemic venous pressure (both
achieved with vasodilators), pushing fluid out of the
alveoli (achieved in part by ventilator support), or alter
ing pulmonary capillary permeability (with experimental
agents). An important part of the management strategy
is to try to reverse any potential precipitant of pulmo
nary oedema, such as myocardial ischaemia, arrhythmia,
mitral regurgitation, or infection; however, this topic is
not discussed further here.
Opiates
Opiates are often used to relieve distress, anxiety, pain,
and the sensation of breathlessness. The 2008 ESC guide
lines for the management of acute HF from the state that
“[morphine] should be considered in the early stage of
the treatment of patients admitted with severe [acute
HF]”.30
The recommendation is made on the basis of
opinion rather than clinical trial data, although small
studies suggest that opiates (diamorphine is often used
in the UK31
) might be effective vasodilators. The updated
guidelines published in 2012 still suggest that opiates
might be helpful.32
Opiates undoubtedly ease the pain of myocardial
infarction and relieve distress, but no good evidence
exists to suggest that their use improves outcomes.
Although morphine might induce some relaxation of
vascular smooth muscle,33
the effect seems to be medi
ated by histamine release rather than by a direct effect of
opiate receptor stimulation.34
Some case reports suggest
that morphine can directly cause worsening of left
ventricular function and even induce shock.35
In a review
of the small number of published trials of opiates in acute
pulmonary oedema, investigators found that although
opiates did relieve anxiety, their use was associated with
Figure 3 | X‑ray of the chest of a patient presenting with
acute pulmonary oedema. The air spaces are bilaterally
filled with oedema fluid.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 5. 160 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
an increase in mortality and the need for intubation.36
In
a retrospective study of nearly 150,000 patients admit
ted to hospital for acute decompensated HF, opiate use
(in 20,000 patients) was associated with poor outcomes
and an odds ratio for mortality of 4.84.37
Although no
definitive evidence of harm with opiate use exists, the
data do not support the routine use of opiates in acute
pulmonary oedema, and these drugs should be used with
caution, if at all.
Oxygenation and ventilatory support
Patients with hypoxia should be given oxygen. No studies
have shown that oxygen helps patients without hypoxia.38
The breeze caused by high air flow and the oxygen mask
might be a comfort for some patients and a source of
anxiety for others. Care should be taken not to overdose
patients with oxygen if they have chronic lung disease
and are at risk of CO2
retention. Ventilatory support
might be necessary. Patients can get tired, or their gas
exchange worsen, despite medical therapy. Invasive
ventilation temporarily reverses the situation,39
immedi
ately removes the work of breathing, can directly reduce
alveolar oedema by applying positive airway pressure,
and improves gas exchange.40
Ventilatory support falling short of endotracheal
intubation and invasive ventilation can be helpful.
Continuous positive airway pressure (CPAP) ventilation
and bilevel positive airway pressure (BiPAP) ventilation, in
which positive pressure is applied to the airway both
during inspiration and expiration, have been the most
widely studied types of ventilatory support. The two
modes of ventilation are collectively known as non
invasive positive pressure ventilation (NIPPV). The
evidence to support the use of prehospital noninvasive
ventilation is limited, but suggests that preadmission
CPAP improves the clinical state of patients arriving at
hospital, and reduces the need for invasive ventilation.41
Importantly, CPAP might reduce cardiac output by
squeezing pulmonary capillaries and increasing resist
ance to pulmonary blood flow, but meta-analyses suggest
that NIPVV might be beneficial for patients once they
have arrived in hospital.42
However, in the 3CPO trial,43
almost 1,000 patients were randomly allocated to CPAP,
BiPAP, or routine oxygen therapy and no difference was
found in short-term mortality or the need for intuba
tion among the three groups, although a small improve
ment was observed in dyspnoea at 1 h with NIPPV. The
3CPO study is, to date, the largest study of ventilation
techniques and the only large clinical trial conducted
primarily among ‘puffers’.
Diuretics
Standard practice in the management of acute pul
monary oedema has been the use of intravenous loop
diuretics, as the ensuing diuresis is understood to
remove the fluid in the lungs. Certainly, loop diuret
ics reduce circulating fluid volume and, consequently,
filling pressure, but they may also have bradykinin-
mediated vasodilator effects. The notion that loop diu
retics reduce preload through venodilatation, and that
the venodilatation occurs before any increase in urine
flow, is firmly entrenched, but the data are weak and
controversial.44
Some investigators have reported rapid
reductions in filling pressure following intravenous
furosemide,44
others report slow changes45
and empha
size that changes in haemodynamic variables are seen
only in patients with a subsequent diuresis.46
One small
study suggested that furosemide does not relieve symp
toms in acute pulmonary oedema.47
In anuric patients
undergoing haemodialysis, neither low-dose nor high-
dose furosemide had an effect on central haemodynamic
variables.48
Others have found that furosemide causes an
increase in peripheral vascular resistance and a decrease
in stroke volume when administered acutely.45,49
Part of
the difficulty in sifting through the data on haemody
namics with furosemide is that most patients included
in studies had had an acute myocardial infarct and thus
their condition was inherently unstable.
Anecdotal reports exist on the use of nebulised furo
semide in patients with end-stage HF.50
Furosemide has
also been used to ease breathlessness in patients with
terminal cancer.51
Nebulised furosemide seems to have
no effect on haemodynamics in patients with chronic,
severe HF, although it does have a diuretic effect,52
and
might become more widely used in treating people with
end-stage disease at home.
Vasodilators
Although diuretics are the most-widely prescribed agents
for acute HF syndromes,53
the best approach to treating
acute pulmonary oedema is to reduce left ventricular
filling pressure (and any mitral regurgitation), which is
easily accomplished using nitrovasodilators (Figure 4).
These drugs reduce preload and afterload, increase
cardiac output, and help to reduce any myocardial
ischaemia. Very little data exist for the direct compari
son between vasodilators and loop diuretics, but vaso
dilators seem to result in more-pronounced reductions
in filling pressures and an increase in cardiac output,
compared with no change or a modest decline in cardiac
output with furosemide.54–56
In a study in which patients were treated in mobile
emergency units delivering intensive therapy much
more quickly than usual, Cotter and colleagues showed
that high-dose nitrate therapy (with low-dose furo
semide) was probably more effective than high-dose
furosemide and low-dose nitrate.57
High-dose nitrate
therapy was associated with a reduced need for intubation
and a lower risk of myocardial infarction. Some studies
suggest that a high-dose nitrate strategy is of greater
benefit and is possibly safer than routine use of NIPPV
and low-dose nitrate.58
Some evidence indicates that acute administration
of an angiotensin-converting-enzyme (ACE) inhibitor
might relieve pulmonary oedema more rapidly than
standard therapy alone.59
Tezosentan, an endothelin
antagonist, acutely reduces pulmonary vascular resist
ance,60
but had no effect on outcomes in a study of
84 patients with pulmonary oedema.61
In large studies
of acute HF, such as the RITZ62
and VERITAS63
trials,
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 6. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 161
tezosentan given at a variety of doses had no positive
effect on outcome. Tezosentan did reduce left ventri
cular filling pressure and increase cardiac output, but
these apparently beneficial effects were accompa
nied by pulmonary vasodilatation and a reduction in
arterial oxygen saturation, suggesting shunting of blood
through unoxygenated lung tissue.64
In a study of 1,613
patients, another endothelin antagonist, bosentan, was
shown to have neutral effects in chronic HF.65
Endothelin
antagonists are currently mainly used for treating
pulmonary hypertension.
Natriuretic peptides have attracted a great deal of
interest as possible agents for the treatment of acute
pulmonary oedema. The recombinant human B‑type
natriuretic peptide, nesiritide, causes vasodilatation,
reducing both afterload and preload and causing natri
uresis.66
Nesiritide was approved for use in the USA
following publication of a study showing haemodynamic
benefits of the drug in patients with acute HF,67
but the
European regulatory authorities were not convinced
of its efficacy. Subsequently, in a study involving 7,000
patients with acute HF,68
nesiritide was shown to have
no effect on symptoms, or on the rates of rehospitaliza
tion or death. Some evidence indicates that natriuretic
peptides might increase capillary permeability,69,70
which might counteract the other beneficial effects of
these agents.
Other vasodilators that are in development include
relaxin, a potent hormone responsible for vaso
dilatation during pregnancy. Relaxin is an arterial
vasodilator that might also have some inotropic effect,
but seems not to reduce venous tone.71
The lack of
venodilatation might explain why relaxin does not
cause syncope to the same extent as other vasodila
tors. Syncope caused by peripheral pooling of venous
blood is resistant to therapy and can be difficult to
manage in patients with acute pulmonary oedema,
for whom lying flat is contraindicated. Keeping the
feet elevated is advisable in this case, while the clini
cian considers what else can be done. In early studies,
relaxin was associated with faster improvement in
symptoms than placebo and a possible improvement in
outcome.72
In a study of 1,161 patients with acute HF,
relaxin was shown to improve breathlessness to a greater
extent than placebo.73
Relaxin use was associated with
a lower mortality at 6 months than placebo, but had
no effect on the rate of readmission to hospital for HF
or renal problems.73
The number of adverse events
was small, and if the beneficial effects are confirmed
by further studies, relaxin could be an enormous step
forward in the management of acute HF.
Another novel arterial vasodilator is clevidipine, an
extremely short-acting dihydropyridine calcium antag
onist (with a half-life measured in several seconds). In
the PRONTO study of 104 patients with acute pulmo
nary oedema and hypertension who were recruited
within a few hours after presenting with symptoms,
clevidipine was associated with a faster reduction
in blood pressure and relief of breathlessness than
standard treatment.74
New pharmacological approaches
Clearance of pulmonary oedema is, at least in part, an
active process, involving an epithelial amiloride-sensitive
sodium channel, sodium potassium ATPase, and possi
bly aquaporins.75,76
Alveolar sodium uptake might be
enhanced by β2
-adrenergic receptor stimulation,77,78
but
no convincing clinical data are yet available.79
The transient receptor potential channel TRPV4 is a
calcium-permeable channel that has been implicated in
disruption of the alveolar membrane during the develop
ment of pulmonary oedema. Research in a mouse model
suggests that inhibiting TRPV4 with the investigational
compound GSK2193874 might speed recovery from or
prevent cardiogenic pulmonary oedema.80
Native soluble guanylate cyclase (sGC) requires a
haem moiety to be activated. Cinaciguat is a nitric oxide
(NO)-independent direct activator of haem-free sGC
that causes pulmonary and systemic vasodilatation.81
Excessive reductions in blood pressure have been a limit
ing factor for cinaciguat use to date, but adjustment of
dose and target population might enable it to become a
useful drug.81
Other agents have been developed, such
as riociguat, to stimulate sGC in the presence of haem.
Both riociguat and cinaciguat might have other effects on
endothelial, renal,82
and myocardial83
function, which are
independent of their haemodynamic effects.
Inotropic support
Positive inotropic drugs are commonly used for patients
with pulmonary oedema when cardiac output, blood
pressure, or both, are low and when the patient is
resistant to immediate therapy. Dobutamine is most
widely used, but little evidence exists to support this
practice. In a randomized trial comparing the effects of
dobutamine and nitroprusside in patients with severe
HF, nitroprusside was safer.84
Furthermore, the results
Vasodilation Vasoconstriction
Exogenous
nitrate
Relaxin Cinaciguat NP Endothelin
antagonist
Endothelium
NO cGMP
cGMP cGMP
Smooth muscle cells
sGC
NOS
GC
Endothelin
Figure 4 | Schematic representation of possible routes through which vasodilators
exert their action. A schematic drawing of arteriolar wall is shown. Vasodilators
cause smooth muscle relaxation, either via interaction with receptors in the
endothelium (relaxin, NP) or via interaction with the smooth muscle itself
(nitrate, cinaciguat). Endothelin antagonists mediate their effects by blocking
the interaction of endothelin with its receptor on vascular smooth muscle.
Abbreviations: cGMP, cyclic GMP; GC, guanylate cyclase; NO, nitric oxide; NOS,
nitric oxide synthase; NP, natriuretic peptide; sGC, soluble guanylate synthase.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 7. 162 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
of a meta-analysis of the available data suggest that
positive inotropic support with agents working through
adrenergic pathways (both β‑adrenergic agonists and
phophodiesterase inhibitors) is associated with a worse
outcome than placebo.85
Levosimendan, an agent that
is both a calcium-concentration-dependent calcium
sensitizer and arterial vasodilator, could be useful in
patients with severe chronic HF,86
but its effects do not
seem to translate into a benefits in the acute setting.87,88
Myosin activators enhance actin–myosin binding,
increasing the efficiency of ATP utilization and pro
longing the duration of systole.89
These actions increase
stroke volume and cardiac output without increasing
the inotropic state of the myocardium (and, therefore,
without increasing the amount of energy consumed).90
Myosin activators are thus very different from dobuta
mine, which increases the force of contraction and
energy consumption, but shortens systole. A trial of
myosin activators in patients with acute HF is ongoing.91
Istaroxime stimulates the reuptake of calcium by the
sarcoplasmic reticulum during diastole, while increas
ing the available intracellular calcium during systole
by blocking the sodium pump (as does digoxin). In the
phase II HORIZON-HF trial,92
conducted in 120 patients
with acute HF, istaroxime was shown to improve diastolic
function, reduce left ventricular filling pressure, increase
blood pressure, and decrease heart rate.93
Mechanical support has a role in selected patients, par
ticularly in those in whom the cause of the pulmonary
oedema can be resolved. Anecdotally, intra-aortic balloon
counterpulsation can be effective in bridging patients to
surgery for severe acute mitral regurgitation. However, the
results of the SHOCK-II trial94
suggested that intra-aortic
balloon pump had no survival benefit in patients with
cardiogenic shock receiving primary angioplasty for acute
myocardial infarction.95
Other approaches include left
ventricular assist devices and pumps inserted transcutane
ously.96
At present, the role of these devices is restricted to
carefully selected patients in specialist centres. Reducing
venous return to the heart by occluding the inferior vena
cava has also been tried in a small study.97
Peripheral oedema
Pathophysiology and presentation
At the other end of the spectrum from pulmonary
oedema is peripheral oedema, also known as anasarca,
which occurs when fluid retention is severe and general
ized. Two processes are involved in the development of
peripheral oedema: an increase in total body fluid and
transfer of fluid into the tissues. The latter is a straight
forward process. As with pulmonary oedema, tissue
oedema forms when the capillary hydrostatic pres
sure exceeds the plasma colloid osmotic pressure by an
amount sufficient for the rate of transudation from capil
lary into tissue to exceed the rate at which the lymphatic
system can drain away the fluid from the interstitium.
Capillary permeability is again important. The upright
posture causes an increase in the hydrostatic pressure in
the lower extremities. Therefore, in ambulant patients,
fluid first begins to accumulate in lower parts of the
body. An unwary doctor might be caught out by a patient
who has been confined to bed for several days in whom
the fluid has migrated from the legs to the sacral region.
Traditional understanding is that sodium handling is
the primary abnormality involved in oedema formation,
whereby water movement passively follows salt move
ment. Total body sodium level is certainly increased
in patients with HF, especially if they have peripheral
oedema,98
but also in those without oedema.99
However,
patients are oedematous because they have an excess of
body fluid,100
not because they have an excess of sodium.
Why do patients with a failing heart have excess
fluid? Two possible reasons are excessive fluid intake
and inadequate fluid loss. Harris drew attention to the
concept of HF as a by-product of mammalian (and
human) evolution.101
A high arterial blood pressure is
required to sustain the high metabolic rate required for
rapid movement of a mammal (and the upright posture
of a human). As the heart fails, blood pressure starts to
decrease and the body responds in the same way as it
would to the volume contraction that might occur with
dehydration or haemorrhage. The ‘set-point’ for blood
pressure varies from one individual to another and, at
least in industrialized societies, rises with age.102
The
body might be more sensitive than a sphygmomanometer
in detecting deviation from its ‘desired’ blood pressure.
The neurohormonal response is determined by the need
to maintain blood pressure and, thus, tissue perfusion.
Since the 1940s, we have known that renal perfu
sion decreases and the kidneys retain sodium as HF
develops.103
This process is mediated, in part, by the
production of renin in the juxtaglomerular appara
tus of the kidney. As mean arterial pressure decreases,
more renin is produced,104
leading to increased
production of angiotensin I and angiotensin II
and, ultimately, aldosterone. The renin response is
enhanced by the concomitant sympathetic nervous
system activation caused by HF,105
and by aldoster
one, which causes sodium and water retention in
the distal convoluted tubule (DCT) of the nephron.
The fact that neuroendocrine activation is not the
only cause for salt and water retention is indicated by the
Figure 5 | The right thigh of a patient presenting with fluid
retention and pitting oedema. The patient subsequently
lost 23 kg in weight (equivalent to 23 l of fluid).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 8. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 163
observation that intensive blockade of multiple neuro
endocrine systems does not overcome the avidity with
which the kidney retains salt and water, perhaps because
the underlying cause for the decrease in blood pressure
has not been corrected. Powerful diuretics are required to
‘poison’ renal function. Restoration of blood pressure can
reverse sodium retention, but exactly how blood pressure
mediates salt and water retention is unclear.
In addition to activation of the renin–angiotensin–
aldosterone system, production of antidiuretic hormone
(ADH; or arginine vasopressin) by the anterior pituitary
gland is increased. ADH has an important role as an
‘osmostat’, being released in response to a rise in osmo
lality and causing a decrease in renal free water clear
ance to restore osmotic balance. ADH mediates its effects
through mobilizing aquaporin channels in the collect
ing duct of the nephron, which increases the movement
of water from the lumen of the nephron to the medulla of
the kidney.106
ADH is also a systemic vasoconstrictor and
increases platelet activation. Other nonosmotic stimuli
leading to the release of ADH include a reduction in
blood pressure and a rise in angiotensin II level.107,108
ADH level rises as HF becomes more severe,109
causing
renal water retention. However, because the stimulus
is nonosmotic, increased ADH production might lead
to hyponatraemia.110
Thirst can be a prominent symptom in patients with
HF,111,112
even in elderly patients,113
in whom the sensa
tion of thirst is otherwise often impaired.114
This finding
could reflect neuroendocrine activation, particularly of
angiotensin II115,116
and ADH, which might have addi
tive effects.117
Thirst is often exacerbated by the common
practice of restricting fluid intake, although no evidence
has shown that such a practice improves outcomes,118
particularly in stable patients.119
Peripheral oedema usually develops gradually.
Around 5 l of excess fluid (and a consequent weight gain
of ~5 kg) accumulates before peripheral, pitting oedema
forms, but this volume may be less if the patient has
a low albumin level, remains seated and immobile for
a long time, or has varicose veins, or ulcers, or both.
Because the fluid gain can be gradual, some patients do
not attend hospital until they have accumulated ≥20 l of
fluid (Figure 5), by which time pitting oedema might
form in the abdominal or even the thoracic wall, as
well as pleural and pericardial effusions. The distribu
tion of fluid in some patients is rather even, and severe
oedema might be missed in a casual physical examina
tion because the patient’s legs might be thickened but
maintain their normal form.
Treatment
In contrast to patients with pulmonary oedema, patients
with peripheral oedema have the problem of an abso
lute excess of fluid, and the mainstay of treatment is to
try to remove the fluid. Careful monitoring of patients
is important during fluid removal, with at least daily
measurements of urea, creatinine, and electrolyte levels,
and body weight. Fluid balance should be recorded
with care. Bed rest is appropriate120
and some studies
performed before modern diuretic therapy was available
showed that bed rest alone could help patients to lose
the fluid.121
Diuretics might be most effective when the
patient is in supine position.122
Keeping the legs elevated
could help fluid removal, allowing gravity to aid the
reabsorption of oedema, but can acutely increase cardiac
filling pressures and should be avoided in patients with
incipient pulmonary oedema.123
Prophylactic low-
molecular-weight heparin is usually given, as patients
with HF are prone to venous thromboembolism. Using
compression stockings might help to force fluid back into
the circulation and might also reduce the risk of venous
thrombi formation.124
The time course of weight loss in
a typical patient is shown in Figure 6.
A key factor in treating patients with cardiogenic
oedema is renal function. Renal dysfunction is a common
comorbidity in patients with HF,125
and as renal function
deteriorates, so does the response to diuretics.126
The origin of renal dysfunction is multifactorial127
(Box 1), with both the HF syndrome alone and intrin
sic renal disease being implicated. Most successful
medical therapies for HF (β-blockers, ACE inhibitors,
and mineralocorticoid antagonists) and diuretics cause
a decline in renal function. Treatment for oedema often
exacerbates renal dysfunction,128
which could reflect
adenosine-mediated increases in sodium reabsorption in
the proximal renal tubule.129
However, studies of adeno
sine antagonists, such as rolofylline, in patients with
acute HF have been unsuccessful.130
Several treatment
strategies are available for management of patients with
renal impairment.
5 Sep 10 Sep 15 Sep 20 Sep
Admission dates in 2006
Volume(l/24h)
25 Sep 30 Sep 5 Oct
–8,000
8,000
4,000
0
–4,000
–6,000
10,000
6,000
2,000
–2,000
Weight(kg)
40
60
50
70
Furosemide
infusion
Input
Output
Balance
Weight
Figure 6 | Pattern of weight loss in a patient presenting with peripheral oedema.
During the first 10 days after admission, oral diuretics had no effect. An
intravenous infusion of furosemide is followed by immediate diuresis, negative
fluid balance, and weight loss.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 9. 164 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
Diuretics
In the normal kidney, 99% of filtered sodium is usually
reabsorbed; 60–70% in the proximal tubule, 20–25% in
the loop of Henle, 5–10% in the DCT, and 3% in the col
lecting duct.131
Loop (or ‘high ceiling’) diuretics block the
sodium–potassium–chloride cotransporter in the thick
ascending loop of Henle. They work from the luminal
surface of the nephron and hence are dependent on the
presence of some glomerular function. These agents
work within minutes of intravenous administration, but
are short acting after a single-dose.132
As much of the
filtered sodium is reabsorbed by the loop of Henle, loop
diuretics are very potent. They increase sodium excre
tion, but the urine is hypotonic as free water clearance
increases, contributing to hyponatraemia. Loop diuretics
also increase excretion of potassium and calcium.132
Thiazide diuretics work in the DCT of the nephron.
They are less potent than loop diuretics, as less sodium is
reabsorbed at this site, but they have a longer duration of
action. Thus, the overall effect of thiazide and loop diure
tics on total daily sodium excretion was similar in some
studies.133,134
Thiazides cause more electrolyte distur
bances than loop diuretics,132
but cause calcium reten
tion,135
which could be why patients with hypertension
using thiazides have a low fracture rate.136
Metolazone, a
thiazide-like diuretic, is widely used to relieve fluid reten
tion caused by HF; this drug might have some effects in
the proximal tubule, and remains effective in patients
with renal impairment.137
As metolazone is only used
in conjunction with loop diuretics for treating severe
oedema and is rarely used for hypertension, use of this
drug stops less-well-informed clinicians being confu
sed about the purpose of the thiazide, as other types of
thiazides are used for other indications.
Potassium-sparing diuretics work on the DCT where
they block the sodium–potassium exchanger. Loop
and thiazide diuretics increase the sodium load in the
DCT, leading to increased activity of the exchanger and
loss of potassium. Potassium-sparing diuretics have
little diuretic effect when used alone, but can prevent
hypokalaemia when used with other diuretics.138
Spironolactone and eplerenone are potassium-sparing
diuretics that block the effects of aldosterone on the
sodium–potassium exchanger. They are principally
used as disease-modifying agents, rather than for their
diuretic effects.139,140
However, in patients with gross
oedema, liver congestion prevents the degradation of
aldosterone, which might then have an increased role
in the genesis of fluid retention. The use of aldosterone
antagonists in this setting, especially at high doses, could
produce diuresis141
and might prevent hypokalaemia.
As HF worsens, systolic arterial pressure decreases
and central venous pressure rises, thus reducing the
filtration pressure across the glomerulus. Loop diuretics
increase the sodium load to the DCT, resulting in tubular
hypertrophy and an increase in its capacity to reabsorb
sodium.142,143
The DCT adaptation is particularly impor
tant with intermittent diuretic dosing, because in the
absence of diuretic between doses, the hypertrophied
DCT will enable rebound reabsorption of sodium.
Intravenous administration of diuretics is usually more
effective than oral dosing. Furosemide, in particular,
has a variable bioavailability, which may be marked in
patients with bowel wall oedema.144,145
Continuous intra
venous infusion of loop diuretic can avoid some of the
problem of diuretic ‘braking’ (that is, the general problem
of a diminishing response to diuretics)146–151
and seems
to offer a greater dose-for-dose natriuresis than repeated
bolus administration. The DOSE trial152
is the only sub
stantial study in which various diuretic strategies have
been compared. In a two-by-two factorial design, 308
patients were randomly assigned to receive intravenous
furosemide at low or high dose, either as a continuous
infusion or by repeated boluses. Greater diuresis and a
slightly greater reduction in dyspnoea occurred in the
high-dose groups than in the low-dose groups at 72 h,
although the high dose was associated with a slightly
greater decline in renal function. No difference in diuresis
was found for continuous and bolus administration.152
An alternative strategy would be to give thiazide diure
tics orally in addition to either bolus or continuous intra
venous therapy. The best loop diuretic dosing strategy
for patients with gross fluid retention remains unclear.
Combination diuretic therapy, sometimes called
sequential nephron blockade, involves a loop diuretic
used with a thiazide. The subsequent diuresis can be
profound,153,154
and patients should be closely moni
tored when combination treatment is used. Metolazone
is the thiazide most often used in combination therapy.
However, in the only comparative trial of this strategy, no
difference was found between metolazone and another
thiazide diuretic, bendroflumethiazide.154
No study has
provided definitive evidence that sequential nephron
blockade is better than simply increasing the dose of
intravenous loop diuretic.
Discontinuation of potentially nephrotoxic drugs
while trying to initiate diuresis is essential. Nonsteroidal
anti-inflammatory drugs, including aspirin, can blunt
the effects of diuretics.155
Whether other HF medication
should also be stopped is not clear. The standard advice
is to reduce or stop β‑blocker therapy when the patient is
admitted to hospital, but some provisional evidence sug
gests that those who continue to receive β‑blockers once
they are admitted have a better outcome than those who
stop taking β‑blockers.156,157
The interest in digoxin has declined, perhaps owing
to the large DIG study,158
which showed no survival
benefit for digoxin in patients with chronic HF. However,
Box 1 | Causes of renal impairment in heart failure127
Predominantly cardiac
Decreased systemic arterial blood pressure
Increased central venous pressure
Increased renal venous pressure by renal oedema
Afferent glomerular arteriolar vasoconstriction
Intrinsic renal
Diabetes
Hypertension
Atherosclerosis
Iatrogenic
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 10. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 165
digoxin has a diuretic effect,159
as well as a positive ino
tropic effect, and some evidence from the DIG trial
indicates that digoxin might reduce the risk of hospitali
zation and mortality in patients with low serum digoxin
concentration.160
The effect of digoxin in patients with
acute HF is not well studied, and digoxin will largely
remain an adjunct to conventional therapy until more
data become available.
Anecdotal evidence exists that, once a patient has
achieved ‘dry weight’ (the weight that they were at before
developing oedema), their diuretic requirement might be
reduced and they could be discharged from hospital to
receive loop diuretics at similar doses to those they were
taking before admission. Presumably, this observation
represents resolution of renal venous hypertension and
reduced ventricular volume.
Ultrafiltration
For many years, ultrafiltration has been known to be an
extremely effective method for rapid removal of fluid
from patients with oedema.161
In veno-venous ultra
filtration, venous blood is pumped out from the patient,
usually using a rotary pump. As the blood passes through
an extracorporeal filter, hydrostatic pressure forces fluid
out of the blood, taking with it some solutes, particu
larly sodium and potassium. The ‘concentrated’ blood
is then returned to the patient. With ultrafiltration, 5 l
of fluid can be safely removed from a patient in 24 h.162
In the RAPID-CHF trial, however, even faster removal
of 3 l of fluid in 8 h was shown to be safe and effec
tive.163
Ultrafiltration might be useful for patients who
are refractory to diuretics, and could also trigger renal
diuresis, presumably owing to a reduction in venous
pressure and relief of renal parenchymal oedema.164
The investigators of the UNLOAD trial165
compared
standard diuretic treatment with ultrafiltration in 200
patients with fluid retention caused by HF. Ultrafiltration
was safe and well tolerated, and resulted in slightly
increased fluid removal with no adverse effects on renal
function. Surprisingly, rehospitalization for HF was
reduced at 90 days, although this measure was not the
primary end point of the study.
The role of ultrafiltration in HF is not yet clear. This
treatment is effective in patients with otherwise intract
able oedema, and has some interesting effects on neuro
hormonal activation with more profound reductions in
noradrenaline, plasma renin activity, and natriuretic pep
tides than those seen with furosemide.164,166
In addition,
the ultrafiltrate contains more sodium and less potassium
than the urine of patients receiving standard diuretic
treatment,167
and ultrafiltration can be used to correct
hyponatraemia.168
However, in patients with refrac
tory fluid retention, ultrafiltration might worsen renal
function.169
The researchers in the CARESS study170,171
specifically investigated whether ultrafiltration is benefi
cial in patients with deteriorating renal function and fluid
retention, and found that creatinine levels increased
significantly with ultrafiltration compared with standard
therapy. Whether this result represents worsening renal
function or the effects of haemoconcentration is not clear.
The adverse effects of ultrafiltration on renal function
could simply suggest that the patients had end-stage
disease; more than one-third of the patients in the study
died or were readmitted at 60 days. Ultrafiltration might
be effective in less severely ill patients, might reduce the
length of hospital stay, and could have beneficial effects
on long-term outcomes. Further trials are needed to
define the role of ultrafiltration better in patients with HF.
Treatment of hyponatraemia
A decrease in serum sodium levels with diuretic treat
ment is common, and is associated with poor quality
of life and a poor prognosis.172
Hyponatraemia devel
ops when a nonosmotic stimulus to ADH production
causes water retention and dilutional hyponatraemia,
despite an overall excess of sodium in the body.173
Hyponatraemia might, therefore, simply reflect increased
neurohormonal activation.
Traditional management of hyponatraemia has been
to restrict salt and water intake, an approach that has met
with minimal success and can cause distressing thirst.
Some data are in support of the opposite approach—
infusing hypertonic saline whilst continuing diuretic
treatment (Figure 7),174
which results in a more rapid
reduction in B‑type natriuretic peptide than orthodox
management.175
Perhaps surprisingly, in light of tradi
tional understanding, a normal salt diet is associated
with a lower rate of admission for HF and of mortality,
as well as less hyponatraemia than a diet in which salt
intake is restricted.176,177
In the absence of any definitive
trial data, the low-salt diet traditionally prescribed for
patients with HF should be abandoned.
ACE inhibition might correct or provoke hypo
natraemia.178
A more logical pharmacological approach is
to use an ADH antagonist, or ‘vaptan’. Vaptans block the
effect of ADH on the renal collecting duct, which reduces
water reabsorption and increases free water clearance,
0 5 10 15
Admission days
SerumNa+(mmol/l)
20 25 50
0
135
130
125
120
115
140
30 35 40 45
Extreme fluid
restriction
No salt diet
Frusemide
infusion
(10 mg/h)
Fluid
restriction
2N* saline×1 l
Frusemide infusion (20 mg/h)
Figure 7 | Time course of serum sodium level changes in a patient presenting with
oedematous heart failure. Salt and fluid restriction, the traditional management,
resulted in further declines in serum sodium levels, which were only restored when
additional sodium was given. Abbreviation: 2N saline, 1.8% sodium chloride solution.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 11. 166 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
thereby correcting hyponatraemia.179
However, in
EVEREST, which was conducted in more than 4,000
patients admitted to hospital with HF, no survival advan
tage was found with tolvaptan.180
Interestingly, patients
who had hyponatraemia at admission had a striking
increase in serum sodium levels with tolvaptan.180
Therefore, the vaptans might have a particular role in
the treatment of patients with hyponatraemia rather than
of those with HF in general. Cardiac resynchronisation
devices can also help to correct hyponatraemia by
improvement of pump function,181
highlighting that HF
syndrome is the ultimate cause of hyponatraemia and
that hyponatraemia will resolve after HF is corrected.
Long-term management strategies
Long-term treatment of patients with HF is impor
tant. Most patients will benefit from education about
the importance of compliance with long-term medical
therapy and of avoiding an excessively high salt load.
Various strategies, ranging from nurse specialist support
to home telemonitoring systems with noninvasive or
implanted technologies, can be used to educate and
monitor patients.182
For most patients with cardiogenic oedema, recov
ery means living with a diagnosis of chronic HF.
Medical management of chronic HF can be extremely
successful, especially if HF is a result of left ventricular
systolic dysfunction.183
The opportunity to prescribe life-
prolonging (and enhancing) medication to patients (such
as β‑blockers, ACE inhibitors, and mineralocorticoid
antagonists) should not be missed.
Most patients have one or more precipitating factors
that caused or exacerbated their illness. Those with
ischaemia or with an arrhythmia should be investi
gated and treated with appropriate therapy. Common
comorbidities and opportunities for further treatment
should be sought. Atrial fibrillation is present in around
25% of patients with HF184
and requires ventricular rate
control and anticoagulation. Cardioversion might be
appropriate in selected patients with atrial fibrillation
once HF is controlled.
QRS prolongation is common in patients with left
ventricular systolic dysfunction185
and its presence
should prompt consideration of cardiac resynchronisa
tion therapy. Patients should be assessed for their suit
ability for treatment with an implantable defibrillator.
Anaemia is common, and often caused by iron deficiency
or renal dysfunction. Serum iron and transferrin satura
tion should be checked routinely if anaemia is present.
Serum ferritin levels are often falsely elevated in this
setting. However, anaemia might be dilutional, indica
ting plasma volume expansion. Treatment of oedema
could resolve anaemia. Ultimately, guidelines and other
published guidance, such as the quality standards for
HF issued by the UK National Institute for Health and
Clinical Excellence,186
will help drive up standards of care.
Conclusions
Cardiogenic oedema is a fundamental feature of HF
syndrome. High venous pressure causes fluid to transude
out of capillaries into tissue spaces faster than lymphatics
can drain the fluid away. In the pulmonary circulation, the
consequence is pulmonary oedema formation. Reducing
venous pressure is the mainstay of treatment, and new
vasodilators may have a role. New approaches using phar
maceuticals to accelerate the rate of fluid removal from
the airspaces are on the horizon. In the systemic circula
tion, the rise in venous pressure is due to fluid retention,
and treatment relies on removal of that fluid. Studies are
only now starting to explore the best strategy for diuretic
use, and the possible role of ultrafiltration.
Review criteria
A search for original articles published between 1960
and 2012 was performed in MEDLINE and PubMed
databases. The search terms used were “heart failure”,
“pulmonary oedema”, “pulmonary edema”, “oedema”
and “edema”, alone and in combination. All articles
identified were English-language, full-text papers. We
also searched the reference lists of identified articles for
further relevant papers.
1. Hospital Episode Statistics. HES online [online],
http://www.hesonline.nhs.uk/ (2012).
2. Cleland, J. G. et al. The national heart failure
audit for England and Wales 2008–2009 Heart
97, 876–86 (2011).
3. National Heart Failure Audit 2010. The NHS
Information Centre [online], http://
www.ic.nhs.uk/webfiles/publications/
002_Audits/NHS_IC_National_Heart_Failure_
Audit_2010_04-01-11.pdf (2012).
4. Michalsen, A., König, G. Thimme, W.
Preventable causative factors leading to hospital
admission with decompensated heart failure.
Heart 80, 437–441 (1998).
5. Fonarow, G. C. et al. Factors identified as
precipitating hospital admissions for heart failure
and clinical outcomes: findings from OPTIMIZE-HF.
Arch. Intern. Med. 168, 847–854 (2008).
6. Roguin, A. et al. Long-term prognosis of acute
pulmonary oedema--an ominous outcome. Eur. J.
Heart Fail. 2, 137–144 (2000).
7. Starling, E. H. On the absorption of fluids from
the connective tissue spaces. J. Physiol. 19,
312–326 (1896).
8. Erdmann, A. J. 3rd
, Vaughan, T. R. Jr,
Brigham, K. L., Woolverton, W. C. Staub, N. C.
Effect of increased vascular pressure on lung
fluid balance in unanesthetized sheep. Circ. Res.
37, 271–284 (1975).
9. Guyton, A. C. Lindsey, A. W. Effect of elevated
left atrial pressure and decreased plasma protein
concentration on the development of pulmonary
edema. Circ. Res. 7, 649–657 (1959).
10. Figueras, J. Weil, M. H. Blood volume prior to
and following treatment of acute cardiogenic
pulmonary edema. Circulation 57, 349–355
(1978).
11. Cotter, G. et al. The role of cardiac power and
systemic vascular resistance in the
pathophysiology and diagnosis of patients with
acute congestive heart failure. Eur. J. Heart Fail.
5, 443–451 (2003).
12. Pickering, T. G. et al. Recurrent pulmonary oedema
in hypertension due to bilateral renal artery
stenosis: treatment by angioplasty or surgical
revascularisation. Lancet 2, 551–552 (1988).
13. Lohmeier, T. E., Mizelle, H. L., Reinhart, G. A.
Montani, J. P. Influence of angiotensin on the
early progression of heart failure. Am. J. Physiol.
Regul.Integr.Comp.Physiol. 278, R74–R86 (2000).
14. Hall, J. E. et al. Mechanisms of escape from
sodium retention during angiotensin II
hypertension. Am. J. Physiol. 246, F627–F634
(1984).
15. van Iperen, C. E., Giezen, J., Kramer, W. L. M.,
Lips, C. J. M. Bartelink, A. K. Acute dyspnea
resulting from pulmonary oedema as the first
sign of a pheochromocytoma. Respiration 68,
323–326 (2001).
16. Sartori, C., Allemann, Y. Scherrer, U.
Pathogenesis of pulmonary edema: learning
from high-altitude pulmonary edema.
Respir. Physiol. Neurobiol. 159, 338–349 (2007).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 12. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 167
17. Fein, A. et al. The value of edema fluid protein
measurements in patients with pulmonary
edema. Am. J. Med. 67, 32–38 (1979).
18. Colombo, P. C., Onat, D. Sabbah, H. N. Acute
heart failure as “acute endothelitis”--Interaction
of fluid overload and endothelial dysfunction.
Eur. J. Heart Fail. 10, 170–175 (2008).
19. Oldenburg, O. et al. Sleep-disordered breathing
in patients with symptomatic heart failure:
a contemporary study of prevalence in and
characteristics of 700 patients. Eur. J. Heart Fail.
9, 251–257 (2007).
20. Fletcher, E. C. et al. Pulmonary edema develops
after recurrent obstructive apneas. Am. J. Respir.
Crit. Care Med. 160, 1688–1696 (1999).
21. Kasai, T. et al. Relationship between sodium
intake and sleep apnea in patients with heart
failure. J. Am. Coll. Cardiol. 58, 1970–1974
(2011).
22. Mackersie, R. C., Christensen, J. Lewis, F. R.
The role of pulmonary lymphatics in the
clearance of hydrostatic pulmonary edema.
J. Surg. Res. 43, 495–504 (1987).
23. Tandon, H. D. Kasturi, J. Pulmonary vascular
changes associated with isolated mitral
stenosis in India. Br. Heart J. 37, 26–36 (1975).
24. Davies, S. W. et al. Reduced pulmonary
microvascular permeability in severe chronic left
heart failure. Am. Heart J. 124, 137–142 (1992).
25. Huang, W. et al. Capillary filtration is reduced in
lungs adapted to chronic heart failure:
morphological and haemodynamic correlates.
Cardiovasc. Res. 49, 207–217 (2001).
26. Puri, S. et al. Reduced alveolar-capillary
membrane diffusing capacity in chronic heart
failure. Its pathophysiological relevance and
relationship to exercise performance. Circulation
91, 2769–2774 (1995).
27. Parissis, J. T. et al. Acute pulmonary oedema:
clinical characteristics, prognostic factors, and
in-hospital management. Eur. J. Heart Fail. 12,
1193–1202 (2010).
28. Zannad, F. et al. Clinical profile, contemporary
management and one-year mortality in patients
with severe acute heart failure syndromes:
The EFICA study. Eur. J. Heart Fail. 8, 697–705
(2006).
29. Mebazaa, A. et al. The impact of early standard
therapy on dyspnoea in patients with acute heart
failure: the URGENT-dyspnoea study. Eur. Heart J.
31, 832–841 (2010).
30. Dickstein, K. et al. ESC Guidelines for the
diagnosis and treatment of acute and chronic
heart failure the Task Force for the Diagnosis
and Treatment of Acute and Chronic Heart
Failure 2008 of the European Society of
Cardiology. Eur. Heart J. 29, 2388–2442 (2008).
31. Gossop, M., Keaney, F., Sharma, P. Jackson, M.
The unique role of diamorphine in British medical
practice: a survey of general practitioners and
hospital doctors. Eur. Addict. Res. 11, 76–82
(2005).
32. McMurray, J. J. et al. ESC Guidelines for the
diagnosis and treatment of acute and chronic
heart failure 2012: The Task Force for the
Diagnosis and Treatment of Acute and Chronic
Heart Failure 2012 of the European Society of
Cardiology. Developed in collaboration with the
Heart Failure Association (HFA) of the ESC.
Eur. Heart J. 33, 1787–1847 (2012).
33. Vismara, L. A., Leaman, D. M. Zelis, R.
The effects of morphine on venous tone in
patients with acute pulmonary oedema.
Circulation 54, 335–337 (1976).
34. Grossmann, M., Abiose, A., Tangphao, O.,
Blaschke, T. F. Hoffman, B. B. Morphine-induced
venodilation in humans. Clin. Pharmacol. Ther.
60, 554–560 (1996).
35. Feeney, C., Ani, C., Sharma, N. Frohlich, T.
Morphine-induced cardiogenic shock.
Ann. Pharmacother. 45, e30 (2011).
36. Sosnowski, M. A. Review article: lack of effect of
opiates in the treatment of acute cardiogenic
pulmonary oedema. Emerg. Med. Australas. 20,
384–390 (2008).
37. Peacock, W. F. et al. Morphine and outcomes in
acute decompensated heart failure: an ADHERE
analysis. Emerg. Med. J. 25, 205–209 (2008).
38. Clark, A. L., Johnson, M. J. Squire, I. Does
home oxygen benefit people with chronic heart
failure? BMJ 342, d234 (2011).
39. British Thoracic Society Standards of Care
Committee. Non-invasive ventilation in acute
respiratory failure. Thorax 57, 192–211 (2002).
40. Esteban, A., De Elió, F. J., Ancillo, P.,
Gómez‑Acebo, E. Cerdá, E. Continuous
positive pressure ventilation in the management
of eight cases of acute pulmonary oedema. Br. J.
Anaesth. 45, 1070–1074 (1973).
41. Simpson, P. M. Bendall, J. C. Prehospital
non-invasive ventilation for acute cardiogenic
pulmonary oedema: an evidence-based review.
Emerg. Med. J. 28, 609–612 (2011).
42. Peter, J. V., Moran, J. L., Phillips-Hughes, J.,
Graham, P. Bersten, A. D. Effect of non-
invasive positive pressure ventilation (NIPPV)
on mortality in patients with acute cardiogenic
pulmonary oedema: a meta-analysis. Lancet
367, 1155–1163 (2006).
43. Gray, A. et al. Noninvasive ventilation in acute
cardiogenic pulmonary edema. N. Engl. J. Med.
359, 142–151 (2008).
44. Dikshit, K. et al. Renal and extrarenal
hemodynamic effects of furosemide in
congestive heart failure after acute myocardial
infarction. N. Engl. J. Med. 288, 1087–1090
(1973).
45. Larsen, F. F. Haemodynamic effects of high or
low doses of furosemide in acute myocardial
infarction. Eur. Heart J. 9, 125–131 (1988).
46. Kiely, J., Kelly, D. T., Taylor, D. R. Pitt, B. The
role of furosemide in the treatment of left
ventricular dysfunction associated with acute
myocardial infarction. Circulation 48, 581–587
(1973).
47. Holzer-Richling, N. et al. Randomized placebo
controlled trial of furosemide on subjective
perception of dyspnoea in patients with
pulmonary oedema because of hypertensive
crisis. Eur. J. Clin. Invest. 41, 627–634 (2011).
48. Hayashi, S. Y. et al. Acute effects of low and high
intravenous doses of furosemide on myocardial
function in anuric haemodialysis patients: a
tissue Doppler study. Nephrol. Dial.Transplant.
23, 1355–1361 (2008).
49. Ikram, H., Chan, W., Espiner, E. A.
Nicholls, M. G. Haemodynamic and hormone
responses to acute and chronic frusemide
therapy in congestive heart failure. Clin. Sci. 59,
443–449 (1980).
50. Towers, K. A., Bardsley, K. A. Macdonald, P. S.
Nebulised frusemide for the symptomatic
treatment of end-stage congestive heart failure.
Med. J. Aust. 193, 555 (2010).
51. Shimoyama, N. Shimoyama, M. Nebulized
furosemide as a novel treatment for dyspnea in
terminal cancer patients. J. Pain Symptom
Manage. 23, 73–76 (2002).
52. Newton, P. J., Davidson, P. M., Krum, H.,
Ollerton, R. Macdonald, P. The acute
haemodynamic effect of nebulised frusemide in
stable, advanced heart failure. Heart Lung Circ.
21, 260–266 (2012).
53. Adams, K. F. Jr et al. Characteristics and
outcomes of patients hospitalized for heart
failure in the United States: rationale, design,
and preliminary observations from the first
100,000 cases in the Acute Decompensated
Heart Failure National Registry (ADHERE).
Am. Heart J. 149, 209–216 (2005).
54. Franciosa, J. A. Silverstein, S. R.
Hemodynamic effects of nitroprusside and
furosemide in left ventricular failure.
Clin. Pharmacol. Ther. 32, 62–69 (1982).
55. Nelson, G. I., Silke, B., Ahuja, R. C., Hussain, M.
Taylor, S. H. Haemodynamic advantages of
isosorbide dinitrate over furosamide in acute
heart failure following myocardial infarction.
Lancet 1, 730–732 (1983).
56. Beltrame, J. F. et al. Nitrate therapy is an
alternative to furosemide/morphine therapy in
the management of acute cardiogenic pulmonary
edema. J. Card. Fail. 4, 271–279 (1998).
57. Cotter, G. et al. Randomised trial of high-dose
isosorbide dinitrate plus low-dose furosemide
versus high-dose furosemide plus low-dose
isosorbide dinitrate in severe pulmonary
oedema. Lancet 351, 389–393 (1998).
58. Sharon, A. High-dose intravenous isosorbide-
dinitrate is safer and better than Bi-PAP
ventilation combined with conventional
treatment for severe pulmonary edema. J. Am.
Coll. Cardiol. 36, 832–837 (2000).
59. Hamilton, R. J., Carter, W. A. Gallagher, E. J.
Rapid improvement of acute pulmonary edema
with sublingual captopril. Acad. Emerg. Med. 3,
205–212 (1996).
60. Spieker, L. E. et al. Acute hemodynamic and
neurohumoral effects of selective ET(A) receptor
blockade in patients with congestive heart
failure. ET 003 Investigators. J. Am. Coll. Cardiol.
35, 1745–1752 (2000).
61. Kaluski, E. et al. RITZ-5: randomized intravenous
TeZosentan (an endothelin-A/B antagonist) for
the treatment of pulmonary edema: a
prospective, multicenter, double-blind, placebo-
controlled study. J. Am. Coll. Cardiol. 41,
204–210 (2003).
62. Teerlink, J. R., Massie, B. M., Cleland, J. G. F.
Tzivoni, D. for the RITZ-1 investigators. A double-
blind, parallel-group, multicenter, placebo-
controlled study to investigate the efficacy and
safety of tezosentan in reducing symptoms in
patients with acute decompensated heart failure
[abstract]. Circulation 104, II–526 (2001).
63. McMurray, J. J. et al. Effects of tezosentan on
symptoms and clinical outcomes in patients with
acute heart failure: the VERITAS randomized
controlled trials. JAMA 298, 2009–2019 (2007).
64. Kohan, D. E., Cleland, J. G., Rubin, L. J.,
Theodorescu, D. Barton, M. Clinical trials with
endothelin receptor antagonists: What went
wrong and where can we improve? Life Sci. 91,
528–539 (2012).
65. Coletta, A., Thackray, S. Nikitin, N.,
Cleland, J. G. Clinical trials update: highlights of
the scientific sessions of The American College
of Cardiology LIFE, DANAMI 2, MADIT-2,
MIRACLE-ICD, OVERTURE, OCTAVE, ENABLE 1
2, CHRISTMAS, AFFIRM, RACE, WIZARD, AZACS,
REMATCH, BNP trial and HARDBALL. Eur. J.
Heart Fail. 4, 381–388 (2002).
66. Mills, R. M. et al. Sustained hemodynamic
effects of an infusion of nesiritide (human b-type
natriuretic peptide) in heart failure: a
randomized, double-blind, placebo-controlled
clinical trial. Natrecor Study Group. J. Am.
Coll. Cardiol. 34, 155–162 (1999).
67. Publication Committee for the VMAC
Investigators (Vasodilatation in the Management
of Acute CHF). Intravenous nesiritide vs
nitroglycerin for treatment of decompensated
congestive heart failure: a randomized controlled
trial. JAMA 287, 1531–1540 (2002).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 13. 168 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
68. O’Connor, C. M. et al. Effect of nesiritide in
patients with acute decompensated heart
failure. N. Engl. J. Med. 365, 32–43 (2011).
69. Ando, S., Imaizumi, T., Harada, S., Hirooka, Y.
Takeshita, A. Atrial natriuretic peptide
increases human capillary filtration and
venous distensibility. J. Hypertens. 10, 451–457
(1992).
70. Chen, W. et al. Atrial natriuretic peptide
enhances microvascular albumin permeability
by the caveolae-mediated transcellular pathway.
Cardiovasc. Res. 93, 141–151 (2012).
71. Debrah, D. O., Conrad, K. P., Jeyabalan, A.,
Danielson, L. A. Shroff, S. G. Relaxin
increases cardiac output and reduces systemic
arterial load in hypertensive rats. Hypertension
46, 745–750 (2005).
72. Teerlink, J. R. et al. Relaxin for the treatment
of patients with acute heart failure
(Pre‑RELAX‑AHF): a multicentre, randomised,
placebo-controlled, parallel-group, dose-finding
phase IIb study. Lancet 373, 1429–1439
(2009).
73. Teerlink, J. R. et al. Serelaxin, recombinant
human relaxin-2, for treatment of acute heart
failure (RELAX-AHF): a randomised,
placebo-controlled trial. Lancet http://
dx.doi.org/10.1016/S0140-6736(12)61855-8.
74. US National Library of Medicine. ClinicalTrials.gov
[online], http://clinicaltrials.gov/ct2/show/
NCT00803634 (2012).
75. Sartori, C., Matthay, M. A. Scherrer, U.
Transepithelial sodium and water transport in
the lung. Major player and novel therapeutic
target in pulmonary edema. Adv. Exp. Med. Biol.
502, 315–338 (2001).
76. Matthay, M. A., Folkesson, H. G. Clerici, C.
Lung epithelial fluid transport and the resolution
of pulmonary edema. Physiol. Rev. 82, 569–600
(2002).
77. Mutlu, G. M. et al. Upregulation of alveolar
epithelial active Na+
transport is dependent on
beta2-adrenergic receptor signaling. Circ. Res.
94, 1091–1100 (2004).
78. Mutlu, G. M. Factor, P. Alveolar epithelial
beta2-adrenergic receptors. Am. J. Respir. Cell.
Mol. Biol. 38, 127–134 (2008).
79. Maak, C. A., Tabas, J. A. McClintock, D. E.
Should acute treatment with inhaled beta
agonists be withheld from patients with dyspnea
who may have heart failure? J. Emerg. Med. 40,
135–145 (2011).
80. Thorneloe, K. S. et al. An orally active TRPV4
channel blocker prevents and resolves
pulmonary edema in heart failure. Sci.Transl.
Med. 4, 159ra148 (2012).
81. Gheorghiade, M. et al. Cinaciguat, a soluble
guanylate cyclase activator: results from the
randomized, controlled, phase IIb COMPOSE
programme in acute heart failure syndromes.
Eur. J. Heart Fail. 14, 1056–1066 (2012).
82. Benz, K. et al. Blood pressure-independent effect
of long-term treatment with the soluble
heme-independent guanylyl cyclase activator
HMR1766 on progression in a model of
noninflammatory chronic renal damage.
Kidney Blood Press. Res. 30, 224–233 (2007).
83. Jones, E. S., Kemp-Harper, B., Stasch, J. P.,
Schmidt, H. Widdop, R. E. Cardioprotective
effects in aged spontaneously hypertensive rats
due to chronic stimulation/activation of sGC
without hypotension. BMC Pharmacol.
9 (Suppl. 1), P29 (2009).
84. Capomolla, S. et al. Chronic infusion of
dobutamine and nitroprusside in patients with
end-stage heart failure awaiting heart
transplantation: safety and clinical outcome.
Eur. J. Heart Fail. 3, 601–610 (2001).
85. Thackray, S., Easthaugh, J., Freemantle, N.
Cleland, J. G. The effectiveness and relative
effectiveness of intravenous inotropic drugs
acting through the adrenergic pathway in
patients with heart failure-a meta-regression
analysis. Eur. J. Heart Fail. 4, 515–529 (2002).
86. Follath, F. et al. Efficacy and safety of intravenous
levosimendan compared with dobutamine in
severe low-output heart failure (the LIDO study):
a randomised double-blind trial. Lancet 360,
196–202 (2002).
87. Mebazaa, A. et al. Levosimendan vs dobutamine
for patients with acute decompensated heart
failure: the SURVIVE Randomized Trial. JAMA
297, 1883–1891 (2007).
88. Landoni, G. et al. Effects of levosimendan on
mortality and hospitalization. A meta-analysis of
randomized controlled studies. Crit. Care Med.
40, 634–646 (2012).
89. Bragadeesh, T. K., Mathur, G., Clark, A. L.
Cleland, J. G. Novel cardiac myosin activators for
acute heart failure. Expert Opin. Investig. Drugs
16, 1541–1548 (2007).
90. Cleland, J. G. et al. The effects of the cardiac
myosin activator, omecamtiv mecarbil, on
cardiac function in systolic heart failure: a
double-blind, placebo-controlled, crossover,
dose-ranging phase 2 trial. Lancet 378,
676–683 (2011).
91. US National Library of Medicine. ClinicalTrials.gov
[online], http://clinicaltrials.gov/ct2/show/
NCT01300013 (2012).
92. Gheorghiade, M. et al. Hemodynamic,
echocardiographic, and neurohormonal effects
of istaroxime, a novel intravenous inotropic and
lusitropic agent: a randomized controlled trial in
patients hospitalized with heart failure. J. Am.
Coll. Cardiol. 51, 2276–2285 (2008).
93. Shah, S. J. et al. Effects of istaroxime on
diastolic stiffness in acute heart failure
syndromes: results from the Hemodynamic,
Echocardiographic, and Neurohormonal Effects
of Istaroxime, a Novel Intravenous Inotropic and
Lusitropic Agent: a Randomized Controlled Trial
in Patients Hospitalized with Heart Failure
(HORIZON-HF) trial. Am. Heart J. 157,
1035–1041 (2009).
94. Thiele, H. et al. Intraaortic balloon
counterpulsation in acute myocardial infarction
complicated by cardiogenic shock: design and
rationale of the Intraaortic Balloon Pump in
Cardiogenic Shock II (IABP-SHOCK II) trial.
Am. Heart J. 163, 938–945 (2012).
95. Thiele, H. et al. Intraaortic balloon support for
myocardial infarction with cardiogenic shock.
N. Engl. J. Med. 163, 938–945 (2012).
96. Engström, A. E. et al. The Impella 2.5 and 5.0
devices for ST-elevation myocardial infarction
patients presenting with severe and profound
cardiogenic shock: the Academic Medical Center
intensive care unit experience. Crit. Care Med.
39, 2072–2079 (2011).
97. Stack, R. S., Stack, R. K., Morris, K. G.,
Bauman, R. P. Shadoff, N. Temporary balloon
occlusion of the inferior vena cava for immediate
reversal of acute pulmonary edema. Am. J.
Cardiol. 57, 886–887 (1986).
98. Warner, G. F., Dobson, E. L., Rodgers, C. E.,
Johnston, M. E. Pace, N. The measurement of
total “sodium space” and total body sodium in
normal individuals and in patients with cardiac
edema. Circulation 5, 915–919 (1952).
99. Cleland, J. G., Dargie, H. J., Robertson, I.,
Robertson, J. I. East, B. W. Total body
electrolyte composition in patients with heart
failure: a comparison with normal subjects and
patients with untreated hypertension. Br. Heart J.
58, 230–238 (1987).
100. Anand, I. S. et al. Edema of cardiac origin.
Studies of body water and sodium, renal
function, hemodynamic indexes, and plasma
hormones in untreated congestive cardiac
failure. Circulation 80, 299–305 (1989).
101. Harris, P. Evolution and the cardiac patient.
Cardiovasc. Res. 17, 313–319, 373–378,
437–345 (1983).
102. Franklin, S. S., et al. Hemodynamic patterns
of age-related changes in blood pressure.
The Framingham Heart Study. Circulation 96,
308–315 (1997).
103. Merrill, A. J. Edema and decreased renal blood
flow in patients with chronic congestive heart
failure: evidence of “forward failure” as primary
cause of edema. J. Clin. Invest. 25, 389–400
(1946).
104. Skinner, S. L., McCubbin, J. W. Page, I. H.
Control of renin secretion. Circ. Res. 15, 64–76
(1964).
105. Farhi, E. R., Cant, J. R. Barger, A. C. Interactions
between intrarenal epinephrine receptors and the
renal baroreceptor in the control of PRA in
conscious dogs. Circ. Res. 50, 477–485 (1982).
106. Knepper, M. A. Molecular physiology of urinary
concentrating mechanism: regulation of
aquaporin water channels by vasopressin. Am. J.
Physiol. Renal Physiol. 41, F3–F12 (1997).
107. Bonjour, J. P. Malvin, R. L. Stimulation of ADH
release by the renin-angiotensin system. Am. J.
Physiol. 218, 1555–1559 (1970).
108. Szatalowicz, V. L. et al. Radioimmunoassay of
plasma arginine vasopressin in hyponatremic
patients with congestive heart failure. N. Engl.
J. Med. 305, 263–266 (1981).
109. Francis, G. S. et al. Comparison of
neuroendocrine activation in patients with left
ventricular dysfunction with and without
congestive heart failure. A substudy of the
Studies of Left Ventricular Dysfunction (SOLVD).
Circulation 82, 1724–1729.
110. Robertson, G. L. Regulation of arginine
vasopressin in the syndrome of inappropriate
antidiuresis. Am. J. Med. 119 (Suppl. 1),
S36–S42 (2006).
111. Nordgren, L. Sörensen, S. Symptoms
experienced in the last six months of life in
patients with end-stage heart failure. Eur. J.
Cardiovasc. Nurs. 2, 213–217 (2003).
112. Falk, S., Wahn, A.‑K. Lidell, E. Keeping the
maintenance of daily life in spite of chronic heart
failure. A qualitative study. Eur. J.
Cardiovasc. Nurs. 6, 192–199 (2007).
113. Waldréus, N., Sjöstrand, F. Hahn, R. G. Thirst
in the elderly with and without heart failure.
Arch. Gerontol. Geriatr. 53, 174–178 (2011).
114. Farrell, M. J. et al. Effect of aging on regional
cerebral blood flow responses associated with
osmotic thirst and its satiation by water drinking:
a PET study. Proc. Natl Acad. Sci. USA 105,
382–387 (2008).
115. Ramsay, D. J., Rolls, B. J. Wood, R. J. The
relationship between elevated water intake and
oedema associated with congestive cardiac
failure in the dog. J. Physiol. 244, 303–312
(1975).
116. Johnson, A. K., Mann, J. F., Rascher, W.,
Johnson, J. K. Ganten, D. Plasma angiotensin II
concentrations and experimentally induced thirst.
Am. J. Physiol. 240, R229–R234 (1981).
117. Szczepanska‑Sadowska, E., Sobocinska, J.
Sadowski, B. Central dipsogenic effect of
vasopressin. Am. J. Physiol. 242, R372–R379
(1982).
118. Travers, B. et al. Fluid restriction in the
management of decompensated heart failure:
no impact on time to clinical stability. J. Card.
Fail. 13, 128–132 (2007).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 14. NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 169
119. Holst, M., Strömberg, A., Lindholm, M.
Willenheimer, R. Liberal versus restricted fluid
prescription in stabilised patients with chronic
heart failure: result of a randomised cross-over
study of the effects on health-related quality of
life, physical capacity, thirst and morbidity.
Scand. Cardiovasc. J. 42, 316–322 (2008).
120. Abildgaard, U. et al. Bed rest and increased
diuretic treatment in chronic congestive heart
failure. Eur. Heart J. 6, 1040–1046 (1985).
121. McDonald, C. D., Burch, G. E. Walsh, J. J.
Prolonged bed rest in the treatment of idiopathic
cardiomyopathy. Am. J. Med. 52, 41–50 (1972).
122. Flapan, A. D. et al. The influence of posture on
the response to loop diuretics in patients with
chronic cardiac failure is reduced by angiotensin
converting enzyme inhibition. Eur. J.
Clin. Pharmacol. 42, 581–585 (1992).
123. Miller, W. L., Bailey, K. R., Weston, S. A.,
Burnett, J. C. Jr Rodeheffer, R. J.
Hemodynamic and plasma atrial natriuretic
peptide responses to acute digitalis therapy in
patients with normal and impaired left ventricular
function. Eur. J. Heart Fail. 4, 63–72 (2002).
124. CLOTS (Clots in Legs Or sTockings after Stroke)
Trial Collaboration. Thigh-length versus below-
knee stockings for deep venous thrombosis
prophylaxis after stroke: a randomized trial.
Ann. Intern. Med. 153, 553–562 (2010).
125. de Silva, R. Incidence of renal dysfunction over 6
months in patients with chronic heart failure due
to left ventricular systolic dysfunction:
contributing factors and relationship to
prognosis. Eur. Heart J. 27, 569–581 (2006).
126. Maxwell, A. P., Ong, H. Y. Nicholls, D. P.
Influence of progressive renal dysfunction in
chronic heart failure. Eur. J. Heart Fail. 4,
125–130 (2002).
127. Cleland, J. G. et al. Renal dysfunction in acute
and chronic heart failure: prevalence, incidence
and prognosis. Heart Fail. Rev. 17, 133–149
(2012).
128. Harjola, V. P. et al. Characteristics, outcomes,
and predictors of mortality at 3 months and
1 year in patients hospitalized for acute heart
failure. Eur. J. Heart Fail. 12, 239–248 (2010).
129. Elkayam, U. et al. Renal circulatory effects of
adenosine in patients with chronic heart failure.
J. Am. Coll. Cardiol. 32, 211–215 (1998).
130. Massie, B. M. et al. Rolofylline, an adenosine
A1-receptor antagonist, in acute heart failure.
N. Engl. J. Med. 363, 1419–1428 (2010).
131. Dormans, T. P., Gerlag, P. G., Russel, F. G.
Smits, P. Combination diuretic therapy in
severe congestive heart failure. Drugs 2,
165–172 (1998).
132. Brater, D. C. Pharmacology of diuretics. Am. J.
Med. Sci. 319, 38–50 (2000).
133. Pothuizen, L. M. Chada, D. R. Treatment of
congestive cardiac failure in elderly patients:
randomised study of hydrochlorothiazide and
slow release furosemide. Curr. Ther. Res. 32,
513–519 (1982).
134. Vermeulen, A. Chada, D. R. Slow-release
furosemide and hydrochlorothiazide in
congestive cardiac failure: A controlled trial.
J. Clin. Pharmacol. 22, 513–519 (1982).
135. Krause, U., Zielke, A., Schmidt-Gayk, H.,
Ehrenthal, W. Beyer, J. Direct tubular effect on
calcium retention by hydrochlorothiazide.
J. Endocrinol. Invest. 12, 531–535 (1989).
136. Solomon, D. H., Mogun, H., Garneau, K.
Fischer, M. A. Risk of fractures in older adults
using antihypertensive medications. J. Bone
Miner. Res. 26, 1561–1567 (2011).
137. Dargie, H. J., Allison, M. E., Kennedy, A. C.
Gray, M. H. High dose metolazone in chronic
renal failure. Br. Med. J. 4, 196–198 (1972).
138. Kohvakka, A. Maintenance of potassium balance
during long-term diuretic therapy in chronic heart
failure patients with thiazide induced
hypokalemia: comparison of potassium
supplementation with potassium chloride and
potassium-sparing agents, amiloride and
triamterene. Int. J. Clin. Pharmacol. Ther. Toxicol.
26, 273–277 (1988).
139. Pitt, B. et al. The effect of spironolactone on
morbidity and mortality in patients with severe
heart failure. Randomized Aldactone Evaluation
Study Investigators. N. Engl. J. Med. 341,
709–717 (1999).
140. Zannad, F. et al. Eplerenone in patients with
systolic heart failure and mild symptoms.
N. Engl. J. Med. 364, 11–21 (2011).
141. Stewart, J. H. Edwards, K. D. G. Clinical
comparison of frusemide with bendrofluazide,
mersalyl and ethacrynic acid. Br. Med. J. 2,
1277–1281 (1965).
142. Kaissling, B. Stanton, B. A. Adaptation of
distal tubule and collecting duct to increased
sodium delivery: I Ultrastructure. Am. J. Physiol.
255, F1256–F1275 (1988).
143. Stanton, B. A. Kaissling, B. Adaptation of
distal tubule and collecting duct to increased Na
delivery. II. Na and K transport. Am. J. Physiol.
255, 1269–1275 (1988).
144. Murray, M. D., Haag, K. M., Black, P. K., Hall, S. D.
Brater, D. C. Variable furosemide absorption
and poor predictability of response in elderly
patients. Pharmacother. 17, 98–106 (1997).
145. Vasko, M. R., Cartwright, D. B., Knochel, J. P.
Nixon, J. V. Brater, D. C. Furosemide
absorption altered in decompensated
congestive heart failure. Ann. Intern. Med. 102,
314–318 (1985).
146. van Meyel, J. J. et al. Continuous infusion of
furosemide in the treatment of patients with
congestive heart failure and diuretic resistance.
J. Intern. Med. 235, 329–334 (1994).
147. Dormans, T. P. et al. Diuretic efficacy of high dose
furosemide in severe heart failure: bolus versus
continuous infusion. J. Am. Coll. Cardiol. 28,
376–382 (1996).
148. Lahav, M., Regev, A., Ra’anani, P. Theodor, E.
Intermittent administration of furosemide vs
continuous infusion preceded by a loading dose
for congestive heart failure. Chest 102,
725–731 (1992).
149. Pivac, N. et al. Diuretic effects of furosemide
infusion versus bolus injection in congestive
heart failure. Int. J. Clin. Pharmacol. Res. 18,
121–128 (1998).
150. Paterna, S. et al. Effects of high dose furosemide
and small volume hypertonic saline solution
infusion in comparison with a high dose of
furosemide as a bolus, in refractory congestive
heart failure. Eur. J. Heart Fail. 2, 305–313
(2000).
151. Rudy, D. W., Voelker, J. R., Greene, P. K.,
Esparza, F. A. Brater, D. C. Loop diuretics for
renal insufficiency: a continuous infusion is
more efficacious than bolus therapy. Ann. Intern.
Med. 115, 360–366 (1991).
152. Felker, G. M. et al. Diuretic strategies in patients
with acute decompensated heart failure. N. Engl.
J. Med. 364, 797–805 (2011).
153. Sigured, B., Olesen, K. H. Wennevold, A.
The supra-additive natriuretic effect of addition
of bendroflumethiazide and bumetanide in
congestive heart failure. Am. Heart J. 89,
163–170 (1975).
154. Channer, K. S., McLean, K. A.,
Lawson‑Matthew, P. Richardson, M.
Combination diuretic treatment in severe heart
failure: a randomised controlled trial. Br. Heart J.
71, 146–150 (1994).
155. Bartoli, E. et al. Blunting of furosemide diuresis
by aspirin in man. J. Clin. Pharmacol. 20,
452–458 (1980).
156. Jondeau, G. et al. B-CONVINCED: Beta-blocker
CONtinuation Vs. INterruption in patients with
Congestive heart failure hospitalizED for a
decompensation episode. Eur. Heart J. 30,
2186–2192 (2009).
157. Metra, M. et al. Should beta-blocker therapy be
reduced or withdrawn after an episode of
decompensated heart failure? Results from
COMET. Eur. J. Heart Fail. 9, 901–909 (2007).
158. [No authors listed] The effect of digoxin on
mortality and morbidity in patients with heart
failure. The Digitalis Investigation Group. N. Engl.
J. Med. 336, 525–533 (1997).
159. Gavey, C. J. Parkinson, J. Digitalis in heart
failure with normal rhythm. Br. Heart J. 1, 27–44
(1939).
160. Ahmed, A. et al. Digoxin and reduction in
mortality and hospitalization in heart failure:
a comprehensive post hoc analysis of the
DIG trial. Eur. Heart J. 27, 178–186 (2006).
161. Kolff, W. J. Leonards, J. R. Reduction of
otherwise intractable edema by dialysis or
filtration. Cleveland Clin. Q. 21, 61–71 (1954).
162. Marenzi, G. et al. Circulatory response to fluid
overload removal by extracorporeal ultrafiltration
in refractory congestive heart failure. J. Am.
Coll. Cardiol. 38, 963–968 (2001).
163. Bart, B. A. et al. Ultrafiltration versus usual care
for hospitalized patients with heart failure: the
Relief for Acutely Fluid-Overloaded Patients With
Decompensated Congestive Heart Failure
(RAPID-CHF) trial. J. Am. Coll. Cardiol. 46,
2043–2046 (2005).
164. Libetta, C. et al. Intermittent haemodiafiltration
in refractory congestive heart failure: BNP and
balance of inflammatory cytokines. Nephrol. Dial.
Transplant. 22, 2013–2019 (2007).
165. Costanzo, M. R. et al. Ultrafiltration versus
intravenous diuretics for patients hospitalized
for acute decompensated heart failure. J. Am.
Coll. Cardiol. 49, 675–683 (Erratum. J. Am. Coll.
Cardiol. 49, 1136 [2007]).
166. Agostoni, P. et al. Sustained improvement in
functional capacity after removal of body fluid
with isolated ultrafiltration in chronic cardiac
insufficiency: failure of furosemide to provide
the same result. Am. J. Med. 96, 191–199
(1994).
167. Ali, S. S. et al. Loop diuretics can cause clinical
natriuretic failure: a prescription for volume
expansion. Congest. Heart Fail. 15, 1–4
(2009).
168. Costanzo, M. R., Saltzberg, M., O’Sullivan, J.
Sobotka, P. Early ultrafiltration in patients with
decompensated heart failure and diuretic
resistance. J. Am. Coll. Cardiol. 46, 2047–2051
(2005).
169. Patarroyo, M. et al. Cardiorenal outcomes after
slow continuous ultrafiltration therapy in
refractory patients with advanced
decompensated heart failure. J. Am. Coll.
Cardiol. 60, 1906–1912 (2012).
170. Bart, B. A. et al. Cardiorenal rescue study in
acute decompensated heart failure: rationale
and design of CARRESS-HF, for the Heart Failure
Clinical Research Network. J. Card. Fail. 18,
176–182 (2012).
171. Bart, B. A. et al. Ultrafiltration in decompensated
heart failure with cardiorenal syndrome. N. Engl.
J. Med. 367, 2296–2304 (2012).
172. Lee, W. H. Packer, M. Prognostic importance of
serum sodium concentration and its
modification by converting-enzyme inhibition in
patients with severe chronic heart failure.
Circulation 73, 257–267 (1986).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
- 15. 170 | MARCH 2013 | VOLUME 10 www.nature.com/nrcardio
173. Francis, G. S. et al. Comparison of
neuroendocrine activation in patients with left
ventricular dysfunction with and without
congestive heart failure. A substudy of the
Studies of Left Ventricular Dysfunction (SOLVD).
Circulation 82, 1724–1729 (1990).
174. Licata, G. et al. Effects of high-dose furosemide
and small-volume hypertonic saline solution
infusion in comparison with a high dose of
furosemide as bolus in refractory congestive
heart failure: long-term effects. Am. Heart J.
145, 459–466 (2003).
175. Paterna, S. et al. Changes in brain natriuretic
peptide levels and bioelectrical impedance
measurements after treatment with high-dose
furosemide and hypertonic saline solution
versus high-dose furosemide alone in refractory
congestive heart failure: a double-blind study.
J. Am. Coll. Cardiol. 45, 1997–2003 (2005).
176. Paterna, S., Gaspare, P., Fasullo, S.,
Sarullo, F. M. Di Pasquale, P. Normal-sodium
diet compared with low-sodium diet in
compensated congestive heart failure: is
sodium an old enemy or a new friend? Clin. Sci.
(Lond.) 114, 221–230 (2008).
177. Dinicolantonio, J. J., Pasquale, P. D.,
Taylor, R. S. Hackam, D. G. Low sodium
versus normal sodium diets in systolic heart
failure: systematic review and meta-analysis.
Heart http://dx.doi.org/10.1136/
heartjnl-2012-302337.
178. Packer, M., Medina, N. Yushak, M. Correction
of dilutional hyponatremia in severe chronic
heart failure by converting-enzyme inhibition.
Ann. Intern. Med. 100, 782–789 (1984).
179. Gheorghiade, M. et al. Vasopressin V2-receptor
blockade with tolvaptan in patients with chronic
heart failure: results from a double-blind,
randomized trial. Circulation 107, 2690–2696
(2003).
180. Konstam, M. A. et al. Effects of oral tolvaptan in
patients hospitalized for worsening heart failure:
the EVEREST Outcome Trial. JAMA 297,
1319–1331 (2007).
181. Cowburn, P. J., Patel, H., Jolliffe, R. E.,
Wald, R. W. Parker, J. D. Cardiac
resynchronization therapy: an option for inotrope-
supported patients with end-stage heart failure?
Eur. J. Heart Fail. 7, 215–217 (2005).
182. Anker, S. D., Koehler, F. Abraham, W. T.
Telemedicine and remote management of
patients with heart failure. Lancet 378,
731–739 (2011).
183. Cleland, J. G. Clark, A. L. Delivering the
cumulative benefits of triple therapy to improve
outcomes in heart failure: too many cooks will
spoil the broth. J. Am. Coll. Cardiol. 42,
1234–1237 (2003).
184. Shelton, R. J., Clark, A. L., Kaye, G. C.
Cleland, J. G. The atrial fibrillation paradox of
heart failure. Congest. Heart Fail. 16, 3–9 (2010).
185. Clark, A. L., Goode, K. Cleland, J. G. The
prevalence and incidence of left bundle branch
block in ambulant patients with chronic heart
failure. Eur. J. Heart Fail. 10, 696–702 (2008).
186. QS9 Quality heart failure quality standard.
National Institute for Health and Clinical
Excellence [online], http://publications.nice.org.
uk/chronic-heart-failure-quality-standard-qs9
(2012).
187. Voors, A. A. et al. Effects of the adenosine A1
receptor antagonist rolofylline on renal function
in patients with acute heart failure and renal
dysfunction: results from PROTECT (Placebo-
Controlled Randomized Study of the Selective
Adenosine A1 Receptor Antagonist Rolofylline
for Patients Hospitalized with Acute
Decompensated Heart Failure and Volume
Overload to Assess Treatment Effect on
Congestion and Renal Function). J.Am.
Coll. Cardiol. 57, 1899-1907 (2011).
Author contributions
Both authors researched data for article, and made
substantial contribution to discussion of content and
to reviewing and editing of manuscript before
submission. A. L. Clark wrote the article.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

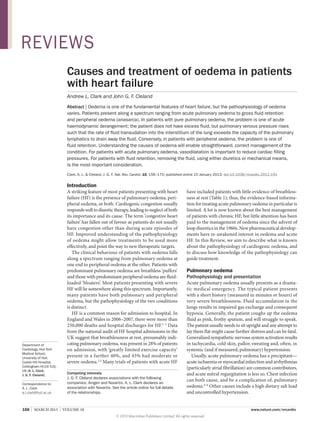
![NATURE REVIEWS | CARDIOLOGY VOLUME 10 | MARCH 2013 | 157
The pathophysiology of acute pulmonary oedema is
best understood as a haemodynamic phenomenon. In
the normal circulation, the Frank–Starling mechanism
holds: As the load on the left ventricle increases prior to
theonsetofsystole,sodoestheworkoftheheartduringthe
subsequent contraction (Figure 1). The preload is equiva
lent to the end-diastolic (or filling) pressure in the left
ventricle, and is the same as the left atrial pressure and
pulmonary venous pressure at the end of diastole (in the
absence of mitral valve stenosis).
Another relationship described by Starling explains the
net flow of fluid across a capillary in terms of the forces
acting across the capillary wall.7
Although the balance of
forces changes along the length of the capillary, the major
factor causing the fluid to move out of the capillary is
the difference between the hydrostatic pressure within the
capillary and the lower pressure in the surrounding
interstitial fluid. Opposing this movement is the colloid
osmotic pressure within the capillary, which is mainly
provided by albumin. The colloid osmotic pressure is
higher than the osmotic pressure in the interstitium and
thus tends to keep the fluid in the capillary. A protec
tive mechanism is provided by lymphatic wash-out
of any albumin that reaches the interstitium, result
ing in an increase in the osmotic pressure gradient
between the capillary and the interstitium, which seems
to reduce transudation of fluid.8
In addition, some
resistance to transudation of fluid is provided by the
alveolar–capillary basement membrane.
In the normal circulation, fluid is continuously
transuded from the capillaries into the interstit
ium, and fluid crossing into the interstitial space
is removed by the lymphatic system. The pulmo
nary capillary wall is relatively impervious to fluid,
and the tight apposition of the pulmonary capil
lary and alveolar membranes (the alveolar–capillary
basement membrane) enables efficient gas transfer.
Even if fluid escapes from the capillaries into the
interstitium, provided that it does not spill over into
the alveoli, lymphatic drainage will clear the fluid and the
patient is unlikely to experience breathlessness at rest.
In the failing left ventricle, the curve relating the end-
diastolic pressure to left ventricular work moves down
and to the right. The filling pressure (preload) in the
left ventricle required to deliver a given amount of work
increases. As the left ventricular filling pressure rises,
so does the pressure in the left atrium and pulmonary
capillaries. As hydrostatic pressure increases, capillary
wall tension increases as the fourth power of the radius of
the capillaries, increasing the rate of transmural filtration.
At the same time, lymphatic drainage into the systemic
veins could be impeded by increases in systemic venous
pressure. Eventually, a tipping point is reached when the
capacity of the lymphatic system to remove fluid from
the interstitium is exceeded, and fluid starts to accumulate
in the airspaces of the lungs (alveolar oedema).
Elegant experiments in dogs have demonstrated the
presence of such a critical tipping point. Beyond
the threshold, there is a near-linear relation between the
increase in left atrial pressure and the rate of oedema
formation (Figure 2).9
A reduction in plasma protein
levels reduces the threshold at which oedema starts to
accumulate. Notably, in acute pulmonary oedema the
total amount of fluid in the body does not increase and
the effect of impaired cardiac function leading to haemo
dynamic changes results in fluid moving to the ‘wrong’
body compartment. Indeed, some evidence suggests that
the fluid extravasation into the alveoli results in a reduc
tion in blood volume during acute pulmonary oedema,
which then increases back to normal levels during
successful treatment.10
Key points
■■ Oedema is one of the fundamental features of heart failure
■■ Clinical trial data to guide best practice in managing cardiac oedema are lacking
■■ Acute pulmonary oedema is characterized by accumulation of fluid in the air
spaces, not by fluid overload
■■ Acute pulmonary oedema is best treated as a haemodynamic problem
using vasodilators
■■ Peripheral oedema is characterized by an excess of total body water
■■ Peripheral oedema is best treated by removing fluid, either with diuretics
or mechanically
Table 1 | Trials of patients with acute heart failure
Study
name
Intervention Mode
of action
Mean
patient
age
(years)
Women
(%)
Systolic
blood
pressure
(mmHg)
Heart
rate
(per
min)
Respiratory
rate
(per min)*
LVEF
(%)*
β-blocker
use (%)
Digoxin
use (%)
Time
to study
inclusion
30-day
mortality
(%)
VERITAS63
Tezosentan Endothelin
antagonist
70 40 131 81 26 [24] 29
[40]
48 21 24 h 4
SURVIVE87
Levosimendan Calcium
sensitizer
67 28 116 84 NR 24
[30]
51 NR NR 13
EVEREST180
Tolvaptan Vasopressin
antagonist
66 26 120 80 NR 28
[40]
70 46 48 h 5
ASCEND68
Nesiritide Natriuretic
peptide
67 34 124 82 23 40
in 81
NR NR 48 h 4
PROTECT187
Rolofylline Adenosine
antagonist
70 33 124 80 21 32
[any]
76 28 24 h 15
3CPO43‡
C-PAP NA 78 57 161 114 33 [20] NR NR NR NR 16
*Numbers in square brackets denote the upper limit permitted by the trial design. ‡
3CPO trial included ‘puffers’; the other trials included ‘bloaters’. Abbreviations: C‑PAP, continuous positive
airways pressure; LVEF, left ventricular ejection fraction; NA, not applicable; NR, not reported.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)