Diferenças de Crescer Fetal -Pós Fetal: Criança Infantil Hormônio: GH Classico;Crescer Fetal
•Als DOCX, PDF herunterladen•
0 gefällt mir•418 views

A deficiência do hormônio tireoidiano não afeta diretamente o peso de nascimento, porém uma gestação prolongada pode ser um achado do hipotireoidismo congênito, bebês nascidos com hipotireoidismo congênito podem mostrar nenhum efeito, ou podem exibir efeitos leves que muitas vezes passam despercebidos como um problema: sono excessivo, redução tônus muscular, choro baixo ou rouco, evacuações frequentes, exagerada icterícia e baixa temperatura do cor

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie Diferenças de Crescer Fetal -Pós Fetal: Criança Infantil Hormônio: GH Classico;Crescer Fetal
Ähnlich wie Diferenças de Crescer Fetal -Pós Fetal: Criança Infantil Hormônio: GH Classico;Crescer Fetal (20)
Mehr von Van Der Häägen Brazil
Mehr von Van Der Häägen Brazil (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (7)
Diferenças de Crescer Fetal -Pós Fetal: Criança Infantil Hormônio: GH Classico;Crescer Fetal
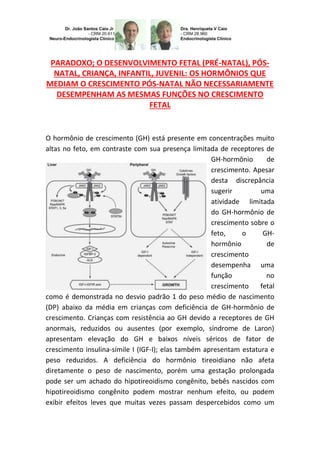
- 1. PARADOXO; O DESENVOLVIMENTO FETAL (PRÉ-NATAL), PÓS- NATAL, CRIANÇA, INFANTIL, JUVENIL: OS HORMÔNIOS QUE MEDIAM O CRESCIMENTO PÓS-NATAL NÃO NECESSARIAMENTE DESEMPENHAM AS MESMAS FUNÇÕES NO CRESCIMENTO FETAL O hormônio de crescimento (GH) está presente em concentrações muito altas no feto, em contraste com sua presença limitada de receptores de GH-hormônio de crescimento. Apesar desta discrepância sugerir uma atividade limitada do GH-hormônio de crescimento sobre o feto, o GH- hormônio de crescimento desempenha uma função no crescimento fetal como é demonstrada no desvio padrão 1 do peso médio de nascimento (DP) abaixo da média em crianças com deficiência de GH-hormônio de crescimento. Crianças com resistência ao GH devido a receptores de GH anormais, reduzidos ou ausentes (por exemplo, síndrome de Laron) apresentam elevação do GH e baixos níveis séricos de fator de crescimento insulina-símile I (IGF-I); elas também apresentam estatura e peso reduzidos. A deficiência do hormônio tireoidiano não afeta diretamente o peso de nascimento, porém uma gestação prolongada pode ser um achado do hipotireoidismo congênito, bebês nascidos com hipotireoidismo congênito podem mostrar nenhum efeito, ou podem exibir efeitos leves que muitas vezes passam despercebidos como um
- 2. problema: sono excessivo, redução tônus muscular, choro baixo ou rouco, evacuações frequentes, exagerada icterícia e baixa temperatura do corpo. Se a deficiência fetal for grave por causa da ausência completa (athyreosis) da glândula, características físicas podem incluir uma maior fontanela anterior e a persistência de uma fontanela posterior, uma hérnia umbilical, e uma grande língua (macroglossia). Na época antes de triagem neonatal, menos da metade dos casos de hipotireoidismo grave foram reconhecidos no primeiro mês de vida. À medida que os meses passaram esses bebês mal cresciam e apresentavam atraso em seu desenvolvimento. Por vários anos de idade, iriam apresentar as características faciais e corporais reconhecíveis de cretinismo. Persistência de grave hipotireoidismo, sem tratamento adequado resultava em deficiência mental grave, com um QI abaixo de 80, na maioria das vezes. A maioria destas crianças acabou chegando a cuidados institucionais. O hipotireoidismo congênito (HC) é uma condição da deficiência do hormônio da tireóide presente no nascimento. Cerca de 1 em 4.000 recém-nascidos tem uma deficiência grave da função da tireóide, enquanto ainda mais têm graus leves ou um hipotireoidismo parcial. Se não for tratado por vários meses após o nascimento, o hipotireoidismo congênito grave pode levar à insuficiência do crescimento com baixa estatura intra-útero, neonatal, criança, infantil, juvenil, adolescente e lamentavelmente repercutirá no adulto principalmente sem tratamento adequado. Esta situação é perene e irreversível depois de instalada com suas sequelas e dentre elas temos a permanente deficiência intelectual. O lactogênio placentário não exerce efeito sobre o tamanho
- 3. do recém-nascido em seres humanos. No entanto, a concentração do GH- hormônio de crescimento derivado da placenta (derivado do gene GHV) encontra-se significativamente diminuído no sangue de uma gestante portadora de um feto com RCIU-Retardo de crescimento intrauterino. Entretanto, esse paradoxo se prolonga em suas funções fisiológicas, metabólicas de origem genética. Outra substância de importância significativa que possui o nome oficial deste gene é o "fator de crescimento semelhante à insulina 2” (somatomedina A). O "IGF-2 é o símbolo oficial do gene. O gene IGF-2 também é conhecido por outros nomes, O gene IGF-2 fornece instruções para fazer uma proteína chamada fator de crescimento semelhante à insulina-2. Esta proteína tem um papel essencial no crescimento e desenvolvimento antes do nascimento, ainda intra-útero. Estudos sugerem que o fator de crescimento semelhante à insulina-2 promove o crescimento e divisão (proliferação) de células em muitos tecidos diferentes. Embora o gene IGF-2 é altamente ativo durante o desenvolvimento fetal, é muito menos ativo no organismo adulto. As pessoas herdam uma cópia da maioria dos genes de sua mãe e de seu pai. Ambas as cópias são normalmente ativas, ou "ligadas", nas células. Para o gene IGF-2, no entanto, a cópia que é herdada do pai de uma pessoa é a única cópia ativa na maioria das partes do corpo.
- 4. Este tipo de diferença específica do pai na ativação do gene é causada por um fenômeno chamado de “imprinting genômico”. O IGF-2 é parte de um grupo de genes no braço curto (p) do cromossoma 11 que passam por “imprinting genômico”. Outro gene, neste conjunto, H19, também está envolvido no crescimento e desenvolvimento. A região vizinha de DNA conhecido como centro de “imprinting 1” (ICR1) ou o H19 região diferencialmente mutilada (H19 DMR) controla o “imprinting genômico” específico do pai de ambos os genes H19 e IGF-2. Na verdade desde o momento de pensarmos em uma concepção, devemos ter a responsabilidade das implicações altamente complexas que acompanharão nossa decisão, tomando todas as ações preventivas e aceitar as intercorrências que eventualmente não esperamos, pois qualquer deslize tem consequências. DIFFERENCES OF FETAL GROWTH-AFTER FETAL; CHILDREN – KIDS AND YOUTH: GROWTH HORMONE CLASSICS AND OF FETAL GROWTH. PARADOX; FETAL DEVELOPMENT (PRENATAL), AFTER BORN, CHILDREN, JUVENILE AND YOUTH: THE GROWTH HORMONES MEDIATING POSTNATAL NOT NECESSARILY PERFORM THE SAME FUNCTIONS IN FETAL GROWTH. PHYSIOLOGY-ENDOCRINOLOGY- NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. Growth hormone (GH) is present in very high concentrations in the fetus, in contrast to its limited the growth hormone GH - receptor presence. Despite this discrepancy suggest a limited activity of the growth hormone- GH in the fetus growth, plays a role in fetal growth as shown in 1 standard deviation of the mean birth weight (SD) below the mean in children deficiency of growth hormone-GH.
- 5. Children with GH insensitivity due to abnormal GH receptors, reduced or absent (e.g., Laron syndrome) have elevated GH and low serum levels of insulin-like growth factor-I (IGF-I), they also have height and weight reduced. A deficiency of thyroid hormone does not directly affect birth weight, but a prolonged pregnancy can be a finding of congenital hypothyroidism, babies born with congenital hypothyroidism may show no effect, or may display mild effects that often go unrecognized as a problem: sleep excessive, reduced muscle tone, low or hoarse cry, frequent bowel movements, exaggerated jaundice and low body temperature. If fetal disability was severe because of the complete absence (athyreosis) gland, physical characteristics may include a larger anterior fontanels and the persistence of a posterior fontanels, an umbilical hernia, and a large tongue (macroglossia). Before the period of newborn screening less than half of the cases of severe hypothyroidism have been recognized in the first month of life. As the months passed, these babies grow poorly and were delayed in their development. For several years, would submit cretinism of recognizable facial and bodily features. Persistence of severe hypothyroidism without adequate treatment resulted in severe mental retardation, with an IQ below 80, most of the time. Most of these children eventually ended up in institutional care. Congenital hypothyroidism (CH) is a condition of deficiency of thyroid hormone present at birth. About 1 in 4,000 newborns have a severe deficiency of thyroid function, while even more have mild or partial degrees. If untreated for several months after birth, severe congenital hypothyroidism can lead to growth failure with
- 6. low intra-utero stature, newborn, and toddler, infant, adolescent and youth sadly resonate mainly in adults without proper treatment. This situation is permanent and irreversible after installed with its squealed and permanent intellectual disability. The placental lactogen had no effect on the size of the newborn in humans. However, the concentration of GH, growth hormone derived from the placenta (GHV-derived gene) is significantly decreased in the blood of a pregnant woman carrying a fetus to IUGR, intrauterine growth retardation. However this paradox extends to its physiological functions, metabolic genetic origin. Another substance of significant importance has the official name of this gene is “insulin-like growth factor-2 (somatomedin A). The "IGF-2 is the official symbol of the gene. The IGF-2 gene is also known by other names, the IGF-2 gene provides instructions for making a protein called insulin- like growth factor-2. This protein has an essential role in the growth and development before birth. Studies suggest that the insulin-like growth factor-2 promotes growth and division (proliferation) of cells in many different tissues. Although the IGF-2 gene is highly active during fetal development, which is much less active in the adult organism. People inherit one copy of most genes from their mother and their father. Both copies are normally active, or "turned on” in cells. For the IGF-2 gene, however, is that the copy inherited from the father of a person is the only active copy in most parts of the body. This type of specific difference of the father in gene activation is caused by a phenomenon called “genomic imprinting” IGF-2 is part of a cluster of genes on the short arm (p) of chromosome 11 that pass through “genomic imprinting”. Another gene in
- 7. this set, H19, is also involved in growth and development. The neighboring region of DNA known as “imprinting center 1 (ICR1)” or H19 differentially mutilated region (H19 DMR) controls the specific “genomic imprinting Dad” both H19 and IGF-2 genes. In fact from the moment we consider a design, we have the responsibility of highly complex implications that accompany our decision, taking all preventive actions and accept the events that eventually did not expect, because any slip has consequences. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Um dos fatores que mais atormentam os profissionais da área de crescimento, ou seja, o endocrinologista, neuro endocrinologista, endócrino-pediatra (sub-divisão da endocrinologia), é a qualidade das chapas de raio–x, diferenças entre radiografias de diversas crianças e pressa na apreciação das chapas... http://hormoniocrescimentoadultos.blogspot.com. 2. Em duplicata por um mesmo observador é muito pequeno: o mesmo não ocorre na leitura de uma mesma radiografia por dois observadores, e daí a necessidade de os estudos serem feitos sempre por um mesmo observador... http://longevidadefutura.blogspot.com 3. O método é digno de confiança para comparar a IO–idade óssea de grupos, mas de valor duvidoso se baseado em uma única radiografia... http://imcobesidade.blogspot.com
- 8. AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio, H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Definitions and Indicators in Family Planning. Maternal & Child Health and Reproductive Health. By European Regional Office, World Health Organization. Revised March 1999 & January 2001. In turn citing: WHO Geneva, WHA20.19, WHA43.27, Article 23; Singh, Meharban (2010). Care of the Newborn. p. 7. Edition 7. ISBN 9788170820536 patient.co.uk » PatientPlus » Antepartum Haemorrhage Last Updated: 5 May 2009; The Royal Women’s Hospital > antepartum haemorrhage Retrieved on Jan 13, 2009; Schacter, Daniel (2009). "11- Development". Psychology Second Edition. United States of America: Worth Publishers. ISBN 978-1- 4292-3719-2; Wilcox AJ, Baird DD, Weinberg CR (June 1999). "Time of implantation of the conceptus and loss of pregnancy". N. Engl. J. Med. 340 (23): 1796–9. doi:10.1056/NEJM199906103402304. PMID 10362823; Kimmel SR, et al. Growth and development. In: Rakel RE. Textbook of Family Medicine. 7th ed. Philadelphia, Pa.: Saunders Elsevier; 2007. Accessed Sept. 18, 2009; Olsson J. The newborn. In: Kliegman R. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, Pa.: Saunders Elsevier; 2007.; Birth to 3 months: Your baby's development. Zero to Three. Accessed Sept. 18, 2009; Persing J, et al. Prevention and management of positional skull deformities in infants. Pediatrics. 2003;112:199. Contato: Fones: 55 11 5087-4404 ou 96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - Bloco D - 12º andar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails: drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr