![[object Object],10 20 30 40 50 60 High BP CAD CHF Stroke Other 50,000,000 12,200,000 4,600,000 4,400,000 2,800,000 Prevalence (millions) BP=blood pressure, CAD=coronary artery disease, CHF=congestive heart failure ,[object Object],[object Object],(24%)](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Hypertension
Ähnlich wie Hypertension (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Hypertension
- 1. Hypertension: New Concepts, Guidelines, and Clinical Management Nathan D. Wong, PhD, FACC Associate Professor and Director Heart Disease Prevention Program Division of Cardiology, Department of Medicine College of Medicine, University of California, Irvine
- 3. Age Distribution of Hypertensives in US Population (NHANES III and the 1991 Census) 3.7 9.5 13 21.3 23.7 19.2 9.6 Hypertensives Within Age Group (%) Franklin SS. J Hypertension. 1999;17(suppl 5):S29-S36. Age Groups (y) 47.4 million hypertensives 26.0% of US population 26% 74% 0 5 10 15 20 25 30 18-29 30-39 40-49 50-59 60-69 70-79 80+
- 4. <40 40-49 50-59 60-69 70-79 80+ Age (y) 17% 16% 16% 20% 20% 11% Distribution of Hypertension Subtype in the untreated Hypertensive Population in NHANES III by Age Numbers at top of bars represent the overall percentage distribution of untreated hypertension by age. Franklin et al. Hypertension 2001;37: 869-874 . Frequency of hypertension subtypes in all untreated hypertensives (%) ISH (SBP 140 mm Hg and DBP <90 mm Hg) SDH (SBP 140 mm Hg and DBP 90 mm Hg) IDH (SBP <140 mm Hg and DBP 90 mm Hg) 0 20 40 60 80 100
- 5. Hypertension: A Significant CV and Renal Disease Risk Factor Peripheral vascular disease Morbidity Disability Renal disease CAD CHF LVH Stroke Hypertension National High Blood Pressure Education Program Working Group. Arch Intern Med. 1993;153:186-208.
- 6. Benefits of Lowering BP Average Percent Reduction Stroke incidence 35–40% Myocardial infarction 20–25% Heart failure 50%
- 7. Preventable CHD Events from Control of Hypertension in US Adults (Wong et al., Am Heart J 2003; 145: 888-95) PAR% = population attributable risk (proportion of CHD events preventable), NNT = number needed to treat to prevent 1 CHD event ; <0.01 comparing men and women for PAR%
- 9. BP Control Rates Trends in awareness, treatment, and control of high blood pressure in adults ages 18–74 Sources: Unpublished data for 1999–2000 computed by M. Wolz, National Heart, Lung, and Blood Institute; JNC 6. 34 27 29 10 Control 59 54 55 31 Treatment 70 68 73 51 Awareness 1999–2000 II (Phase 2) 1991–94 II (Phase 1) 1988–91 II 1976–80 National Health and Nutrition Examination Survey, Percent
- 10. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) National Heart, Lung, and Blood Institute National High Blood Pressure Education Program U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute
- 11. Blood Pressure Classification <80 and <120 Normal 80–89 or 120–139 Prehypertension 90–99 or 140–159 Stage 1 Hypertension > 100 or > 160 Stage 2 Hypertension DBP mmHg SBP mmHg BP Classification
- 13. 4-Year Progression To Hypertension: The Framingham Heart Study (<120/80 mm Hg) (130/85 mm Hg) (130-139/85-89 mm Hg) Vasan, et al. Lancet 2001;358:1682-86 Participants age 36 and older
- 14. Impact of High-Normal BP on Risk of Major CV Events* in Men * Defined as death due to CV disease; recognized myocardial infarction (MI), stroke, or congestive heart failure (CHF). Adapted from Vasan RS. N Engl J Med. 2001;345:1291-1297. Cumulative Incidence (%) of Major CV Events Time (y) Optimal BP (<120/80 mm Hg) Normal BP (120-129/80-84 mm Hg) High-normal BP (130-139/85-89 mm Hg) 16 12 10 8 6 4 2 0 14 0 2 4 6 8 10 12
- 15. HOT Study: Significant Benefit From Intensive Treatment in the Diabetic Subgroup Hansson L et al. Lancet. 1998;351:1755-1762. 0 5 10 15 20 25 90 85 80 Major cardiovascular events/1,000 patient-years p =0.005 for trend mm Hg Target Diastolic Blood Pressure
- 16. SBP-Associated Risks: MRFIT Adapted from Neaton JD et al. Arch Intern Med . 1992;152:56-64 . SBP versus DBP in Risk of CHD Mortality Diastolic BP (mm Hg) Systolic BP (mm Hg) CHD Death Rate 100+ 90–99 80–89 75–79 70–74 <70 <120 120–139 140–159 160+ 48.3 20.6 10.3 11.8 8.8 8.5 9.2 23.8 16.9 13.9 12.8 12.6 11.8 31.0 25.5 24.6 25.3 25.2 24.9 37.4 34.7 43.8 38.1 80.6
- 19. SHEP: Outcomes * P =.0003 vs placebo. Adapted from SHEP Cooperative Research Group. JAMA . 1991;265:3255-3264. Risk Reduction Risk Reduction (%) 0 – 10 – 20 – 30 – 40 – 50 – 36* Total Mortality – 13 Stroke
- 21. Syst-Eur: Outcomes * P =.003; † P =.03; ‡ P =.12; § P <.001. Adapted from Staessen JA et al. Lancet . 1997;350:757-764 . Percent Reduction 0 – 5 – 10 – 15 – 20 – 25 – 30 – 35 – 40 – 45 – 42* Heart Failure Stroke All Cardiac Endpoints All Fatal/Nonfatal Cardiac Endpoints MI – 26 † – 29 ‡ – 30 ‡ – 31 § Risk Reduction
- 24. ATP III: The Metabolic Syndrome* *Diagnosis is established when 3 of these risk factors are present. † Abdominal obesity is more highly correlated with metabolic risk factors than is BMI. ‡ Some men develop metabolic risk factors when circumference is only marginally increased. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA . 2001;285:2486-2497. © 2001, Professional Postgraduate Services ® www.lipidhealth.org <40 mg/dL <50 mg/dL Men Women >102 cm (>40 in) >88 cm (>35 in) Men Women 110 mg/dL Fasting glucose 130/ 85 mm Hg Blood pressure HDL-C 150 mg/dL TG Abdominal obesity † (Waist circumference ‡ ) Defining Level Risk Factor
- 25. Prevalence of Selected Risk Factors in US Adults with the Metabolic Syndrome (without Diabetes) (Wong et al., Am J Cardiol 2003, in press)
- 26. Estimated Proportion of CHD Events Preventable by Control of Blood Pressure, HDL-C, LDL-C, and All 3 Factors to “Optimal” Levels in Persons with the Metabolic Syndrome (Wong et al., Am J Cardiol 2003, in press) ** * * p<0.05, ** p<0.01 compared to men
- 28. Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group Chlorthalidone Amlodipine Lisinopril Years to CHD Event 0 1 2 3 4 5 6 7 Cumulative CHD Event Rate 0 .04 .08 .12 .16 .2 0.81 0.99 (0.91-1.08) L/C 0.65 0.98 (0.90-1.07) A/C p value RR (95% CI) ALLHAT
- 29. Cumulative Event Rates for Stroke by ALLHAT Treatment Group Chlorthalidone Amlodipine Lisinopril Cumulative Stroke Rate Years to Stroke 0 1 2 3 4 5 6 7 0 .02 .04 .06 .08 .1 0.02 1.15 (1.02-1.30) L/C 0.28 0.93 (0.81-1.06) A/C p value RR (95% CI) ALLHAT
- 30. Cumulative CHF Rate Years to HF 0 1 2 3 4 5 6 7 0 .03 .06 .09 .12 .15 Cumulative Event Rates for Heart Failure by ALLHAT Treatment Group Chlorthalidone Amlodipine Lisinopril <.001 1.19 (1.07-1.31) L/C <.001 1.38 (1.25-1.52) A/C p value HR (95% CI) ALLHAT
- 31. Overall Conclusions Because of the superiority of thiazide-type diuretics in preventing one or more major forms of CVD and their lower cost, they should be the drugs of choice for first-step antihypertensive drug therapy. ALLHAT
- 35. BP Measurement Techniques Provides information on response to therapy. May help improve adherence to therapy and evaluate “white-coat” HTN. Self-measurement Indicated for evaluation of “white-coat” HTN. Absence of 10–20% BP decrease during sleep may indicate increased CVD risk. Ambulatory BP monitoring Two readings, 5 minutes apart, sitting in chair. Confirm elevated reading in contralateral arm. In-office Brief Description Method
- 41. Lifestyle Modification Approximate SBP reduction (range) Modification 5–20 mmHg/10 kg weight loss Weight reduction 8–14 mmHg Adopt DASH eating plan 2–8 mmHg Dietary sodium reduction 4–9 mmHg Physical activity 2–4 mmHg Moderation of alcohol consumption
- 44. Algorithm for Treatment of Hypertension Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease ) Initial Drug Choices Lifestyle Modifications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. With Compelling Indications Stage 2 Hypertension (SBP > 160 or DBP > 100 m mHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Stage 1 Hypertension (SBP 140 –159 or DBP 90–99 mmHg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Without Compelling Indications Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist.
- 45. Classification and Management of BP for adults *Treatment determined by highest BP category. † Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension. ‡ Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mmHg. Two-drug combination for most † (usually thiazide-type diuretic and ACEI or ARB or BB or CCB). Yes or > 100 > 160 Stage 2 Hypertension Drug(s) for the compelling indications. ‡ Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Yes or 90–99 140–159 Stage 1 Hypertension Drug(s) for compelling indications. ‡ No antihypertensive drug indicated. Yes or 80–89 120–139 Prehypertension Encourage <80 <120 & Normal With compelling indications Without compelling indication Initial drug therapy Lifestyle modification DBP* mmHg SBP* mmHg BP classification
- 49. Compelling Indications for Individual Drug Classes Clinical Trial Basis Initial Therapy Compelling Indication ALLHAT, HOPE, ANBP2, LIFE, CONVINCE ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS ACC/AHA Heart Failure Guideline, MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES THIAZ, BB, ACE, CCB BB, ACEI, ALDO ANT THIAZ, BB, ACEI, ARB, ALDO ANT High CAD risk Postmyocardial infarction Heart failure
- 50. Compelling Indications for Individual Drug Classes Recurrent stroke prevention Chronic kidney disease Diabetes Clinical Trial Basis Initial Therapy Options Compelling Indication PROGRESS NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK NKF-ADA Guideline, UKPDS, ALLHAT THIAZ, ACEI ACEI, ARB THIAZ, BB, ACE, ARB, CCB
- 53. Relative Risk of CV Events and Mortality: CCBs vs Diuretics or Beta Blockers CCBs, calcium channel blockers. CHD, coronary heart disease. * Includes INSIGHT, NICS-EH, STOP-2, NORDIL, and VHAS. Diamonds represent the 95% CI for pooled estimates of effect and are centered on pooled relative risk. Adapted from Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet . 2000;356:1955-1964. Stroke 456 529 0.87 (0.77-0.98) CHD 567 510 1.12 (1.00-1.26) Heart Failure 278 250 1.12 (0.95-1.33) Major CV Events 1,251 1,234 1.02 (0.95-1.10) CV Death 425 405 1.05 (0.92-1.20) Total Mortality 776 776 1.01 (0.92-1.11) Relative Risk Favors CCBs Favors diuretics or beta blockers CCBs (n=11,685) Diuretics or Beta Blockers (n=11,769) 0.5 1.0 2.0 No. of Events* Relative Risk (95% CI)
- 54. HOPE: Risk Reduction of CV Events Associated with ACEI (RAS Inhibition) Treatment Adapted from The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med . 2000;342:145-153. -22 ( P <.001) MI, Stroke, CV Death (primary end point) -26 ( P <.001) CV Death -20 ( P <.001) MI -32 ( P <.001) Stroke -16 ( P =.005) All-cause Death -35 -30 -25 -20 -15 -10 -5 0 Risk Reduction (%)
- 55. Relative Risk of CV Events and Mortality: ACE Inhibitors vs Diuretics or Beta Blockers CHD, coronary heart disease. * Includes STOP-2, UKPDS-HDS, and CAPPP. Diamonds represent the 95% CI for pooled estimates of effect and are centered on pooled relative risk. Adapted from Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet . 2000;356:1955-1964. Stroke 425 402 1.05 (0.92-1.19) CHD 423 420 1.00 (0.88-1.14) Heart Failure 223 250 0.92 (0.77-1.09) Major CV Events 1,018 1,004 1.00 (0.93-1.08) CV Death 350 348 1.00 (0.87-1.15) Total Mortality 639 618 1.03 (0.93-1.14) Relative Risk Favors ACE inhibitors Favors diuretics or beta blockers No. of Events* ACE Inhibitors (n=8,097) Diuretics or Beta Blockers (n=8,064) 0.5 1.0 2.0 Relative Risk (95% CI)
- 56. Reversal of LV Hypertrophy By Antihypertensive Treatment Schmieder RE et al. JAMA. 1996;275:1507-1513. Change in LV mass index (%) Diuretics -blockers Calcium channel blockers ACE inhibitors p <.01 p <.01 7% 6% 9% 13% 0 -5 -10 -15 -20 -25
- 57. Regression of LV Hypertrophy Predicts Prognosis LV, left ventricular. Nonregressors defined as baseline and follow-up left ventricular mass index (LVMI) >125 g/m 2 ; regressors defined as baseline LVMI >125 g/m 2 and follow-up LVMI <125 g/m 2 . Adapted from Verdecchia P et al. Circulation. 1998;97:48-54. Probability of event-free survival (%) Rate of events (per 100 patient-yrs) Time to event (wk) P =.002 Regressors (n=285) Nonregressors (n=145) Regressors (n=52) Nonregressors (n=50) 0 100 200 300 400 500 100 90 80 70 0 60 50 7 6 5 4 1 3 2 0
- 58. Irbesartan and Atenolol in Hypertension and LVH Study Design Single-blind Placebo Irbesartan 150-300 mg Atenolol 50-100 mg Addition of HCTZ 12.5-25 mg if SeDBP 90 mm Hg Addition of Felodipine 5-10 mg if SeDBP 90 mm Hg Wk: -4 0 12 24 48 * BP, echocardiography, neurohormone measurements. Malmqvist K et al. J Hypertens. 2001;19:1167-1176. * Double Blind * * *
- 59. Irbesartan vs Atenolol in Hypertension and LVH: SeDBP Reduction -20 -15 -10 -5 0 12 wk 24 wk 48 wk % reduction in SeDBP Irbesartan Atenolol * * † * * * * * p <.001 vs baseline. † p <.028 irbesartan vs atenolol. Malmqvist K et al. J Hypertens. 2001;19:1167-1176.
- 60. Irbesartan vs Atenolol in Hypertension and LVH: LVMI Reduction -18 -16 -14 -12 -10 -8 -6 -4 -2 0 % change in LVMI (g/m 2 ) * p <.001 vs baseline; † p =.024 irbesartan vs atenolol. Malmqvist K et al. J Hypertens. 2001;19:1167-1176. Irbesartan Atenolol 12 wk * 24 wk * * 48 wk * * †
- 62. LIFE: Dosing * Other antihypertensives excluding ACEIs, AII antagonists, beta-blockers. Adapted from Dahlöf B et al. Am J Hypertens. 1997;10:705-713. Titration to target blood pressure: <140 / <90 mmHg Placebo Run-in Losartan 50 mg Atenolol 50 mg Losartan 50 mg + HCTZ 12.5 mg Losartan 100 mg + HCTZ 12.5 mg Losartan 100 mg + HCTZ 12.5-25 mg + others* Atenolol 50 mg + HCTZ 12.5 mg Atenolol 100 mg + HCTZ 12.5 mg Atenolol 100 mg + HCTZ 12.5-25 mg + others* Average follow up 4.7 years
- 63. LIFE: Blood Pressure Results – Follow-up Study Month Systolic Diastolic Mean Arterial mmHg Atenolol Losartan Atenolol 145.4 mmHg Losartan 144.1 mmHg Atenolol 80.9 mmHg Losartan 81.3 mmHg B Dahl ö f et al. Lancet. 2002;359:995-1003. 0 6 12 18 24 30 36 42 48 54 40 60 80 100 120 140 160 180
- 68. DASH Fact Sheet
- 69. Your Guide to Lowering Blood Pressure
- 70. Reference Card
- 74. MRFIT: Association of Systolic BP and Cardiovascular Death in Type 2 Diabetes < 120 120–139 140–159 160–179 180–199 200 Systolic blood pressure (mm Hg) Cardiovascular mortality rate/10,000 person-yr Nondiabetic Diabetic Stamler J et al. Diabetes Care. 1993;16:434-444. 250 225 200 175 150 125 100 75 50 0 25
- 75. Veterans Administration Hypertension and Screening Clinics 15-Year ESRD Rates and Risk Ratios by Baseline Systolic Blood Pressure SBP (mm Hg) Risk Ratio < 140 > 140 but < 151 > 151 but < 165 > 165 but < 180 > 180 1.00 1.00 1.08 2.07 5.62 Number of screenees: 11,912 (5,730 black; 6,182 white) Source: Perry HM, et al. Hypertension. 1995;25:587-594
- 76. Veterans Administration Hypertension and Screening Clinics 15-Year ESRD Rates and Risk Ratios by Baseline Diastolic Blood Pressure DBP (mm Hg) Risk Ratio < 94 > 94 but < 100 > 100 but < 106 > 106 but < 118 > 118 1.00 1.05 0.89 1.54 4.18 Number of screenees: 11,912 (5,730 black; 6,182 white) Source: Perry HM, et al. Hypertension. 1995;25:587-594
- 80. Correlation Between MAP & Renal Function GFR, glomerular filtration rate; HTN, hypertension; MAP, mean arterial pressure. Adapted from Bakris GL et al. Am J Kidney Dis. 2000;36:646-661. GFR Decline (mL/min/y) MAP (mm Hg) 95 98 101 107 104 110 113 116 119 r=0.69; P <.05 Untreated HTN 130/85 140/90 0 -2 -4 -6 -8 -10 -12 -14
- 81. Microalbuminuria as a Risk Factor for Death in Type 2 Diabetes UAC, urinary albumin concentration. Adapted from Schmitz A et al. Diabetes Med. 1988;5:126-134. Years after Diagnosis Survival UAC 15 g/mL UAC 16-40 g/mL UAC 41-200 g/mL 0.0 0.4 1.0 0.8 0.6 0.2 0 5 10 2 1 3 4 7 6 8 9 11
- 82. Proteinuria & Risk of CV Mortality,Stroke, & CHD Events in Type 2 Diabetes CHD, coronary heart disease; UPC, urinary protein concentration. * Defined as CHD death or nonfatal MI. Adapted from Miettinen H et al. Stroke. 1996;27:2033-2039. A: UPC <150 mg/L B: UPC 150-300 mg/L C: UPC >300 mg/L 1.0 0.9 0.8 0.7 0.6 0.5 0 0 10 20 30 40 50 60 70 80 90 Stroke CHD Events* P <.001 for trends Incidence (%) Reduction in Survival due to CV Mortality Months A B C P -values: Overall <.001 A vs B =.013 A vs C <.001 B vs C <.001 0 10 20 30 40
- 83. Risk Reduction of Diabetes-Related End Points with Tight BP Control * Death due to MI, sudden death, stroke, peripheral vascular disease, renal disease, hyperglycemia, or hypoglycemia. † Fatal or nonfatal. ‡ Retinopathy requiring photocoagulation, vitreous hemorrhage and fatal or nonfatal renal failure. Mean BP achieved with captopril- or atenolol-based therapy: 144/82 mm Hg (tight BP control) vs 154/87 mm Hg (less tight BP control). Adapted from UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713. Risk Reduction (%) Diabetes-related Mortality* Stroke † Microvascular End Points ‡ Myocardial Infarction 32 44 37 21 0 10 20 30 40 50
- 84. HOT: Significant Benefit From Intensive Antihypertensive Treatment in Diabetes * Defined as fatal and nonfatal MI, fatal and nonfatal stroke, and all other CV death. Adapted from Hansson L et al. Lancet. 1998;351:1755-1762. 0 5 10 15 20 25 90 85 80 Major CV Events*/1000 Patient-yrs in Hypertensive Patients with Diabetes P =.005 for trend Target DBP (mm Hg)
- 85. Effect of ACE Inhibition on Nephropathy in Type 1 Diabetes * P=.006 vs placebo. Adapted from Lewis EJ et al. N Engl J Med. 1993;329:1456-1462. Progression to Death, Dialysis, or Transplant (%) Captopril Placebo Follow-up (y) * 0 1 2 3 4 0 10 20 30 40
- 86. IRMA 2: Blood Pressure Response SeSBP, seated systolic blood pressure; SeDBP, seated diastolic blood pressure. Control defined as placebo. * Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and dihydropyridine CCBs) could be added to all groups to help achieve target BP levels. At the end of 2-year follow-up, 56% of patients in the control group, 45% in the irbesartan 150-mg group, and 43% in the irbesartan 300-mg group were receiving concomitant antihypertensive agents. Adapted from Parving H-H et al. N Engl J Med. 2001;345:870-878. Control SeDBP* Irbesartan 150 mg SeDBP* Irbesartan 300 mg SeDBP* Control SeSBP* Irbesartan 150 mg SeSBP* Irbesartan 300 mg SeSBP* Mean SeSBP and SeDBP (mm Hg) Months 0 3 6 9 12 15 18 21 24 27 0 70 130 160 80 90 100 110 120 140 150
- 87. IRMA 2 Primary Endpoint Development of Overt Proteinuria Subjects (%) Control (n=201) 150 mg (n=195) 300 mg (n=194) Irbesartan 9.7 5.2 14.9 RRR=39% P =0.08 RRR=70% P<0.001 Parving H-H, et al. N Engl J Med 2001;345:870-878. 14 18 16 12 10 8 6 4 2 0
- 88. IDNT: Systolic BP, Mean Arterial Pressure, & Diastolic BP Response Control defined as placebo. Patients received an average of 3.0 concomitant antihypertensive agents in the irbesartan and amlodipine groups, and 3.3 concomitant agents in the control group. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. Irbesartan Amlodipine Control Follow-up Visit (mo) SBP MAP DBP BP (mm Hg) 0 6 12 18 24 30 36 42 48 54 80 100 120 140 160
- 89. IDNT Primary Endpoint: Time to Doubling of Serum Creatinine, ESRD, or Death Subjects (%) 0 6 12 18 24 30 36 42 48 54 Follow-up (mo) 60 Irbesartan Amlodipine Control Lewis EJ et al. N Engl J Med 2001;345:851-860. RRR 20% P =0.02 P =NS RRR 23% P =0.006 0 10 20 30 40 50 60 70
- 90. IDNT & RENAAL: Study Design SeCr, serum creatinine; ESRD, end-stage renal disease. † Lewis EJ et al. N Engl J Med. 2001;345:851-860. ‡ Brenner BM et al. N Engl J Med. 2001;345:861-869. Patients: 1,715 HTN patients with type 2 1,513 HTN patients with diabetes & nephropathy type 2 diabetes & nephropathy Treatment arms: irbesartan, amlodipine, losartan, placebo placebo Target BP: 135/85 mm Hg 140/90 mm Hg Adjunctive therapy: Permitted except ARBs, Permitted including ACE inhibitors, or CCBs CCBs, except ARBs or ACE inhibitors Primary outcome: Composite of doubling of Composite of doubling of SeCr, ESRD, or death SeCr, ESRD, or death Secondary outcomes: CV events CV events Mean Follow-up: 2.6 years 3.4 years RENAAL ‡ IDNT †
- 91. IDNT and RENAAL Trial Results Doubling of Creat, 16 ( P =0.02) 20 ( P =0.02) 23 ( P =0.006) -4 ( P =0.69) ESRD, or death Doubling of Creat 25 ( P =0.006) 33 ( P =0.003) 37 ( P< 0.001) -6 ( P =0.60) ESRD 28 ( P =0.002) 23 ( P =0.07) 23 ( P =0.07) 0 ( P =0.99) Death -2 ( P =0.88) 8 ( P =0.57) -4 ( P =0.8) 12 ( P =0.4) CV Morbidity 10 (P=0.26) 9 (P=0.4) -3 (P=0.79) 12 (P=0.29) & Mortality Losartan vs control Irbesartan vs control Irbesartan vs amlodipine Amlodipine vs control RRR (%) Comparison of Major Endpoints RENAAL IDNT Lewis EJ et al. N Engl J Med 2001;345:851-860. Brenner B et al. N Engl J Med 2001;345:861-869.
- 116. Antihypertensive Drugs Used in Pregnancy These agents* may be used with chronic hypertension (DBP > 100 mm Hg) or acute hypertension (DBP > 105 mm Hg). Central -agonists Methyldopa is the drug of choice. -blockers and - -blockers Atenolol, metoprolol, and labetalol appear safe and effective in late pregnancy. Calcium antagonists Potential synergism with magnesium sulfate may lead to precipitous hypotension. *Limited or no controlled trials in pregnant women.
- 117. Antihypertensive Drugs Used in Pregnancy (continued) These agents* may be used with chronic hypertension (DBP > 100 mm Hg) or acute hypertension (DBP > 105). Diuretics Diuretics are recommended for chronic hypertension if prescribed before gestation, but they are not recommended for preeclampsia. Direct vasodilators Hydralazine is the parenteral drug of choice based on its long history of safety and efficacy. *Limited or no controlled trials in pregnant women. ACE inhibitors and angiotensin II receptor blockers are contraindicated.
- 120. Combined Results of Five Randomized Trials of Antihypertensive Treatment in the Elderly Stroke 0 100 200 300 400 500 600 78 288 T T = Treatment C = Control = Fatal events 120 438 C CHD 208 346 T 279 438 C Vascular deaths Total numbers of individuals affected 383 T 494 C All other deaths 34% (6) 2P <0.0001 % (SD) reduction in odds 19% (7) 2P <0.05 23% (6) 2P <0.001 – 7% (8) 2P >0.5 344 362 T C
- 123. Mechanism of Action of Angiotensin II Receptor Antagonists Angiotensinogen Angiotensin I Angiotensin II AT 2 receptor AT 1 receptor Other AT receptors Bradykinin Inactive peptides Vasodilation Attenuate growth and disease progression ACE inhibitors Alternate pathways AIIRAs ? ?
- 130. IRMA 2: Mean Baseline Characteristics N Age (y) Male (%) BMI (kg/m 2 ) BP (mm Hg) HbA 1c (%) SeCr (mg/dL) Irbesartan 150 mg/d 195 58 66 29.9 153/90 7.3 1.0 Irbesartan 300 mg/d 194 57 71 30.0 153/91 7.1 1.1 Control 201 58 69 30.3 153/90 7.1 1.0 UAER (µg/min) 58 53 55 Duration of diabetes (y) 9.5 9.2 10.4 Control defined as placebo. BMI, body mass index; SeCr, serum creatinine; UAER, urinary albumin excretion rate; HbA 1c , glycosylated hemoglobin. Adapted from Parving H-H et al. N Engl J Med. 2001;345:870-878.
- 131. IRMA 2 Primary End Point: Time to Overt Proteinuria RRR, relative risk reduction. Control defined as placebo. * Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and dihydropyridine CCBs) could be added to all groups to help achieve target BP levels. Adapted from Parving H-H et al. N Engl J Med. 2001;345:870-878. Follow-up (mo) Control (n=201)* Irbesartan 150 mg/d (n=195)* Irbesartan 300 mg/d (n=194)* RRR=39% P =.08 RRR=70% P <.001 Patients (%) 0 3 6 12 18 22 24 0 5 10 15 20
- 132. IRMA 2: Normalization * of UAER UAER, urinary albumin excretion rate. Control defined as placebo. * Normoalbuminuria defined as UAER of <20 mg/min. † Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and dihydropyridine CCBs) could be added to all groups to help achieve target BP levels. Parving H-H et al. N Engl J Med. 2001;345:870-878. Control † (n=201) 150 mg/d † (n=195) 300 mg/d † (n=194) Irbesartan 24 34 21 P =.006 Patients (%) 35 45 40 30 25 20 15 10 5 0
- 133. IRMA 2: Adverse Events Cardiovascular events 18 (8.7) 1 14 (6.9) 2 9 (4.5) 1 Serious AE 47 (22.8) 1 32 (15.8) 2 30 (15.0) 2 Discontinuations due to AE 19 (9.2) 2 18 (8.9) 2 11 (5.5) 2 Control group* (n=201) Irbesartan 150 mg* (n=195) Irbesartan 300 mg* (n=194) No. of Adverse Events (%) Control defined as placebo. * Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and dihydropyridine CCBs) could be added to all groups to help achieve target BP levels. 1. Parving H-H, et al. N Engl J Med. 2001;345:870-878. 2. Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo, Inc.
- 135. IDNT: Study Design 1,715 patients with hypertension, type 2 diabetes, & proteinuria 900 mg/d Double-blind treatment Up to 5 weeks Screening/enrollment Control* Amlodipine* Minimum follow-up: approximately 2 years (average follow-up, 2.6 years) Irbesartan* Control defined as placebo. * Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and CCBs) could be added to all groups to help achieve target BP. Lewis EJ et al. N Engl J Med. 2001;345:851-860.
- 137. IDNT: Mean Baseline Demographics N Age (y) Male (%) Non-white (%) BMI (kg/m 2 ) History of CV disease (%) Retinopathy (%) Irbesartan 579 59 65 24 31.0 27 69 Amlodipine 567 59 63 31 30.9 30 64 Control 569 58 71 28 30.5 29 67 Control defined as placebo. BMI, body mass index. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. Duration of diabetes (y) 15 14 15
- 138. IDNT: Baseline Exam & Laboratory Characteristics Irbesartan Amlodipine Control SBP (mm Hg)* 160 159 158 Control defined as placebo. SeCr, serum creatinine; HbA 1c , glycosylated hemoglobin. * Mean. † Median. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. DBP (mm Hg)* 87 87 87 SeCr (mg/dL)* 1.67 1.65 1.69 Urine protein (g/24 h) † 2.9 2.9 2.9 HbA 1c (%)* 8.1 8.2 8.2
- 139. IDNT Primary End Point: Time to Doubling of SeCr, ESRD, or Death Control defined as placebo. SeCr, serum creatinine; ESRD, end-stage renal disease; RRR, relative risk reduction. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. Irbesartan (n=579) Amlodipine (n=565) Control (n=568) 0 6 12 18 24 30 36 42 48 54 Follow-up (mo) Patients (%) RRR=20% P =.02 P =NS RRR=23% P =.006 0 10 20 30 40 50 60 70
- 140. IDNT: Time to Doubling of SeCr Control defined as placebo. SeCr, serum creatinine; RRR, relative risk reduction. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. Patients (%) Follow-up (mo) Irbesartan (n=579) Amlodipine (n=567) Control (n=569) RRR=33% P =.003 P =NS RRR=37% P <.001 0 6 12 18 24 30 36 42 48 54 0 10 20 30 40 50 60 70
- 141. IDNT Secondary End Point: CV Events * No significant differences between groups. Control defined as placebo. * Defined as death from cardiovascular causes, nonfatal myocardial infarction, heart failure resulting in hospitalization, a permanent neurologic deficit caused by a cerebrovascular event, or lower limb amputation above the ankle. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:851-860. Control (n=569) Irbesartan (n=579) Amlodipine (n=567) 25.3 23.8 22.6 Patients (%) 0 10 20 30 5 15 25
- 142. IDNT: Adverse Events Early SeCr rise (n) 2 0 0 1 Discontinuations due to hyperkalemia [n (%)] 1 11 (1.9) 3 (0.5) 2 (0.4) Stopped study medicine [n (%)] 2 134 (23) 133 (23) 140 (25) SAEs/1000 days on drug (%) 2 2.0 2.5 2.3 Irbesartan Amlodipine Control No. of AEs AE, adverse event; SAE, serious adverse event. Control defined as placebo. 1. Lewis EJ et al. N Engl J Med. 2001;345:851-860. 2. Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo, Inc.
Hinweis der Redaktion
- 1
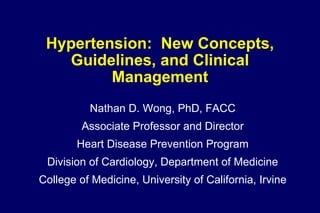
- Hypertension is an important contributing risk factor for morbidity and mortality from both cardiovascular (CV) and renal disease. Hypertension is one of the most significant contributing factors to the development of CV and renal disease. Complications of hypertension include coronary artery disease, congestive heart failure, stroke, renal disease (including end-stage renal disease), and peripheral vascular disease. These diseases account for significant disability, loss of productivity, and decreased quality of life for many Americans. National High Blood Pressure Education Program Working Group. National High Blood Pressure Education Program Working Group report on primary prevention of hypertension. Arch Intern Med. 1993;153:186-208.
- High-normal blood pressure (BP) is associated with an increased risk of major cardiovascular (CV) events defined as death due to CV disease; recognized myocardial infarction (MI), stroke, or congestive heart failure (CHF). Patients with high-normal BP (systolic BP of 130-139 mm Hg, diastolic BP of 85-89 mm Hg) at baseline were tracked for 10 years to determine the incidence of CV events at follow-up. The 6,859 patients in the study were initially free of hypertension and CV disease. High-normal BP was found to be associated with an increased risk of CV events. The 10-year incidence of CV events was 8% in men aged 35-64 years and 25% in men aged 65-90 years. Compared with optimal BP, high-normal BP was associated with a risk factor–adjusted hazard ratio for cardiovascular disease of 1.6. Vasan RS, Larson MG, Leip EP, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med . 2001;345:1291-1297.
- HOT Study: Significant Benefit From Intensive Treatment in the Diabetic Subgroup The Hypertension Optimal Treatment (HOT) study was a Prospective Randomized Open Blinded End-point (PROBE) study comparing the effect of 3 different target DBP levels ( 90 mm Hg, n=6264; 85 mm Hg, n=6264; 80 mm Hg, n=6262) in 18,790 patients with hypertension and DBP between 100 mm Hg and 105 mm Hg. Antihypertensive therapy started with the long-acting calcium channel blocker felodipine, with the addition of other agents according to a five-step regimen. Patients were followed for an average period of 3.8 years [Hansson et al, 1998]. The primary objective of HOT was to assess: 1) major cardiovascular events (nonfatal MI, nonfatal stroke, and cardiovascular death) for each of the target DBP groups during treatment, and 2) major cardiovascular events for the DBP achieved during treatment. In the overall HOT study population, intensive lowering of BP substantially reduced the incidence of major cardiovascular events including fatal and nonfatal MI, fatal and nonfatal stroke, and cardiovascular death, although the differences among the 3 groups did not reach statistical significance. The greatest risk reduction (30%) was observed in those who achieved a DBP of 83 mm Hg. Additional lowering of BP did not produce further reduction in events, but was not harmful; there was no evidence of a J-shaped curve for the relation of cardiovascular events with the achieved BPs in the HOT study. Among the 1501 patients with diabetes at baseline, there was a 51% reduction in the risk of major cardiovascular events in the group randomized to a DBP target of 80 mm Hg compared with that of the 90 mm Hg target group ( p =0.005 for trend). Cardiovascular mortality was also significantly lower in the 80 mm Hg target group than in each of the other target groups. Thus, intensive BP-lowering is particularly beneficial to patients with hypertension and diabetes mellitus.
- MRFIT showed that SBP is a stronger predictor of CHD mortality than DBP in men of all age groups except those 35 to 39 years of age. This study examined the relative risk of CHD mortality as a function of SBP and DBP in 353,340 screened men who were followed for an average of 12 years. A strong, graded relationship was evident between SBP at every level >110 mm Hg and death due to CHD. Differences in CHD-related mortality at various DBP levels were relatively small. 24 Results from MRFIT strongly support the conclusion that SBP is a better indicator of increased CHD risk than DBP. This conclusion prompted the recent recommendation by the Coordinating Committee, National High Blood Pressure Education Program, National Heart, Lung, and Blood Institute, that SBP should “…become the principal clinical end point for the detection, evaluation, and treatment of hypertension, especially in middle-aged and older Americans.” 26
- Numerous epidemiologic studies have shown that elevated SBP is an independent risk factor for cardiovascular morbidity and mortality and have supported the conclusion that, more than high DBP, elevated SBP increases those risks. 20-24 The Framingham Study indicated significantly increased risk of coronary disease, stroke, cardiac failure, and peripheral vascular disease in individuals 65 to 94 years old with elevated SBP. In all cases, the risks with elevated DBP were lower than those with elevated SBP. 20 A study of 11,912 hypertensive US veterans (5730 African American and 6182 nonblack; mean age, 52.5 years) showed significant and increasing risk of end-stage renal disease with rising SBP.21 The risk ratio (relative to that in the normotensive cohort) was 2.8 for SBP of 165 to 180 mm Hg and increased to 7.6 for SBP >180 mm Hg. In the Multiple Risk Factor Intervention Trial (MRFIT) of 332,554 screened men (35 to 57 years of age), the relative risks of end-stage renal disease were 6.0 for SBP of 160 to 179 mm Hg, 11.2 for SBP of 180 to 209 mm Hg, and 22.1 for SBP 210 mm Hg. 22 Elevated SBP also increases risk of stroke. A prospective, population-based study of 6621 individuals 50 years of age indicated relative risks of 2.7 for men and 3.0 for women versus normotensives. 23 Men with high SBP also had an increased risk of MI. MRFIT showed further that the risk of mortality from coronary heart disease (CHD) increases progressively with increased SBP. The adjusted relative risk rate was 1.8 for individuals with high-normal SBP (132–141 mm Hg) and 3.0 for hypertensive individuals (SBP 142 mm Hg). 24
- Two large, long-term, placebo-controlled clinical trials have demonstrated significant reductions in cardiovascular risk for older patients with elevated SBP. The Systolic Hypertension in the Elderly (SHEP) and the Systolic Hypertension in Europe (Syst-Eur) trials evaluated the efficacy of antihypertensive therapy in reducing cardiovascular risk in older patients with elevated SBP. 27,28 The designs and results of each of these landmark studies are reviewed in the following slides.
- SHEP demonstrated that effective antihypertensive therapy in older patients with elevated SBP significantly reduced the risk of stroke. 27 The 5-year average blood pressure was 143/68 mm Hg for patients receiving active treatment versus 155/72 mm Hg for patients receiving placebo. The 5-year incidence of total stroke was 5.2 per 100 participants with active treatment compared with 8.2 per 100 with placebo ( P =.0003). Reductions occurred in relative risk of nonfatal MI plus coronary death (to 0.73) and in major cardiovascular events (0.68). Relative risk of death from all causes was 0.87 in the patients who received antihypertensive therapy.
- Syst-Eur investigated whether antihypertensive treatment reduced cardiovascular complications in older patients with high SBP. 28-30 Men and women 60 years of age with SBP 160 to 219 mm Hg and DBP <95 mm Hg were randomly assigned to active treatment with nitrendipine (n=2398), with the possible addition of enalapril and hydrochlorothiazide, or to placebo (n=2297). Median follow-up was 2 years.
- Syst-Eur demonstrated that treatment of systolic hypertension with a dihydropyridine calcium-channel antagonist (nitrendipine) significantly reduced SBP and the risk of several cardiovascular endpoints. 28 At a median of 2 years of follow-up, sitting blood pressure had fallen by 13/2 mm Hg in the placebo group versus 23/7 mm Hg in the active-treatment group. Active treatment reduced the total rate of stroke by 42% ( P =.003) and of nonfatal stroke by 44% ( P =.007), as well as all cardiac endpoints, including sudden death (26%; P =.03). Nonfatal cardiac endpoints decreased by 33% ( P =.03) and all fatal and nonfatal cardiovascular endpoints by 31% ( P <.001). Cardiovascular mortality was slightly lower (27%) in the patients who received antihypertensive therapy ( P =.07), but all-cause mortality was not significantly decreased (14%; P =.22).
- The Antihypertensive and Lipid‑Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), a randomized, double‑blind, multi‑center, clinical trial sponsored by the National Heart Lung and Blood Institute (NHLBI), was designed to determine whether the occurrence of fatal CHD or nonfatal myocardial infarction (MI) is lower for high‑risk hypertensive patients treated with a CCB (represented by amlodipine), an ACEI (represented by lisinopril), or an alpha blocker (represented by doxazosin), each compared with diuretic treatment (represented by chlorthalidone). 42,418 high-risk hypertensive patients age 55 and older were randomized.
- No significant difference was observed between amlodipine (the red line) and chlorthalidone (the blue line) for the primary outcome. The relative risk for amlodipine compared to chlorthalidone was 0.98, with a 95% confidence interval of 0.90-1.07. Also, no significant difference was observed between lisinopril (the green line) and chlorthalidone for the primary outcome. The relative risk was 0.99, with a 95% confidence interval of 0.91-1.08.
- There was no difference for stroke between the amlodipine and chlorthalidone groups. The lisinopril group had a 15% higher risk for stroke.
- The amlodipine group had a 38% higher risk of HF (p<.001) with a 6-year absolute risk difference of 2.5% . The lisinopril group had a 19% higher risk of HF (p < .001) .
- Because of the superiority of thiazide-type diuretics in preventing one or more major forms of CVD and their lower cost, they should be the drugs of choice for first-step antihypertensive drug therapy .
- Major hypertension trials, using a variety of antihypertensive agents, have demonstrated that effective blood pressure control significantly reduces cardiovascular (CV) morbidity and mortality. Until recently (LIFE study comparing the ARB losartan with the beta blocker atenolol), there has been no evidence that any one class of antihypertensive agents consistently provides better CV morbidity and mortality reductions than another. The Blood Pressure Lowering Treatment Trialists’ Collaboration 1 included 5 trials comparing calcium channel blocker (CCB)–based regimens with diuretic-based and beta blocker–based regimens, involving more than 23,000 patients: the Verapamil in Hypertension and Atherosclerosis Study (VHAS) 2,3 ; the Swedish Trial in Old Patients with Hypertension-2 (STOP-Hypertension-2) 4 ; the National Intervention Cooperative Study in Elderly Hypertensives (NICS-EH) 5 ; the Nordic Diltiazem (NORDIL) study 6 ; and the International Nifedipine GITS Study: Intervention as a Goal in Hypertension Treatment (INSIGHT). 7 Among patients assigned to CCB therapy, there was a significant 13% reduction in the risk of stroke compared with diuretic-based and beta blocker–based therapy. Additionally, there was a 12% greater risk of coronary-heart-disease events of borderline significance among those patients assigned CCB-based therapy. No significant differences were seen between randomized groups for major CV events, CV death, or total mortality. Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Lancet. 2000;356:1955-1964. Agabiti Rosei E, Dal Palù C, Leonetti G, Magnani B, Pessina A, Zanchetti A, on behalf of the VHAS Investigators. Clinical results of the Verapamil in Hypertension and Atherosclerosis Study. J Hypertens. 1997;15:1337-1344. Zanchetti A, Agabiti Rosei E, Dal Palù C, et al. The Verapamil in Hypertension and Atherosclerosis Study (VHAS): results of long-term randomized treatment with either verapamil or chlorthalidone on carotid intima-media thickness. J Hypertens. 1998;16:1667-1676. Hansson L, Lindholm LH, Ekbom T, et al, for the STOP-Hypertension-2 study group. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity. The Swedish Trial in Old Patients with Hypertension-2 study. Lancet. 1999;354:1751-1756. National Intervention Cooperative Study in Elderly Hypertensives Study Group (NICS-EH). Randomized double-blind comparison of a calcium antagonist and a diuretic in elderly hypertensives. Hypertension. 1999;34:1129-1133.
- Renin-angiotensin system blockade is beneficial in a broad range of patients at high risk for cardiovascular (CV) events. The Heart Outcomes Prevention Evaluation (HOPE) study evaluated the benefits of the angiotensin-converting enzyme inhibitor ramipril and vitamin E in 9,297 patients, 55 years of age, at high risk for CV events. The study had a double-blind, randomized, placebo-controlled, 2 x 2 factorial design. Patients with evidence of vascular disease (history of coronary artery disease, stroke, or peripheral vascular disease), or diabetes plus one other CV risk factor (eg, hypertension, elevated total cholesterol, low levels of high-density lipoprotein cholesterol, cigarette smoking, or documented microalbuminuria), without heart failure or low ejection fraction, were randomly assigned to receive either ramipril 10 mg/d, vitamin E, or matching placebo for a mean of 5 years. The primary end point was a composite of myocardial infarction (MI), stroke, and CV death. Baseline characteristics included a mean age of 66 years and a mean blood pressure of 139/79 mm Hg. At baseline, 80% of the patients had a history of coronary artery disease and 53% had a prior MI; 47% had been diagnosed with hypertension, 38% with diabetes, and 21% with microalbuminuria. None of the patients had overt diabetic nephropathy. Results showed that although vitamin E provided no CV benefit, ramipril significantly reduced the risk of the composite primary end point by 22% ( P <.001). Treatment with ramipril significantly reduced the risk of death from CV causes ( P <.001), MI ( P <.001), stroke ( P <.001), total mortality ( P =.005), revascularization procedures ( P =.002), heart failure ( P <.001), and complications related to diabetes ( P =.03). The beneficial effect of treatment with ramipril was consistently observed among these predefined subgroups: women and men, with or without diabetes, CV disease, hypertension, and microalbuminuria; older than 65; and younger than 65. The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med . 2000;342:145-153.
- Major hypertension trials, using a variety of antihypertensive agents, have demonstrated that effective blood pressure control significantly reduces cardiovascular (CV) morbidity and mortality. Until recently (LIFE study comparing the ARB losartan with the beta blocker atenolol), there has been no evidence that any one class of antihypertensive agents consistently provides better CV morbidity and mortality reductions than another. The Blood Pressure Lowering Treatment Trialists’ Collaboration included 3 trials comparing ACE-inhibitor-based therapy with diuretic or beta blocker-based therapy: CAPPP, UKPDS-HDS, and STOP-2. There were no detectable differences between randomized groups in the risks of any of the outcomes studied (all P >.1). Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Lancet. 2000;356:1955-1964. Hansson L, Lindholm L, Niskanen L, et al. Effect of angiotensin converting enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trial. Lancet 1999; 353:611-616. UK Prospective Diabetes Study Group. Efficacy of atenolol and captopril in reducing risk of macrovascular complications in type 2 diabetes: UKPDS 39. BMJ. 1998; 317:713-720. Hansson L, Lindholm LH, Ekbom T, et al, for the STOP-Hypertension-2 study group. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity. The Swedish Trial in Old Patients with Hypertension-2 study. Lancet. 1999;354:1751-1756.
- It is well established that blood pressure reduction will reduce hypertensive LV hypertrophy. However, experimental evidence suggests that various classes of antihypertensive agents may have different effects on LV mass. Most notably, drugs acting as direct vasodilators seem to provide little benefit. A meta-analysis of all randomized, controlled echocardiographic trials in humans with a duration of six months or more indicate that reductions in LV mass may be greater with angiotensin-converting enzyme (ACE) inhibitors (13%) than with beta blockers, calcium antagonists or diuretics (6%, 9% and 7%, respectively). 1 These findings confirm earlier work by Dahlöf et al 2 , which found a 17% reduction in LV mass with ACE inhibitors compared with reductions of 10% for diuretics, 9% for beta blockers, and 8% for calcium antagonists. These findings suggest that both hemodynamic factors and mechanisms related to the RAS are involved in the development, maintenance and regression of LV hypertrophy. Schmieder RE, Martus P, Klinbeil A. Reversal of left ventricular hypertrophy in essential hypertension. A meta-analysis of randomized double-blind studies. JAMA. 1996;275:1507-1513. Dahlöf B, Pennert K, Hansson L. Reversal of left ventricular hypertrophy in hypertensive patients. A metaanalysis of 109 treatment studies. Am J Hypertens. 1992;5:95-110 .
- In essential hypertension, a reduction in left ventricular (LV) mass during treatment is a favorable prognostic marker that predicts a smaller risk for subsequent cardiovascular morbid events. Increased LV mass predicts an adverse outcome in patients with essential hypertension. A study was designed to determine the relation between changes in LV mass during antihypertensive treatment and subsequent prognosis. Procedures including echocardiography and 24-hour ambulatory blood pressure monitoring were performed in 430 patients with essential hypertension before therapy and after 1,217 patient-years. The prevalence of LV hypertrophy at echocardiography (LV mass >125.0 g/m 2 ) was 26%, and the event rate in this group was higher (3.9 events per 100 patient-years) than among patients with normal LV mass (1.6 events per 100 patient-years). This slide shows event-free survival curves in the 2 groups. There were 15 events (1.78 per 100 patient-years) among the 285 patients who had a decrease in LV mass from baseline (regressors) to follow-up visit, and 16 events (3.03 per 100 person-years) in the patients who had no change or an increase in LV mass (nonregressors) ( P =.029, log-rank test). Verdecchia P, Schillaci G, Borgioni C, et al. Prognostic significance of serial changes in left ventricular mass in essential hypertension. Circulation. 1998;97:48-54.
- The trial began with a 4-week, single-blind placebo lead-in period, after which patients were randomized to irbesartan 150 mg or atenolol 50 mg. Doses of the study drugs were doubled at week 6 or anytime thereafter for SeDBP 90 mm Hg. At weeks 12 and 18, once subjects were titrated to the higher dose of the study medications, adjunctive therapy with hydrochlorothiazide (12.5 mg titrated to 25 mg as needed) was added for SeDBP 90 mm Hg. At week 24 or anytime thereafter, felodipine (5 mg titrated to 10 mg as needed) could be added for SeDBP 90 mm Hg. Blood pressure, echocardiography and neurohormone levels were assessed at the start of the double-blind period and at weeks 12, 24 and 48. Malmqvist K, Kahan T, Edner M, et al. Regression of left ventricular hypertrophy in human hypertension with irbesartan. J Hypertens 2001;19:1167-1176. Malmqvist K, Kahan T, Edner M, Held C, Osbakken M. Rate and extent of left ventricular hypertrophy regression: A comparison of angiotensin II blockade with irbesartan and beta-blockade. J Am Coll Cardiol. 1998;31:212A.
- Change from baseline in SeDBP was significant at all time points in both treatment groups ( P <.001). There were no statistically significant differences between irbesartan and atenolol in SeDBP except at week 12. Reductions in SeDBP from baseline with irbesartan were 9.0, 12.2 and 17.8 mm Hg at weeks 12, 24 and 48, respectively. Reductions in SeDBP with atenolol were 11.2, 13.4 and 15.5 mm Hg at weeks 12, 24 and 48, respectively. Malmqvist K, Kahan T, Edner M, et al. Regression of left ventricular hypertrophy in human hypertension with irbesartan. J Hypertens 2001;19:1167-1176. Malmqvist K, Kahan T, Edner M, Held C, Osbakken M. Rate and extent of left ventricular hypertrophy regression: A comparison of angiotensin II blockade with irbesartan and beta-blockade. J Am Coll Cardiol. 1998;31:212A.
- There was a progressive reduction in LV mass index in both treatment groups. Reductions from baseline in LVMI were significant at weeks 12, 24 and 48 in the irbesartan group; and was reduced at weeks 24 ands 48 in the atenolol group. Reductions tended to occur sooner with irbesartan than with atenolol. The reduction in LVMI at week 48 was significantly greater in the irbesartan group compared to the atenolol group at week 48 ( p =.024). Moreover, reductions in LVMI were numerically greater with irbesartan than with atenolol at all time points. Malmqvist K, Kahan T, Edner M, et al. Regression of left ventricular hypertrophy in human hypertension with irbesartan. J Hypertens 2001;19:1167-1176. Malmqvist K, Kahan T, Edner M, Held C, Osbakken M. Rate and extent of left ventricular hypertrophy regression: A comparison of angiotensin II blockade with irbesartan and beta-blockade. J Am Coll Cardiol. 1998;31:212A.
- L II FE was a prospective, multicentre, double-blind, double-dummy, randomised, active-controlled, parallel group study. After a 2-week single-blind placebo run-in period, patients entered a minimum 4-year active treatment period. Active treatment continued for 4 years after the last patient was enrolled and until 1,040 patients experienced a primary cardiovascular event. Antihypertensive therapy was titrated as shown in the figure to achieve a goal blood pressure of 140 / 90 mmHg or less. Patients initially received losartan 50 mg or atenolol 50 mg. After 2 months, HCTZ 12.5 mg was added if blood pressure was not at, or below, goal blood pressure. After 4 months, the dose of losartan or atenolol was doubled to 100 mg plus HCTZ 12.5 mg if blood pressure was still inadequately controlled. At month 6, additional open-label antihypertensive medication including upward titration of HCTZ could be added in order to reach goal blood pressure. If blood pressure was 160 / 95 mmHg, upward titration with additional open-label therapy was mandatory.
- Dahlöf B, Dever ë ux RB, Kjeldsen SE, et al, for the UFE study group. Cardiovascular morbidity and mortality in the losartan intervention for endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet . 2002;359:995-1003.
- Dahlöf B, Dever ë ux RB, Kjeldsen SE, et al, for the UFE study group. Cardiovascular morbidity and mortality in the losartan intervention for endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet . 2002;359:995-1003.
- Association of Systolic BP and Cardiovascular Death in Type 2 Diabetes In the large cohort of men screened for Multiple Risk Factor Intervention Trial (MRFIT), the relationships of SBP and other cardiovascular risk factors to cardiovascular mortality were compared in men with diabetes (n=5163) and without diabetes (n=342,815). The absolute risk of cardiovascular death was 3- times higher for men with diabetes than for those without diabetes, after adjustment for age, race, income, serum cholesterol, SBP, and cigarette smoking ( p <0.0001). Systolic blood pressure was positively related to the risk of cardiovascular death, with a significant trend in both nondiabetic and diabetic subjects ( p <0.001). At every level of SBP, cardiovascular death was much greater for men with diabetes than for men without diabetes. Moreover, with higher SBP levels, the cardiovascular mortality rate increased more steeply among those with diabetes than among those without diabetes. Thus, the higher the SBP, the greater the absolute excess risk for patients with diabetes, indicating a greater potential for prevention of cardiovascular death among patients with diabetes by control of elevated BP [Stamler et al, 1993].
- United Kingdom Prospective Diabetes Study (UKPDS): Results The United Kingdom Prospective Diabetes Study (UKPDS) was a multicenter, prospective, randomized, interventional trial. The primary goal was to determine the effect of intensive blood glucose control (fasting plasma glucose <6 mmol/L) with either sulfonylurea or insulin treatment versus conventional blood glucose treatment with diet on macrovascular and microvascular complications in 3867 newly-diagnosed patients with type 2 diabetes. Over 10 years, median HbA1c was 7.0% in the “intensive” group compared with 7.9% in the conventional treatment group, an 11% reduction. This resulted in a 12% reduction in the risk of any diabetes-related endpoint ( p =0.029), mainly due to a 25% risk reduction in microvascular endpoints ( p =0.01), including the need for retinal photocoagulation [UK Prospective Diabetes Study Group 33, 1998]. Embedded within the UKPDS was a randomized, controlled trial comparing tight BP control using a captopril- or atenolol-based regimen (aiming at a BP <150/85 mm Hg) with less tight BP control (avoiding treatment with ACE inhibitors or beta blockers and aiming at a BP <180/105 mm Hg) on the development of macrovascular and microvascular complications in 1148 hypertensive patients with type 2 diabetes. During the median follow-up of 8.4 years, the mean BP was significantly reduced in the group with tight BP control (144/82 mm Hg) compared with the group with less tight BP control (154/87 mm Hg), p <0.0001, representing a 10/5mmHg difference. Tight BP control reduced the risk of developing any endpoint related to diabetes by 24% compared with less tight BP control ( p =0.005). Compared to less tight BP control, tight BP control also significantly reduced the risk of diabetes-related mortality, two thirds of which was due to cardiovascular disease, by 32% ( p =0.019), the risk of microvascular disease by 37% ( p =0.009), and the risk of stroke by 44% ( p =0.013).
- Type 2 diabetes is the most common cause of end-stage renal disease. Costs/patient-year and mortality rates are higher for diabetic patients than for nondiabetic patients with ESRD. Diabetes has become the most common single cause of ESRD, defined by the need for dialysis or transplantation, accounting for over 44% of all new cases of ESRD reported in the United States. 1 Type 2 diabetes accounts for the majority of diabetic patients with ESRD. 2,3 The dramatic increase in numbers of patients with type 2 diabetic nephropathy reflects both an increase in the prevalence of diabetes in the general population as well as improved survival of patients with type 2 diabetes in recent years. With a reduction in mortality from cardiovascular disease, patients with type 2 diabetes are now surviving long enough to develop diabetic nephropathy and ESRD. 2,3 Among patients who have had type 2 diabetes for at least 25 years, the prevalence of nephropathy is 57%. 4 The financial implications of ESRD are staggering. The average cost of hemodialysis in the United States is $52,000/year, and total spending for ESRD by all payers in the United States was estimated to be $15.64 billion in 1997. 1 The cost per patient-year at risk among all ESRD patients was higher for patients with diabetes ($51,000) than for those without diabetes ($39,000). 5 USRDS Coordinating Center. USRDS 1999 Annual Data Report . The Kidney Epidemiology and Cost Center of the University of Michigan; 1999. NIH Contract no. NO1-DK-3-2202. American Diabetes Association. Diabetic Nephropathy: clinical practice recommendations. Diabetes Care . 2001;24(suppl 1):S69-S72. Ritz E, Stefanski A. Diabetic nephropathy in type II diabetes. Am J Kidney Dis . 1996;27:167-194. Bakris GL, Williams M, Dworkin L, et al, for the National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Preserving renal function in adults with hypertension and diabetes: a consensus approach. Am J Kidney Dis . 2000;36:646-661. Ruggenenti P, Gambara V, Perna A, Bertani T, Remuzzi G. The nephropathy of non-insulin-dependent diabetes: predictors of outcome relative to diverse patterns of renal injury. J Am Soc Nephrol. 1998;9:2336-2343.
- The average survival time for patients with ESRD is 4 to 5 years. 1 The mortality rate among patients with diabetes and ESRD is approximately 1.5 to 2.5 times greater than that among those with ESRD who do not have diabetes, and < 20% of ESRD patients with diabetes survive for 5 years after initiation of dialysis. 1 Cardiovascular disease is the most common cause of death among diabetic patients with ESRD. 2,3 Koch M, Thomas B, Tschöpe W, Ritz E. Survival and predictors of death in dialysed diabetic patients. Diabetologia . 1993;36:1113-1117. Bakris GL. Progression of diabetic nephropathy. A focus on arterial pressure level and methods of reduction. Diabetes Res Clin Pract. 1998;39(suppl):S35-S42. Grundy SM, Benjamin IJ, Burke GL, et al. Diabetes and cardiovascular disease. A statement for healthcare professionals from the American Heart Association. Circulation . 1999;100:1134-1146.
- This figure illustrates the relationship between achieved blood pressure control and declines in GFR in clinical trials of diabetic and nondiabetic renal disease. Lower levels of blood pressure (BP) result in slower rates of decline in renal function. Note: Hypertension substantially contributes to cardiovascular morbidity and mortality in people with diabetes. Diabetes is the most common cause of end-stage renal disease in the United States. The recent National Kidney Foundation consensus report on preserving renal function in adults with hypertension and diabetes updated the previous recommendations, with a focus on level of BP control, proteinuria reduction, and therapeutic approaches to achieve these target levels. 1 The previous goal of 130/85 mm Hg in patients with diabetes 2 has been further lowered to a suggested target of 130/80 mm Hg. Bakris GL, Williams M, Dworkin L, et al, for the National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Preserving renal function in adults with hypertension and diabetes: a consensus approach. Am J Kidney Dis. 2000;36:646-661. Keane WF, Eknoyan G., for the Committee Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis. 1999;33:1004-1010.
- Microalbuminuria is a strong predictor of all-cause mortality and cardiovascular (CV) morbidity and mortality in type 2 diabetes. The impact of microalbuminuria on mortality was investigated in a 10-year follow-up study of 503 predominantly type 2 diabetic patients. 1 Two hundred sixty five of the patients died, and 58% of the deaths were caused by CV disease and stroke. Compared with patients with normal morning urinary albumin concentration (UAC 15 µg/min), the relative risk of death for patients with UAC between 16 µg/min and 40 µg/min and for patients with UAC between 41 µg/min and 200 µg/min was greater. Thus, the probability of survival decreased with increasing levels of UAC within the microalbuminuria range. Microalbuminuria was demonstrated to be a major CV risk factor; even a minor increase in UAC was associated with increased mortality. A meta-analysis of prospective trials involving patients with type 2 diabetes 2 found that microalbuminuria was associated with an increased odds ratio for all-cause mortality (2.4) and CV morbidity or mortality (2.0). The presence of microalbuminuria may reflect a generalized defect in vascular permeability leading to atherogenesis. Schmitz A, Vaeth M. Microalbuminuria: a major risk factor in non-insulin-dependent diabetes: a 10-year follow-up study of 503 patients. Diabetes Med. 1988;5:126-134. Dinneen SF, Gerstein HC. The association of microalbuminuria and mortality in non-insulin-dependent diabetes mellitus. Arch Intern Med. 1997;157:1413-1418.
- Overt proteinuria significantly predicts mortality, stroke, and other atherosclerotic events. In a 7-year follow-up of 1,056 patients with type 2 diabetes in Finland, overt proteinuria significantly predicted mortality and the incidence of stroke and other atherosclerotic vascular disease events, even after adjustments for hypertension and other cardiovascular (CV) risk factors were made. Based on urinary protein concentration from the morning spot urine at baseline, patients were stratified into 3 categories: no proteinuria (UPC<150 mg/L), borderline proteinuria (UPC 150-300 mg/L), and overt proteinuria (UPC>300 mg/L). Both all-cause mortality and CVD mortality were significantly higher in patients with overt proteinuria than in patients without proteinuria. The association between the different degrees of proteinuria and the risk of stroke and coronary heart disease events was stepwise ( P <.001 for trend). Miettinen H, Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Proteinuria predicts stroke and other atherosclerotic vascular disease events in nondiabetic and non-insulin-dependent diabetic subjects. Stroke. 1996;27:2033-2039.
- Intensive blood pressure (BP) control reduces the risk of diabetes-related death, stroke, and microvascular end points in patients with diabetes and hypertension. The United Kingdom Prospective Diabetes Study (UKPDS-38) compared the effect of tight BP control with less tight BP control in 1,148 hypertensive patients with type 2 diabetes over a median follow-up of 8.4 years. The tight BP control group was assigned a BP target of <150/85 mm Hg and were treated with antihypertensives (captopril or atenolol) and diet. The less tight BP control group had a BP target of <180/105 mm Hg and was treated with diet alone. Additional antihypertensive agents could be added to either group if the control criteria were not met. Tight BP control reduced the risk of developing any end point related to diabetes by 24% compared with less tight BP control ( P =.005). Compared with less tight BP control, tight BP control specifically reduced the risk of diabetes-related mortality (two thirds of diabetes-related mortality was due to cardiovascular disease) by 32% ( P =.019); the risk of stroke by 44% ( P =.013); the risk of microvascular disease by 37% ( P =.009); and the risk of myocardial infarction by 21% ( P =.13). UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS-38. BMJ. 1998;317:703-713.
- Intensive lowering of diastolic blood pressure (DBP) decreases the risk of major cardiovascular (CV) events. The Hypertension Optimal Treatment (HOT) study was a Prospective, Randomized, Open with Blinded End point (PROBE) trial comparing the effect of 3 different target DBP levels ( 90 mm Hg, n=6,264; 85 mm Hg, n=6,264; 80 mm Hg, n=6,262) in 18,790 patients with hypertension and DBP between 100 mm Hg and 115 mm Hg (mean 105 mm Hg). The PROBE design has been proposed as a novel, simplified study design for medical intervention trials that more closely mimics actual clinical practice compared with double-blind, randomized, controlled trials. In the HOT study, antihypertensive therapy was started with the long-acting calcium channel blocker felodipine, with other agents added according to a 5-step regimen. Patients were followed for an average period of 3.8 years. The primary objectives of the study were to assess major CV events (fatal and nonfatal myocardial infarction [MI], fatal and nonfatal stroke, and all other CV death), the association between each of the 3 target DBP levels during antihypertensive treatment, and the DBP achieved during treatment. Results indicated that in the overall HOT study population, intensive lowering of blood pressure (BP) substantially reduced the incidence of major CV events, including fatal and nonfatal MI, fatal and nonfatal stroke, and CV death, although the differences among the 3 groups did not reach statistical significance. The greatest risk reduction (30%) was observed in those who achieved a DBP of 83 mm Hg. Additional lowering of BP did not produce further reduction in events but was not harmful; there was no evidence of a J-shaped curve for the relation between CV events and achieved BPs. Among the 1,501 patients with diabetes at baseline, there was a 51% reduction in the risk of major CV events in the group randomized to a DBP target of 80 mm Hg compared with patients whose target was 90 mm Hg ( P =.005 for trend). CV mortality was also significantly lower in the 80 mm Hg target group than in each of the other target groups. Thus, intensive BP-lowering was particularly beneficial for patients with both hypertension and diabetes mellitus. Hansson L, Zanchetti A, Carruthers SG, et al, for the HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet. 1998;351:1755-1762.
- Angiotensin-converting enzyme (ACE) inhibition protects against deterioration in renal function in type 1 diabetic nephropathy to a greater degree than would be expected from blood pressure (BP) reduction alone. A randomized, controlled trial compared the ACE inhibitor captopril with placebo in 409 patients with type 1 diabetes, diabetic retinopathy, proteinuria 500 mg/d, and serum creatinine (SeCr) concentrations 2.5 mg/dL. Median follow-up was 3 years. The primary end point was a doubling of the baseline SeCr concentration. Doubling of SeCr from baseline corresponds to an almost 50% reduction in renal function. Results showed that captopril slowed the progression of diabetic nephropathy, reducing the risk of doubling of SeCr by 48% ( P =.007). Captopril was also associated with a 50% risk reduction in the composite end point of death, need for dialysis, or transplantation ( P =.006). Lewis EJ, Hunsicker LG, Bain RP, Rohde RD, for the Collaborative Study Group. The effect of angiotensin-converting–enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993;329:1456-1462.
- The average trough blood pressure (BP) was similar in all 3 treatment groups throughout the study. Trough BP was similar in the 3 groups at baseline. The average trough BP throughout the study was 144/83, 143/83, and 141/83 mm Hg in the placebo, irbesartan 150-mg, and irbesartan 300-mg groups, respectively ( P =.004 for the comparison of SBP between the combined irbesartan groups and the placebo group). The average trough mean arterial BP during the study was 103 mm Hg in the placebo and irbesartan 150-mg groups, and 102 mm Hg in the irbesartan 300-mg group ( P =.005 for the comparison between the 300-mg group and the placebo group). Fifty-six percent of the patients in the control group were receiving adjunctive antihypertensive therapy at the end of the 2-year follow-up, compared with 45% in the irbesartan 150-mg group and 43% in the irbesartan 300-mg group ( P =.03, irbesartan 150 mg vs placebo; P =.01, irbesartan 300 mg vs placebo). Nondihydropyridine calcium channel blockers, diuretics, and beta blockers were the most commonly used adjunctive antihypertensive medications in all three arms. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- The event rates for the primary endpoint are approximately 15%, 10%, and 5% in the control (placebo in addition to other nonexcluded antihypertensive therapies), irbesartan 150 mg, and irbesartan 300 mg groups, respectively. 1 This corresponds to relative risk reductions of 39% for irbesartan 150 mg vs. the control group (p=0.08), and 70% for irbesartan 300 mg vs. the control group (p<0.001). Two important secondary endpoints in IRMA 2 include change in overnight urinary albumin excretion rate (AER) and change in creatinine clearance. AER was reduced in the two irbesartan groups throughout the study (-24% and -38% at 24 months, compared with baseline, in the irbesartan 150 mg and 300 mg groups, respectively). AER remained unchanged in the control group (-2% at 24 months compared with baseline), p<0.001 for the comparison between the control group and the two irbesartan groups combined. Creatinine clearance remained in the normal range in all three groups throughout the study. Additionally, regression to normoalbuminuria (< 20 g/min, or < 30 mg/day) at the last visit was more frequent in the patients treated with irbesartan 300 mg than in the control (placebo in addition to other nonexcluded antihypertensive therapies) group (34% vs. 21%, respectively, p=0.006). 1 1 Parving et al, 2001a.
- Irbesartan effectively lowered blood pressure, achieving the same level of blood pressure as that observed in the amlodipine group. 1 The average blood pressure improved over the course of the trial in all 3 arms, averaging 140/77, 141/77, and 144/80 mm Hg at visits after baseline in the irbesartan, amlodipine, and control (placebo in addition to other nonexcluded antihypertensive therapies) groups, respectively. 1 The average dose of irbesartan used in the irbesartan group was 269 mg once daily; the average dose of amlodipine used in the amlodipine group was 9.1 mg once daily. 2 The distribution of classes of nonstudy agents used to help lower blood pressure was similar in the 3 treatment groups and included primarily diuretics, beta blockers, peripheral alpha blockers, and central alpha- 2 agonists. An average of 3.3 nonstudy antihypertensive drugs were used in the control group, and an average of 3.0 nonstudy antihypertensive drugs were used in the irbesartan and amlodipine groups. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860. Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo Inc.
- IDNT is a positive study, demonstrating a 20% risk reduction for the primary endpoint vs. the control group, and a 23% risk reduction vs. the amlodipine group, independent of the effects of irbesartan on systemic blood pressure. The irbesartan group in IDNT demonstrates a 20% RRR vs. the control group (placebo in addition to other nonexcluded antihypertensive therapies) for the primary endpoint of doubling of serum creatinine, development of end-stage renal disease (ESRD), or death from any cause (p=0.02), and a 23% RRR vs. the amlodipine group (p=0.006). 1 The Kaplan-Meier curve for irbesartan continues to diverge away from the control and amlodipine curves throughout the course of the study. No significant difference is observed between the control and amlodipine groups. The better outcomes among patients in the irbesartan group could not be explained by differences in achieved blood pressure. Although the mean arterial blood pressure (MAP) in the irbesartan group was the same as that in the amlodipine group, there was a significant difference in the primary endpoint in favor of irbesartan. Furthermore, correction for achieved MAP at quarterly visits during follow-up in a time-dependent proportional hazards analysis gave results similar to those of the primary analysis. After adjustment for blood pressure, the benefits of irbesartan are still present: RRR of 19% for irbesartan vs. the control group (p=0.03); RRR of 24% for irbesartan vs. the amlodipine group (p=0.005). 1 Lewis et al, 2001.
- Depicted are the study designs for the Irbesartan Diabetic Nephropathy Trial (IDNT) 1 and the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) Study. 2 Both IDNT and RENAAL were multicenter, double-blind, randomized, placebo-controlled studies designed to evaluate the renoprotective effects of an angiotensin II receptor blocker in patients with type 2 diabetes and nephropathy. The primary outcome for both IDNT and RENAAL was a composite of doubling of baseline serum creatinine, end-stage renal disease, or death. Some differences in the study designs included an additional treatment arm in the IDNT trial (amlodipine) and a more stringent blood pressure (BP) goal of 135/85 mm Hg in IDNT, vs a BP goal of 140/90 mm Hg in RENAAL. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860. Brenner BM, Cooper ME, de Zeeuw D, et al, for the RENAAL Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861-869.
- Results from RENAAL are comparable to those from IDNT, with similar renal and cardiovascular effects. Only the PRIME program with irbesartan evaluates morbidity and/or mortality in patients with type 2 diabetes across the continuum of early and late stages of diabetic renal disease. RENAAL was designed to determine whether the AIIRA losartan would slow the progression of type 2 diabetic nephropathy beyond that which could be attributed to reduction of blood pressure alone. This is a prospective, randomized, double-blind, placebo-controlled study conducted in 250 clinical centers worldwide, in which 1513 patients were randomized to losartan 50 mg once daily (n=751) or placebo (n=762). Adjunctive antihypertensive therapies (excluding ACE inhibitors and AIIRAs) could be added to both groups to help achieve the target blood pressure of < 140/90 mm Hg. The mean duration of follow-up was 3.4 years. The positive results from both IDNT 1 and RENAAL 2 help define the role of angiotensin II receptor antagonists in the management of patients with type 2 diabetes and late-stage renal disease. The primary endpoint of both trials are positive, demonstrating that irbesartan and losartan successfully reduced the risk of progression of late-stage type 2 diabetic renal disease. The irbesartan group in IDNT demonstrates a 20% RRR vs. the placebo/control group for the primary endpoint of doubling of serum creatinine, development of end-stage renal disease, or death from any cause (p=0.02), and a 23% RRR vs. the amlodipine group (p=0.006). The losartan group in RENAAL demonstrates a 16% RRR vs. the placebo/control group for an identical primary endpoint (p=0.02). There was no significant difference among the three treatment groups in IDNT for the secondary cardiovascular endpoint. Similarly, there was no significant difference between the losartan and placebo/control groups in RENAAL for a similar cardiovascular secondary endpoint. These secondary findings suggest that both agents provide similar cardiovascular protection as seen with other commonly used antihypertensive agents. (Note that all groups, including the placebo/control group, received other antihypertensive therapy in order to reach the target blood pressure) 1 Lewis et al, 2001. 2 Brenner et al, 2001.
- Opie LH, Gersh BJ. Drugs for the Heart, 5 th ed. Philadelphia, PA: W.B. Saunders Company; 2001.
- Angiotensin II receptor blockers (ARBs) such as irbesartan block the binding of angiotensin II to the AT 1 receptor, while leaving the AT 2 receptor unblocked. Opie LH, Gersh BJ. Drugs for the Heart, 5 th ed. Philadelphia, PA: W.B. Saunders Company; 2001.
- Patients were randomized to an irbesartan 150 mg group, an irbesartan 300 mg group, or a control group (placebo in addition to other nonexcluded antihypertensive therapies), and were followed for two years. This multicenter, multinational, randomized, double-blind, placebo-controlled trial assesses the renoprotective effect of 2 doses of irbesartan (150 mg and 300 mg once daily). 1 The study enrolled 590 hypertensive patients, age 30 to 70 years, with type 2 diabetes, persistent microalbuminuria (albumin excretion rate of 20-200 g/min), and normal renal function, and followed them for 2 years. Following an enrollment visit, all antihypertensive treatment was withdrawn and replaced by placebo during the single-blind, 3-week run-in screening period. Eligible patients were then randomized to receive irbesartan 150 mg, irbesartan 300 mg, or matching placebo (a control group). Additional antihypertensive agents (excluding ACE inhibitors, angiotensin II receptor antagonists, and dihydropyridine calcium channel blockers) could be added to all three groups to help achieve a target blood pressure of < 135/85 mm Hg. 1 Parving et al, 2001a.
- Mechanism of Action of Angiotensin II Receptor Antagonists The renin-angiotensin system (RAS) consists of a cascade of enzymatic reactions. Angiotensinogen is produced in the liver and is converted to angiotensin I (Ang I) by renin, secreted by juxtaglomerular cells in the kidneys [Ellis et al, 1996]. Angiotensin-converting enzyme (ACE) then converts Ang I to angiotensin II (Ang II), a potent vasoconstrictor [Oliverio et al, 1997]. Angiotensin II can bind to different receptors, most notably the AT 1 and AT 2 receptors. The AT 1 receptor is responsible for virtually all the known actions of Ang II that contribute to hypertension. The AT 2 receptor may exert opposing effects by inhibiting cell proliferation and reversing AT 1 -induced hypertrophy. Inhibition of the RAS is a powerful therapeutic tool, as evidenced by the effectiveness of ACE inhibitors in treating hypertension, congestive heart failure (CHF), MI, and diabetic nephropathy. ACE inhibition may not optimally block the RAS since several alternate enzymes capable of generating Ang II from angiotensinogen and/or Ang I in vitro have been described [Klickstein et al, 1982; Urata et al, 1990]. Further, ACE inhibitors result in the accumulation of bradykinin or other tachykinins, which may contribute to cough and angioedema [Johnston et al, 1997]. Angiotensin II receptor antagonists (AIIRAs) inhibit the AT 1 receptor, providing complete and sustained blockade of the RAS independent of the pathway of Ang II production. Further, AIIRAs do not cause accumulation of bradykinin while selectively inhibiting the AT 1 receptor and allowing for Ang II to bind to the AT 2 receptor, thus potentially enhancing the beneficial opposing effects of these receptors on endothelial proliferation, vasoconstriction and tissue repair [Lucius et al, 1998].
- IRMA 2 evaluates the effect of irbesartan compared with a control group on the progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria, an early stage of diabetic renal disease. The primary endpoint in IRMA 2 is time to occurrence of clinical proteinuria, defined as an overnight urinary albumin excretion rate (AER) exceeding 200 g/min (300 mg/day) and an increase of urinary AER from baseline by at least 30% at 2 successive 3-month evaluations. 1 Secondary endpoints include changes in overnight urinary AER, regression to normoalbuminuria (< 20 g/min), and change in creatinine clearance. 1 Parving et al, 2001a.
- Patients were randomized to an irbesartan group, an amlodipine group, or a control group (placebo in addition to other nonexcluded antihypertensive therapies), and were followed for a minimum of 2 years. This worldwide, double-blind, placebo-controlled study enrolled 1,715 hypertensive patients, age 30 to 70 years, with type 2 diabetes and late stages of renal disease (proteinuria 900 mg/day and serum creatinine between 1.0 and 3.0 mg/dL in women and 1.2 and 3.0 mg/dL in men). 1 Following initial screening for blood pressure (BP) and renal function, antihypertensive treatment with ACE inhibitors, angiotensin II receptor antagonists (AIIRAs), and/or calcium channel blockers (CCBs) were discontinued; use of other antihypertensive medication was permitted to maintain BP control. Patients were randomized to irbesartan 75 mg, amlodipine 2.5 mg, or matching placebo (a control group). Irbesartan was titrated to 300 mg once daily and amlodipine to 10 mg once daily, as tolerated. Additional antihypertensive agents (excluding ACE inhibitors, angiotensin II receptor antagonists, and calcium channel blockers) could be added to all three groups to help achieve a target blood pressure of 135/85 mm Hg or a reduction of 10 mm Hg in systolic BP in patients with systolic BP > 145 mm Hg at screening. Patients were followed for a minimum of approximately 2 years, with follow-up visits scheduled every 3 months. 1 Lewis et al, 2001.
- IDNT evaluates the effect of irbesartan compared with amlodipine and a control group on the progression of renal disease, total mortality, and cardiovascular morbidity in hypertensive patients with type 2 diabetes and later stages of diabetic renal disease. The primary outcome in IDNT is the time from randomization until the first occurrence of doubling of baseline serum creatinine, end-stage renal disease (i.e., renal transplantation, renal dialysis, or serum creatinine level 6.0 mg/dL), or death from any cause. 1 The safety and tolerability of irbesartan when administered long-term to patients with hypertension and diabetic nephropathy is also compared with that of placebo. The secondary endpoint is the time from randomization until the first occurrence of cardiovascular death, nonfatal myocardial infarction, hospitalization for heart failure, permanent neurologic deficit attributed to stroke, or above-the-ankle amputation. The primary comparison for both the primary and secondary endpoints is irbesartan versus the control group (placebo in addition to other nonexcluded antihypertensive therapies), while the secondary comparison is irbesartan versus amlodipine. 1 Lewis et al, 2001.
- Opie LH, Gersh BJ. Drugs for the Heart, 5 th ed. Philadelphia, PA: W.B. Saunders Company; 2001.
- In the IRMA 2 trial, patients were randomized to receive irbesartan 150 mg/d, irbesartan 300 mg/d, or placebo, and were followed for 2 years. This multicenter, multinational, randomized, double-blind, placebo-controlled trial assessed the renoprotective effect of 2 doses of irbesartan (150 mg and 300 mg once daily). The study enrolled 590 hypertensive patients, aged 30 to 70 years, with type 2 diabetes; persistent microalbuminuria (urinary albumin excretion rate of 20 to 200 ìg/min); normal renal function; seated systolic blood pressure >135 mm Hg and/or seated diastolic blood pressure >85 mm Hg; body mass index 40 kg/m 2 ; serum creatinine 1.5 mg/dL (males) and 1.1 mg/dL (females); and serum potassium between 3.5 mmol/L and 5.5 mmol/L. Patients were followed for 2 years. Major exclusion criteria included required treatment with angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs); type 1 diabetes; age of onset of type 2 diabetes <20 years; renal disease; need for chronic ( 1 month) treatment with nonsteroidal anti-inflammatory drugs or aspirin >325 mg/d; macroscopic hematuria; active or uncontrolled cardiac, hepatic, nondiabetic, metabolic, neurologic, pulmonary, or hematologic disorder; malignant disease; or nondiabetic renal disease. Following an enrollment visit, all antihypertensive treatment was withdrawn and replaced with placebo during the single-blind, 3-week, run-in screening period. Eligible patients were then randomized to receive irbesartan 150 mg/d, irbesartan 300 mg/d, or matching placebo. Additional antihypertensive agents (excluding ACE inhibitors, ARBs, and dihydropyridine calcium channel blockers) were allowed to be added to all 3 groups to help achieve a target blood pressure of <135/85 mm Hg. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- IRMA 2 evaluated the effect of irbesartan vs placebo on progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria, an early stage of diabetic renal disease. The primary end point in IRMA 2 was time to occurrence of clinical proteinuria, defined as an overnight urinary albumin excretion rate (UAER) >200 ìg/min (300 mg/d) and an increase in UAER from baseline of at least 30% at 2 successive 3-month evaluations. Secondary end points included change in overnight UAER, regression to normoalbuminuria (<20 ìg/min), and change in creatinine clearance. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- Shown are the baseline characteristics of patients in the IRMA 2 trial. Demographic, clinical, and biochemical characteristics were balanced among the 3 groups at baseline. Approximately two thirds of the patients were male. Mean age was approximately 58 years, mean blood pressure was approximately 153/90 mm Hg, and mean glycosylated hemoglobin was >7%. Patients were at an early stage of diabetic renal disease, with a mean serum creatinine level of approximately 1mg/dL and low levels of microalbuminuria (urinary albumin excretion rate of approximately 55 µg/min). Duration of diabetes was about 10 years. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- The IRMA 2 trial was a positive study, demonstrating a 70% risk reduction in the primary end point (time to the onset of diabetic nephropathy), independently of the effects of irbesartan on systemic blood pressure (BP). A clear dose response was observed in IRMA 2 for the primary end point. Patients who received irbesartan 150 mg/d demonstrated a 39% relative risk reduction (RRR) in the development of overt proteinuria (urinary albumin excretion rate [UAER] >200 ìg/min, and an increase of UAER from baseline of at least 30%) compared with patients who received placebo ( P =.08). Patients who received irbesartan 300 mg/d demonstrated a highly significant 70% RRR compared with patients in the control group ( P <.001). As seen in the above graph, the Kaplan-Meier curves separate at the first visit (at 3 months) and continue to diverge. After adjustment for the baseline level of microalbuminuria and the BP achieved during the study, the benefits of irbesartan in slowing progression to overt proteinuria were still present, as evidenced by an RRR of 44% for irbesartan 150 mg/d vs placebo ( P =.05) and an RRR of 68% for irbesartan 300 mg/d vs control ( P <.001). Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- In the IRMA 2 trial restoration of normoalbuminuria (<20 g/min) at the last visit was more frequent in patients treated with irbesartan 300 mg/d than in patients in the control group (34% vs 21%, respectively; P =.006). Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- Irbesartan was safe and well tolerated in hypertensive patients with type 2 diabetes and microalbuminuria. Serious adverse events were recorded in 22.8% of the patients in the control group and 15.4% of those in the combined irbesartan groups ( P =.02). There was a trend toward fewer nonfatal cardiovascular events and fewer discontinuations due to an adverse event in the irbesartan groups compared with the control group. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- IRMA 2 was a positive study, demonstrating that irbesartan 300 mg compared with placebo provides a 70% reduction in the risk of progression from microalbuminuria to overt diabetic nephropathy (defined as an overnight urinary albumin excretion rate [UAER] >200 ìg/min and an increase in UAER from baseline of at least 30%) ( P <.001). These results were independent of the effects of irbesartan on systemic blood pressure. In addition, restoration of normoalbuminuria (UAER <20 ìg/min) at the last visit was significantly more frequent in the irbesartan 300 mg/d group than in the placebo group (34% vs 21%, respectively; P =.006). Irbesartan was safe and well tolerated, and was associated with fewer serious adverse events, fewer discontinuations due to adverse events, and fewer nonfatal cardiovascular events. Parving H-H, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P, for the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study Group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345:870-878.
- In the Irbesartan Diabetic Nephropathy Trial (IDNT), patients were randomized to receive irbesartan, amlodipine, or control (placebo plus other nonexcluded antihypertensive therapies) and were followed for a minimum of 2 years. The objective of IDNT was to determine whether the inhibition of angiotensin II (Ang II) activity would alter the progression of type 2 diabetic nephropathy. This multicenter, multinational, randomized, double-blind, placebo-controlled prospective trial enrolled 1,715 hypertensive patients with type 2 diabetes and late stages of renal disease (proteinuria 900 mg/d and serum creatinine between 1.0 mg/dL and 3.0 mg/dL in women and between 1.2 mg/dL and 3.0 mg/dL in men), aged 30 to 70 years, with seated blood pressure (BP) >135/85 mm Hg and no known recent cardiovascular events. After initial screening for BP and renal function, antihypertensive treatment with angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), and/or calcium channel blockers (CCBs) was discontinued; use of other antihypertensive medication was permitted to maintain BP control. Patients were randomized to receive irbesartan 75 mg/d, amlodipine 2.5 mg/d, or matching placebo. Irbesartan was titrated to 300 mg/d and amlodipine to 10 mg/d as tolerated. Additional antihypertensive agents (excluding ACE inhibitors, ARBs, and CCBs) could be added to all 3 groups to help achieve a target BP of 135/85 mm Hg or a reduction of >10 mm Hg in systolic blood pressure (SBP) in patients with SBP >145 mm Hg at screening. Patients were followed for a minimum of approximately 2 years, with follow-up visits scheduled every 3 months. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- IDNT evaluated the effects of irbesartan, amlodipine, and control (placebo plus other nonexcluded antihypertensive therapies) on the progression of renal disease, total mortality, and cardiovascular (CV) morbidity in hypertensive patients with type 2 diabetes and late stages of diabetic renal disease. The primary outcome in IDNT was the time from randomization until the first occurrence of doubling of baseline serum creatinine (SeCr), end-stage renal disease (ie, renal transplantation, renal dialysis, or SeCr level 6.0 mg/dL), or death from any cause. The safety and tolerability of irbesartan when administered long-term to patients with hypertension and diabetic nephropathy was also compared with that of placebo. The secondary end point was the time from randomization until the first occurrence of CV death, nonfatal myocardial infarction, hospitalization for heart failure, permanent neurologic deficit attributed to stroke, or above-the-ankle amputation. The primary comparison for both the primary and secondary end points was irbesartan versus control, while the secondary comparison was irbesartan versus amlodipine. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- The baseline demographics of the 1,715 patients enrolled in IDNT 1 are shown above. The demographics of the 3 groups were similar, except for a slightly lower percentage of females assigned to the control group. Mean age was approximately 59 years. Most patients were male and had type 2 diabetes for a mean of about 15 years. 1 Compared with patients enrolled in the Collaborative Study Group trial, 2 which evaluated the benefits of captopril in type 1 diabetic nephropathy, the type 2 diabetic patients enrolled in IDNT were older, more obese, and generally at higher risk, with higher levels of blood pressure and serum creatinine and a higher incidence of previous cardiovascular events. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD, for the Collaborative Study Group. The effect of angiotensin-converting–enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993;329:1456-1462.
- The baseline clinical and laboratory characteristics of patients in IDNT are shown above. The clinical and laboratory characteristics of the 3 groups in IDNT were similar. Median urinary protein excretion rate and mean serum creatinine level were 2.9 g/24 h and approximately 1.7 mg/dL, respectively. Mean glycosylated hemoglobin was slightly more than 8%. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- IDNT was a positive study, with irbesartan demonstrating a 20% relative risk reduction (RRR) in reaching the primary end point vs control (placebo plus other nonexcluded antihypertensive therapies), and a 23% RRR vs amlodipine, independent of its effects on systemic blood pressure (BP). In IDNT, treatment with irbesartan provided a 20% RRR in the primary end point of doubling of serum creatinine, development of end-stage renal disease, or death from any cause compared with treatment with control ( P =.02), and a 23% RRR compared with treatment with amlodipine ( P =.006). No significant difference was observed between the control and amlodipine groups. The better outcomes among patients in the irbesartan group could not be explained by differences in achieved BP. Although the mean arterial pressure (MAP) of patients in the irbesartan group was the same as that of patients in the amlodipine group, there was a significant difference in the primary end point in favor of irbesartan. Furthermore, correction for achieved MAP at quarterly visits during follow-up in a time-dependent proportional–hazards analysis gave results similar to those of the primary analysis. After adjustment for BP, the benefits of irbesartan were still present: RRR of 19% for irbesartan versus control ( P =.03) and RRR of 24% for irbesartan versus amlodipine ( P =.005). Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- Results of IDNT showed that irbesartan provided a greater than 30% relative risk reduction (RRR) in the doubling of baseline serum creatinine (SeCr) versus either control (placebo plus other nonexcluded antihypertensive therapies) or amlodipine. Patients assigned to the irbesartan group had a 33% RRR in the doubling of baseline SeCr compared with patients in the control group ( P =.003) and a 37% RRR compared with patients in the amlodipine group ( P <.001). Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- In IDNT, irbesartan provided cardiovascular (CV) protection similar to that provided by other commonly used antihypertensive agents. There was no significant difference among the irbesartan, amlodipine, and control (placebo plus other nonexcluded antihypertensive therapies) groups in the risk of all-cause mortality or in the risk of CV events. Thus, irbesartan provided CV protection similar to that seen with other commonly used antihypertensive agents, including amlodipine, diuretics, and beta blockers. It should be noted that the size and duration of IDNT may have been insufficient to detect any differences in CV outcomes. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
- Irbesartan therapy was generally safe and well tolerated in IDNT. In this trial, only one episode of an acute early rise in serum creatinine occurred, which suggests a possible bilateral renal-artery stenosis. However, this subject was assigned to the control group and did not receive any renin-angiotensin-system blocking agent. 2 Hyperkalemia requiring discontinuation of study medicine was an uncommon event, occurring in 1.9% of patients in the irbesartan group. 1 Overall, approximately 24% of patients in the trial discontinued the study drug before reaching a primary end point or before their data were censored. The most common reason for discontinuing study medication was the occurrence of a clinical cardiovascular event. These discontinuations were evenly balanced among the 3 groups. 1 There was no significant difference among groups in the percentage of patients experiencing at least one serious adverse event (SAE). However, patients in the irbesartan group had a significantly lower rate of SAEs (2.0/1000 days on drug) than those in the control group (2.3/1000 days on drug) or the amlodipine group (2.5/1000 days on drug); P =.002 for placebo and amlodipine. 2 Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860. Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo Inc.
- IDNT was a positive study, with irbesartan demonstrating a 20% RRR in the primary composite end point of doubling of serum creatinine, development of end-stage renal disease, or death compared with control ( P =.02) and a 23% RRR compared with amlodipine ( P =.006). These results were independent of the effects of irbesartan on systemic BP; in fact, the BP lowering observed was similar in the irbesartan and amlodipine groups (average BP achieved with irbesartan was 140/77 mm Hg; with amlodipine, 141/77 mm Hg). There were no significant differences among the 3 groups in the risk of cardiovascular (CV) events; the size and duration of IDNT was insufficient to detect any differences. Irbesartan provided CV protection similar to that seen with other commonly used antihypertensive agents, including amlodipine, diuretics, and beta blockers. Irbesartan was also generally safe and well tolerated, with a lower rate of serious adverse events in patients receiving irbesartan than in those receiving control or amlodipine. Lewis EJ, Hunsicker LG, Clarke WR, et al, for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.