Oral antidiabetics
•Als PPTX, PDF herunterladen•
23 gefällt mir•8,687 views

Oral antidiabetics

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Oral antidiabetics
Ähnlich wie Oral antidiabetics (20)
Mehr von BikashAdhikari26
Mehr von BikashAdhikari26 (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Oral antidiabetics
- 2. Meglitinide Analogs Sulphonylureas Thiazolindinediones Metformin (Biguanides) Alpha Glucosidase Inhibitors
- 3. Classification of oral anti-diabetic drugs A. Enhance Insulin Secretion 1. Sulfonylureas (K+ ATP channels blockers) • First Generation: Tolbutamide • Second Generation: Glibenclamide, Glipizide, Gliclazide, Glimepiride 2. Meglitinide analouges: Repaglinide, Nateglinide 3. Glucagon-like peptide (GLP-1) receptor agonists (injectable): Exenadite, Liraglutide 4. Dipeptidyl peptidase-4 (DPP-4) inhibitors: Sitagliptin, Vildagliptin, Saxagliptin, Alogliptin, Linagliptin B. Overcome Insulin Resistance 1. Biguanides (AMPK activators): Metformin 2. Thiazolidinediones (PPARγ activator): Pioglitazone C. Miscellaneous 1. α-Glucosidase inhibitors: Acarbose, Miglitol, Voglibose 2. Amylin analogue: Pramlintide 3. Dopamine D2 receptor agonist: Bromocriptine 4. Sodium Glucose Co-Transport 2 (SGLT 2) inhibitor: Dapagliflozine
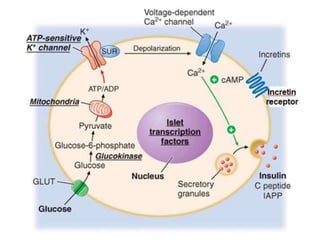
- 5. Sulfonylureas (K+ ATP channels blockers) Insulin secretagogue Requires at least 30% functional β cells • Glibenclamide, Glicazide, Glipizide, Glimepiride • MOA: ↑ insulin secretion by acting on sulfonylurea receptor at ATP sensitive K+ channel • Acts by blocking the K+ ATP channel that reduces influx of rectifying K+ ion current & causes partial depolarization of pancreatic beta-cells increased influx of Ca++ ions as well as release of Ca++ from intracellular stores & promotes exocytotic release of insulin. • Chronic use: sensitize the target tissue to the action of insulin • Slow hepatic degradation of insulin • Reduces glucagon secretion
- 7. Pharmacokinetics: • Well absorbed orally • High plasma protein bound (90%) • Single daily dose is sufficient Adverse Effects: • Hypoglycaemia • Non specific Side effects: weight gain, nausea, vomiting, flatulence, diarrhoea, constipation, headache, paresthesia; mild and infrequent • Hypersensitivity: Rashes, photosensitivity, purpura, transient leukopenia, rarely agranulocytosis • SU + alcohol: flushing, disulfiram-like reaction Should not be used in pregnancy and lactating mothers !
- 8. MEGLITINIDE/PHENYLALANINE ANALOGUES Mechanism of Action: • K+ ATP channel blockers; quick and short lasting action • Normalises meal time glucose levels Repaglinide and Nateglinide: • Quickly absorbed and rapidly metabolised • Administered before each major meal, omit if meal missed. • Lower incidence of hypoglycaemia Indication: • Type 2 DM with pronounced postprandial hyperglycaemia • Along with Metformin/long acting insulin S/E: Mild headache, dyspepsia, arthralgia weight gain Avoid in liver disease!
- 10. GLUCAGON-LIKE PEPTIDE-1 (GLP) RECEPTOR AGONISTS MOA: GLP-1 is an important incretin released from the gut in response to ingested glucose. It induces insulin release from pancreatic β cells, inhibits glucagon release from α cells, slows gastric emptying and suppresses appetite. Exenatide: • Synthetic dipeptidyl peptidase-4 (DPP-4) enzyme resistant analogue. • Activates GLP receptors • Cannot be given orally • Used as an add-on drug to metformin/SU/Pioglitazone • Lowers postprandial as well as fasting blood glucose, HbA1c and body weight S/E: nausea/vomiting, tolerance develops later Liraglutide: • Highly bound to plasma proteins: longer duration of action
- 12. DIPEPTIDYL PEPTIDASE-4 (DPP-4) INHIBITORS DPP-4 enzyme causes rapid degradation of endogenous GLP- 1, thus orally active inhibitors of this enzyme have been developed as indirectly acting insulin secretagogues. Sitagliptin: • MOA: Acts as competitive and selective DPP-4 inhibitor & potentiates the action of GLP-1 and GIP. • Boosts postprandial release, decreases glucagon secretion and lowers meal time as well as fasting blood glucose in Type 2DM • Body weight neutral, low risk of hypoglycaemia • Well absorbed orally, little metabolised, largely excreted unchanged in urine • Dose reduction needed in renal dysfunction • S/E: nausea, loose stools, headaches, rashes, allergic reactions, edema
- 14. BIGUANIDES (METFORMIN) Biguanides do not cause insulin release, but presence of insulin is essential for their action. MOA: Metformin causes activation of AMPK, leading to: • Suppression of hepatic gluconeogenesis • Enhances insulin-mediated glucose uptake and disposal in skeletal muscle and fat • Interferes with mitochondrial respiratory chain and promotes peripheral glucose utilization • Retards glucose absorption of glucose, hexose, amino acids, Vit B12 Adverse Effects: Hypoglycaemia in overdose, Lactic acidosis, Vitamin B12 deficiency Contraindicated in hypotensive states, heart failure, severe respiratory, hepatic and renal disease, alcoholics Advantages: nonhypoglycaemic, weight loss, prevents long term complications, prolongs beta cell life Limiting feature: gastrointestinal intolerance
- 16. THIAZOLIDINEDIONES (PPARγ ACTIVATOR): MOA: Pioglitazone is selective agonist for the nuclear peroxisome proliferator-activated receptor γ (PPARγ) expressed mainly in fat cells, and in muscle cells. It enhances transcription of insulin responsive genes & tends to reverse insulin resistance by enhancing GLUT4 receptor expression and translocation. • Suppresses hepatic gluconeogenesis • Additionally, lowers serum triglyceride, raises HDL • Well tolerated S/E: plasma volume expansion, edema, weight gain, headache, myalgia, mild anaemia, increased risk of fracture esp. in elderly women Contraindicated in liver disease and in CHF
- 18. Miscellaneous α GLUCOSIDASE INHIBITORS Acarbose: MOA: Inhibits α-glucosidases (enzyme responsible for digestion of carbohydrates in the brush border of small intestine mucosa) slow down and decrease digestion and absorption of polysaccharides and sucrose. Dose 50–100 mg TDS is taken at the beginning of each major meal. Additionally it promotes GLP-1 release. S/E: Flatulence, abdominal discomfort, loose stool; Poor patient acceptability Miglitol: It has a smaller molecule than acarbose, and it is a stronger inhibitor of sucrase. Potency for other α-glucosidases is equivalent to acarbose. Dose: 25–100 mg TDS at beginning of each meal. Voglibose: It has properties, use and side effects similar to that of acarbose. Dose: 0.2–0.3 mg TDS just before meals.
- 20. AMYLIN ANALOGUE Amylin is produced by pancreatic β cells and acts in the brain to reduce glucagon secretion from α cells, delay gastric emptying, retard glucose absorption and promote satiety. Pramlintide: • Synthetic amylin analogue injected s.c. before meal attenuates postprandial glycaemia and exerts centrally mediated anorectic action. • Reduction in body weight is additional benefit. Bromocriptine: it is dopamine D2 agonist that acts on hypothalamic dopaminergic control of the circadian rhythm of hormone (GH, prolactin, ACTH) release and reset it to reduce insulin resistance. Dapagliflozin: It inhibits sodium-glucose co-transport-2 (SGLT-2), which is major transporter for glucose reabsorbtion in the proximal tubules. Thus it induces glucosuria and lowers blood glucose in type 2 DM, as well as causes weight loss.
- 24. HbA1c?
- 26. THANK YOU FOR YOUR KIND ATTENTION ! FOR FURTHER REFERENCE PLEASE SEE K. D. TRIPATHI!