1. 2-Aminoimidazole Suppression of Drug Resistant Mycobacterium Tuberculosis
William Hoffert, Vu Nguyen, Meghan Blackledge, and Christian Melander*
Department of Chemistry, North Carolina State University, Raleigh, NC 27695, ccmeland@ncsu.edu
Synthesis of 2-ABI2
• 3-step synthetic route to synthesize lead 2-ABI compound.
• The route is not efficient for creating a diversified library because diversification would have to be
introduced in the first step of the synthetic scheme.
• A new protecting group based synthetic route is needed in which acylation occurs near the end.
Synthesis of 2-ABI Analogs
We thank North Carolina State University and Nation Institute of Health for their generous support.
Also, a special thanks to all members of the Melander lab, past and present.
Summary
References
Introduction
Tuberculosis is a bacterial infection, and antibiotics are used for treatment. However, due to
improper use of antibiotics, strains of Mycobacterium tuberculosis have become resistant to many
antibiotics. Multidrug-resistant TB (MDR TB) is immune to either isoniazid and rifampin, which are
first-line antibiotics for TB.1 MDR TB is commonly treated with intravenous second-line antibiotics,
such as amikacin, kanamycin, or capreomycin, and an extensive chemotherapy program for up to
two years.2 Unfortunately, these medications are not readily available in many places, are
expensive, and can have severe side effects.2 Furthermore, Extensive Drug Resistant TB or XDR
TB is a strain resistant to all first line antibiotics, fluoroquinolone, and at least one second-line
antibiotic.3 XDR TB is a major concern for pathologists, because treatment is intense, expensive,
has many side effects, and treatment rates are around 30-50% worldwide.3 MDR TB and XDR TB
are becoming increasingly more common across the world; an estimated 650,000 people are
infected with MDR TB, and 9% of those have XDR TB.4 In addition, 65 cases of XDR TB have been
confirmed in the United States from 1993 to 2011.4 In order to slow TB resistance, pharmaceutical
companies are forced to develop more complex and expensive medications, making TB treatment
more more expensive and inaccessible to those in developing nations. In order to have a lasting
impact on TB antibiotic resistance, we are synthesizing a new medication that works by targeting
antibiotic resistance at its source. Through resensitizing TB to common antibiotics, treatment for
those infected with XDR and MDR TB will be easier than before, with better prognoses.
Acknowledgements
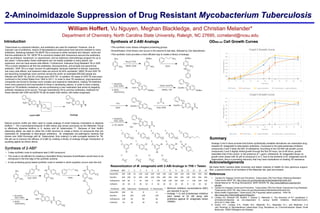
Resensitization of M. smegmatis with 2-ABI Analogs in 7H9 + Tween
OD600 nm Cell Growth Curves
• Minimum inhibitory concentrations (MIC)
are reported in ug mL-1
• Analogs 1-14 and β-lactamase inhibitors
were tested at 20 uM along with
antibiotics against M. smegmatis (strain
700084)
Natural product motifs are often used to create analogs of small molecule modulators to disperse
biofilms. 5 The 2-aminobenzimidazole (2-ABI) below was shown previously by the Melander Group
to effectively dipserse biofilms in S. aureus and M. tuberculosis. 5,6 Because of their biofilm
dispersing ability, we seek to utilize the 2-ABI structure to create a library of compounds that can
resensitize M. smegmatis to beta-lactam antibiotics. M. smegmatis non-pathogenic bacteria that
shares over 2000 homologs with M. Tuberculosis, thus making it a safe surregate bacteria for TB.
We set out to improve the efficacy of 2-ABI by creating a library of analogs through introduction of
acylating agents as shown above.
•This synthetic route utilizes orthoganol protecting groups.
•Diversification of the library now occurs in the second to last step, followed by Cbz deprotection.
•This synthetic route provides a more efficient way to create a library of analogs.
Analogs 2 and 5 show promise that further synthetically available derivatives can resensitize drug
resistant M. smegmatis to beta-lactam antibiotics. Compared to the beta-lactamase inhibitors,
compounds 2 and 5 lower the MIC of cefotaxime. According to the OD-600 cell growth curves
compounds 2 and 5 slightly inhibit growth through the first 24 hours, but at 48 hours, growth
resembles that of the control. In the presence of 1 μg/mL cefotaxime, M. smegmatis shows no
growth when dosed with 20 μM of compound 2 or 5. Due to the similarity of M. smegmatis and M.
tuberculosis, this is a promising discovery that may have implications on treating TB resistance.
1. Centers for Disease Control and Prevention. Tuberculosis (TB) Fact Sheet: Multidrug-Resistant
Tuberculosis (MDR TB). http://www.cdc.gov/tb/publications/factsheets/drtb/mdrtb.htm.
2. Global Alliance for TB Drug Development. MDR-TB/XDR-TB. http://www.tballiance.org/why/mdr-
xdr.php.
3. Centers for Disease Control and Prevention. Tuberculosis (TB) Fact Sheet: Extensively Drug-Resistant
Tuberculosis (XDR TB). http://www.cdc.gov/tb/publications/factsheets/drtb/xdrtb.htm.
4. World Health Organization. Tuberculosis (TB) Frequently asked questions - XDR-TB.
http://www.who.int/tb/challenges/xdr/faqs/en/.
5. Lindsey EA, Brackett CM, Mullikin T, Alcaraz C, Melander C. The discovery of N-1 substituted 2-
aminobenzimidazoles as zinc-dependent S. aureus biofilm inhibitors. MedChemComm.
2012;3(11):1462-1465.
6. Ackart, D.F., Lindsey, E.A., Podell, B.K., Melander, R.J., Basaraba, R.J., and Melander, C.In
vitro Reversal of Mycobacterium tuberculosis Drug Resistance by 2-Aminoimidazole Based Small
Molecules. FEMS Pathogens and Disease.
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0 5 10 15 20 25 30 35 40 45 50
CellGrowth(OD600nm)
Time (hrs.)
Cmpd 2 Growth Curve
Control 20 uM Cmpd 2 1 ug/mL Cefotaxime 20 uM Cmpd 2 + 1 ug/mL Cefotaxime
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0 5 10 15 20 25 30 35 40 45 50
CellGrowth(OD600nm)
Time (hrs.)
Cmpd 5 Growth Curve
Control 20 uM Cmpd 5 1 ug/mL Cefotaxime 20 uM Cmpd 5 + 1 ug/mL Cefotaxime