1. Chapter 57
Intensive Care Monitoring of the Critically
Ill Pregnant Patient
Stephanie Rae Martin, DO, and Michael Raymond Foley, MD
Less than 1% of pregnant women will become critically ill and require Mortality rates have declined precipitously in the United States
admission to an intensive care unit (ICU).1-8 Between 47% and 93% over the past century, but a slight increase has been observed in more
of ICU admissions result from an obstetric complication, primarily recent years, as shown in Figure 57-2.11 Some of this increase has been
hemorrhage and hypertensive disorders. Other common causes include attributed to better ascertainment of data collected prospectively and
respiratory failure and sepsis. Common non-obstetric indications for to the use of multiple source documents. Although this trend is exhib-
ICU admission include maternal cardiac disease, trauma, anesthetic ited for all races, wide discrepancies still exist between white and non-
complications, cerebrovascular accidents, and drug overdosage. In white populations, even when controlling for age and use of prenatal
many series, most obstetric ICU admissions occur in the immediate care (Fig. 57-3).12 The reasons for this discrepancy remain unclear.
postpartum period and are most likely caused by complications of Geographic differences in maternal mortality rates are also apparent
acute hemorrhage.1,4-6,9 and are likely influenced by racial disparities. States with higher per-
An intimate understanding of the physiologic changes of pregnancy centages of births to African-American women are also those with the
is essential in managing critically ill patients. This chapter addresses highest maternal mortality rates. The data on pregnancy-related mor-
basic critical care monitoring in obstetrics and discusses conditions in tality in the United States between 1990 and 1997 indicate a rate
which more intensive management of the pregnant patient may be of 11.8 deaths per 100,000 pregnant women (8.1 deaths per 100,000
indicated. whites, 30.0 deaths per 100,000 African Americans).12 Advancing
maternal age and lack of education are also associated with an increased
risk for death in pregancy.12 Potential explanations for this increased
risk include a higher incidence of underlying or undiagnosed chronic
Maternal Mortality disease.
Epidemiology
Maternal mortality is defined as the number of maternal deaths (direct Prediction of Maternal Mortality
and indirect) per 100,000 live births. Direct obstetric deaths result pri- Predicting the risk of mortality for pregnant patients remains a chal-
marily from thromboembolic events, hemorrhage, hypertensive dis- lenge. The overall maternal mortality rate for critically ill gravidas
orders of pregnancy, and infectious complications. Indirect obstetric admitted to an ICU ranges from 0% to 20%, with most series reporting
deaths arise from preexisting medical conditions, including diabetes, maternal mortality rates of less than 5% for all obstetric ICU admis-
systemic lupus erythematosus, pulmonary disease, and cardiac disease sions.1,3-5,8 Several scoring systems are routinely employed in critical
aggravated by the physiologic changes of pregnancy. Figure 57-1 shows care settings in an attempt to objectively describe the severity of the
specific causes of pregnancy-related mortality for three time periods as critical illness and accurately predict mortality risks. The Acute Physi-
reported by the Centers for Disease Control and Prevention.10-12 ologic and Chronic Health Evaluation (APACHE) scoring system,14,15
Maternal mortality rates are periodically surveyed by various local, Simplified Acute Physiologic Score (SAPS),16 and Mortality Prediction
state, and national agencies. Because these data are primarily collected Model (MPM)17 are three widely used methods that track a variety of
from death certificates, some have suggested that the numbers under- variables in nonpregnant patients.
estimate the mortality rate by as much as 20% to 50%.13 Variations in Several authors have evaluated the applicability of the scoring
the definition of maternal death, medicolegal concerns, and physicians systems in critically ill pregnant patients.18-20 In a study of obstetric
untrained in the proper completion of death certificates further ICU patients, the APACHE III score did not accurately predict mater-
confuse these investigations. To address these concerns, the Division nal mortality.18 In the largest series, 93 gravidas were compared with
of Reproductive Health at the Centers for Disease Control and Preven- 96 nonpregnant women. The overall mortality rate in the obstetric
tion, in collaboration with the American College of Obstetricians and population was 10.8%. The APACHE II, SAPS II, and MPM II scoring
Gynecologists (ACOG) and state health departments, began in 1987 systems each performed well in predicting mortality (14.7%, 7.8%,
to systematically collect these data in the Pregnancy-Related Mortality and 9.1%, respectively).19 The predicted mortality rate was signifi-
Surveillance System. cantly higher among obstetric patients compared with non-obstetric
2. 1168 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
180
160
140
White
120 Black
100
Ratio
80
60
40
20
0
19 20–24 25–29 30–34 35–39 40
Age group (yrs)
FIGURE 57-3 Pregnancy-related mortality ratios by age and race in
the United States for 1991 to 1999. The mortality ratios are the
FIGURE 57-1 Causes of maternal mortality for three time number of deaths per 100,00 live births.
periods. Obstetric deaths are caused by thromboembolic events,
hemorrhage, hypertension, infections, and preexisting medical
conditions, such as diabetes, systemic lupus erythematosus,
pulmonary disease, and cardiac disease aggravated by the physiologic to the obstetric population, they have the potential to overestimate the
changes of pregnancy. CVA, cerebrovascular accident; HTN, mortality risk for critically ill gravidas.
hypertension. (From Berg CJ, Chang J, Callaghan WM, et al:
Pregnancy-related mortality in the United States, 1991-1997. Obstet
Gynecol 101:289-296, 2003.)
Invasive Central
Hemodynamic Monitoring
30
Background and Insertion Technique
25
Placement of a central venous catheter may be indicated to provide
20 central venous access for fluid replacement, medication administra-
tion, or hemodynamic measurements. Since its introduction in the
Ratio
15 early 1970s,21 invasive hemodynamic monitoring with a pulmonary
10
artery catheter (PAC) has become quite common in critically ill
patients. The most commonly available Swan-Ganz catheters are
5 multilumen devices that enable direct monitoring of central venous
pressure (CVP, right ventricular preload), pulmonary capillary wedge
0 pressure (PCWP, left ventricular preload), cardiac output (CO), sys-
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
temic vascular resistance (SVR, left ventricular afterload), pulmonary
19
19
19
19
19
19
19
19
19
19
19
19
19
19
19
Year artery pressures, and mixed venous oxygen saturation. CO and mixed
venous oxygen saturation can be measured in the conventional manner
FIGURE 57-2 Maternal mortality ratios in the United States by by thermodilution and direct distal port aspiration, respectively, or by
year for 1967 to 1996. Ratios are the number of maternal deaths newer fiberoptic technology that allows continuous monitoring of CO
per 100,000 live births. The term ratio is used instead of rate because and mixed venous oxygen saturation.
the numerator includes some maternal deaths that were not related PACs (i.e., Swan-Ganz catheters) are typically inserted percutane-
to live births and therefore were not included in the denominator. ously through an introducer sheath and in a sterile manner through
(From Centers for Disease Control and Prevention: Maternal the left subclavian or right internal jugular veins and advanced into
Mortality—United States, 1982-1996. MMWR Morb Mortal Wkly Rep the right heart. The right internal jugular vein is usually preferred
47:705-707, 1998.)
because it offers the shortest and most direct entry into the right
heart. Access through the femoral vein offers the advantage of com-
pressibility in a patient with a coagulopathy, but it is most distant
patients for each of the three scoring tools, despite no difference in from the right heart and may require fluoroscopic guidance. As the
actual mortality between the two groups (10.8 versus 10.4%). catheter is advanced, characteristic oscilloscopic pressure waveforms
None of the scoring systems includes adjustments for normal are used to establish the catheter’s location within the heart. A 1.5-mL
obstetric physiologic changes such as decreased blood pressure and balloon is positioned close to the tip of the catheter. Inflation of the
increased respiratory rate. Laboratory abnormalities such as elevated balloon allows the catheter to be carried through the heart by flowing
liver function test results and low platelet counts, which are common blood.
in obstetric disorders such as HELLP syndrome (hemolysis, elevated After the inflated balloon reaches the pulmonary artery, it travels
liver enzymes, and low platelets), are not included in the assessments distally until it wedges in a smaller-caliber artery and occludes blood
and may limit their potential applicability. In summary, although the flow. This results in a nonpulsatile waveform from which the PCWP
available critical care mortality scoring systems can possibly be applied is measured. When the balloon is deflated, return of an identifiable
3. CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient 1169
pulmonary artery systolic and diastolic pressure tracing should occur. TABLE 57-1 POTENTIAL PULMONARY ARTERY
A portable chest radiograph is indicated after placement of a PAC to CATHETER COMPLICATIONS
verify appropriate catheter positioning and exclude pneumothorax.
At Insertion After Placement
Indications for Pulmonary Pneumothorax Pulmonary infarction
Artery Catheterization Thrombosis Pulmonary artery rupture
Arterial puncture Infection
The most common indications for PAC placement in the obstetric Air embolization Balloon rupture
population include the following22: Catheter knotting Endocardial or valvular damage
Cardiac arrhythmias (transient,
Hypovolemic shock unresponsive to initial volume sustained)
resuscitation attempts
Septic shock with refractory hypotension or oliguria
Severe preeclampsia with refractory oliguria or pulmonary
edema complication rates decline as operator experience increases, and only
Ineffective intravenous antihypertensive therapy properly trained personnel should insert catheters for invasive hemo-
Adult respiratory distress syndrome (ARDS) dynamic monitoring.38 Several studies have also demonstrated that
Intraoperative or intrapartum cardiac failure ultrasound-guided placement results in fewer failed attempts at place-
Severe mitral or aortic valvular stenosis ment, fewer complications such as hematoma or arterial puncture, and
New York Heart Association (NYHA) class III or IV heart less time for placement.39
disease in labor Complications encountered at initial insertion include arterial
Anaphylactoid syndrome of pregnancy (i.e., amniotic fluid puncture, pneumothorax, and air embolism. Pneumothorax risks are
embolism) highest with a subclavian approach. Transient cardiac arrhythmias are
commonly encountered during placement and advancement of the
Although use of the PAC in nonpregnant critically ill patients is PAC. The majority consist of premature ventricular contractions or
widespread, until recently, randomized trials demonstrating a clear nonsustained ventricular tachycardia, and they resolve with withdrawal
benefit of PAC-directed care were lacking. Several small studies or advancement of the catheter. The overall incidence of transient
suggested a decrease in mortality when PACs are used to direct thera- minor arrhythmias during advancement of a PAC exceeds 20% in most
pies,23-25 while others reported an increase in mortality associated with studies.37 Significant arrhythmias such as sustained ventricular tachy-
the use of PACs26-29 or no benefit.30-32 The large Canadian Critical Care cardia or fibrillation are less common, occurring in less than 4% of
Clinical Trials Group study prospectively randomized 1994 high-risk patients in most series, and they are more likely to be encountered in
surgical patients to receive a PAC to direct therapy or standard therapy patients with cardiac ischemia.37
and reported no survival benefit when therapy was directed by Infections related to central venous catheters are common and
a PAC (7.8% versus 7.7% for controls).33 A British trial randomized may involve a superficial skin infection, colonization, or a more
more than 1000 critically ill patients to management with or without serious bacteremia. Skin flora, particularly Staphylococcus species, are
a PAC and failed to demonstrate a survival benefit (68.4% versus most commonly involved. Positive cultures from the tip of a PAC are
65.7% for controls).34 The Evaluation Study of Congestive Heart common and are considered evidence of colonization. However, for
Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE bacteremia or sepsis to be diagnosed, the patient must also have posi-
trial) also demonstrated no difference in mortality or length of stay for tive blood cultures with the same organism and clinical evidence of
433 patients with congestive heart failure randomized to PAC or no systemic infection, such as fever or hypotension.40 The risk of bactere-
catheter.35 mia is approximately 0.5% per catheter day, and the risk increases with
A meta-analysis of 13 trials published since 1985 included 5051 each day the catheter remains indwelling. Bacteremia resulting from
patients randomized to a PAC or to no PAC to guide management. central venous catheters accounts for 87% of bloodstream infections
No difference was identified in mortality or length of hospital stay. in critically ill patients.41 Infectious complications can be minimized
Conversely, the use of a PAC was significantly associated with more by adherence to strict sterile technique, placement in the subclavian
frequent use of inotropes and vasodilators.36 In summary, although site, use of antimicrobial-coated catheters, avoiding antibiotic oint-
placement of PACs remain widespread, the available data do not ments that can increase fungal colonization, avoiding empiric catheter
support the routine use of PACs for all critically ill patients. Data changes, and removing the catheter as soon as possible.42
addressing the role of PACs in pregnant critically ill patients are Venous thrombosis risk can be minimized by placement at the sub-
lacking. clavian site and by limiting the duration of catheter placement. Pulmo-
nary infarction may occur as a result of direct occlusion of a pulmonary
artery branch caused by drifting of the catheter or thromboembolic
Complications of Central events. Catheter knotting can be avoided during placement if the opera-
Venous Catheters tor remains aware of the centimeter markings on the advancing cathe-
ter. The right ventricle usually is reached when the catheter has been
Common complications associated with initial venous access, advance- inserted 25 to 30 cm from the jugular vein site. Few patients require
ment, and maintenance of a PAC are listed in Table 57-1.37 Some more than 50 cm of catheter to reach the pulmonary artery. Inflated
complications, such as pulmonary infarction and pulmonary artery catheter balloons should be checked before insertion to reduce the risk
rupture, are specific to placement of a PAC and do not occur with of air leakage and balloon rupture. Overinflation of the balloon with
central venous access alone. Minimal available data address specific air (>1.5 mL) should be avoided. A pressure-release balloon has been
complication rates associated with PAC use in pregnant women. Initial described that limits overinflation and thereby minimizes pulmonary
4. 1170 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
24 TABLE 57-2 FORMULAS FOR CALCULATING
HEMODYNAMIC VARIABLES
22
SVR = [(MAP − RAP)]/CO × 80
20 PVR = (PAP − PCWP/CO) × 80
18 CO = VO2/(CaO2 − CvO2)
DO2 = CO × CaO2 × 10
PCWP (mm Hg)
16 VO2 = (CaO2 − CvO2) × CO × 10
CaO2 = (1.34 × Hb × SaO2) + (0.003 × PaO2)
14
CvO2 + (1.34 × Hb × SvO2) + (0.003 × PvO2)
12 O2 extraction = VO2/ DO2
Qs/Qt = CcO2 − CaO2/CcO2 − CvO2
10
CaO2, arterial oxygen concentration; CcO2, end capillary O2 content;
8
CO, cardiac output; CvO2, venous oxygen concentration; DO2, oxygen
6 delivery; Hb, hemoglobin; MAP, mean arterial pressure; O2, oxygen;
PaO2, arterial partial pressure of oxygen; PAP, pulmonary artery
4 pressure; PCWP, pulmonary capillary wedge pressure; PvO2, venous
partial pressure of oxygen; PVR, pulmonary vascular resistance;
2 Qs/Qt, shunt fraction; RAP, right atrial pressure; SaO2, arterial oxygen
saturation; SvO2, venous oxygen saturation; SVR, systemic vascular
–2 0 2 4 6 8 10 12 14 16 18 resistance; VO2, oxygen consumption.
CVP (mm Hg)
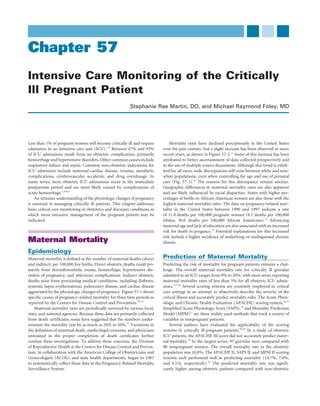
FIGURE 57-4 Relationship of central venous pressure (CVP)
to pulmonary capillary wedge pressure (PCWP) in severe obtained. Table 57-2 lists formulas for calculating selected hemody-
pregnancy-induced hypertension. If an accurate assessment of left namic variables.
ventricular preload is deemed important in the management of the Hemodynamic variables often are expressed in an “indexed” fashion
patient’s cardiovascular complications, insertion of a pulmonary artery
(i.e., cardiac index). To do this, the original nonindexed CO value must
catheter may be indicated. (From Cotton DB, Gonik B, Dorman K,
et al: Cardiovascular alterations in severe pregnancy-induced
be divided by body surface area. Because standard body surface area
hypertension: Relationship of central venous pressure to pulmonary calculations have never been established specifically for pregnancy, this
capillary wedge pressure. Am J Obstet Gynecol 151:762, 1985.) traditional way of expressing hemodynamic data is somewhat contro-
versial in obstetrics. Those who argue for its use point out that index-
ing allows direct comparison of hemodynamic parameters for pregnant
vessel injury. Pulmonary artery rupture is a rare but often fatal compli- women of different sizes, a critical issue when interpreting these
cation that occurs more commonly in patients with pulmonary artery values.
hypertension or who are anticoagulated. Valvular damage can occur Mean hemodynamic measurements for pregnant and nonpregnant
from chronic catheter irritation or during insertion when the catheter patients are presented in Table 57-3. They are paired data from 10
balloon is not deflated before retrograde movement. healthy subjects, taken between 36 and 38 weeks’ gestation and between
CVP monitoring alone should not be considered equivalent to PAC 11 and 13 weeks after delivery.45 Using the noninvasive technique of
monitoring. Preeclampsia and its complications, such as oliguria M-mode echocardiography, other investigators have demonstrated
and pulmonary edema, may prompt central venous access. However, that many of these physiologic alterations in hemodynamics begin in
several investigators have described poor correlation between the the early phases of pregnancy.46 Position changes late in pregnancy
central venous catheter and PCWP in gravidas with pregnancy-induced significantly influenced central hemodynamic stability. The standing
hypertension (Fig. 57-4).43,44 If an accurate assessment of left ventricu- position increased pulse by 50%, left ventricular stroke work index by
lar preload is deemed important in the management of the patient’s 21%, and pulmonary vascular resistance by 54%.47 Compared with the
cardiovascular complications, insertion of a PAC may be indicated. nonpregnant state, the pregnant state seemed to result in a buffering
Whether this holds true for pregnant women with critically ill disease of orthostatic-related hemodynamic changes. The investigators specu-
states other than pregnancy-induced hypertension remains unknown. lated that the increased intravascular volume during pregnancy
accounted for this stabilizing effect.
Hemodynamic Considerations
With a PAC, the following hemodynamic variables can be directly
measured in the patient: Hemodynamics of Specific Conditions
during Pregnancy
Heart rate (beats/min)
CVP (mm Hg) Mitral Valve Stenosis
Pulmonary artery systolic and pulmonary artery diastolic Mitral stenosis is the most common rheumatic valvular lesion encoun-
pressures (mm Hg) tered in pregnancy (see Chapter 39). When the valve area falls below
PCWP (mm Hg) 1.5 cm2, filling of the left ventricle during diastole is severely limited,
CO (L/min) resulting in a fixed CO. Prevention of tachycardia and maintenance of
Mixed venous oxygen saturation (%) adequate left ventricular preload is essential in these patients. As the
heart rate increases, less time is allowed for the left atrium to ade-
By use of a sphygmomanometer or by peripheral artery catheteriza- quately empty and fill the left ventricle during diastole. The left atrium
tion, direct measurements of systemic arterial pressures can also be may become overdistended, resulting in dysrhythmias (primarily atrial
5. CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient 1171
TABLE 57-3 NORMAL CENTRAL HEMODYNAMIC PARAMETERS IN HEALTHY NONPREGNANT AND
PREGNANT PATIENTS
Hemodynamic Parameter Nonpregnant Values Pregnant Values
Cardiac output (L/min) 4.3 ± 0.9 6.2 ± 1.0
Heart rate (beats/min) 71 ± 10 83 ± 10
Systemic vascular resistance (dyne × cm × sec−5) 1530 ± 520 1210 ± 266
Pulmonary vascular resistance (dyne × cm × sec−5) 119 ± 47 78 ± 22
Colloid oncotic pressure (mm Hg) 20.8 ± 1.0 18.0 ± 1.5
Colloid oncotic pressure − pulmonary capillary wedge pressure (mm Hg) 14.5 ± 2.5 10.5 ± 2.7
Mean arterial pressure (mm Hg) 86.4 ± 7.5 90.3 ± 5.8
Pulmonary capillary wedge pressure (mm Hg) 6.3 ± 2.1 7.5 ± 1.8
Central venous pressure (mm Hg) 3.7 ± 2.6 3.6 ± 2.5
Left ventricular stroke work index (g × m × m−2) 41 ± 8 48 ± 6
From Clark SL, Cotton DB, Lee W, et al: Central hemodynamic assessment of normal term pregnancy. Am J Obstet Gynecol 161:1439, 1989.
fibrillation, which increases the risk of thromboembolic complica- for patients with primary pulmonary hypertension; mean survival is
tions) or pulmonary edema. Adequate preload, however, is essential to 2.8 years from the diagnosis. Maternal mortality rates for patients with
maintain left ventricular filling pressure. Alternatively, if preload pulmonary hypertension have been as high as 50%.48-50 These patients
is excessive, pulmonary edema and atrial dysrhythmias may result. are at increased risk for complications from placement of a PAC.
Medical management of these patients involves activity restriction, Pulmonary hypertension may also result from unrepaired congenital
treatment of dysrhythmias, β-blockers to control heart rate, and careful intracardiac shunts such as a ventricular septal defect, atrial septal
diuretic use. The goal of diuretic therapy is to treat pulmonary edema, defect, or patent ductus arteriosus, which lead to chronic over-
with care not to overly reduce left ventricular preload. Adequate anal- perfusion of the pulmonary vasculature. Over time, pulmonary arterial
gesia and anesthesia during labor and delivery also reduce excessive pressures may become significant enough to reverse the direction of
cardiac demands associated with pain and anxiety. flow across the shunt. This reversal of shunt flow to a right-to-left
The other important hemodynamic consideration for patients pattern defines Eisenmenger syndrome. The estimated maternal mor-
with mitral valve stenosis relates to the potential for misinterpretation tality rate for Eisenmenger syndrome is between 30% and 40%.50,51 In
of the invasive monitoring data. Because of the stenotic mitral valve, a review of 73 patients with Eisenmenger syndrome, the overall mor-
PCWP readings do not accurately reflect left ventricular diastolic tality rate was 36%, which has been essentially unchanged during the
pressure. In some instances, very high PCWP values are recorded (and past 2 decades.50
are needed to maintain an adequate CO). Overt pulmonary edema is The underlying problem in patients with this condition is obstruc-
usually not associated with these high readings. During attempts at tion to right ventricular outflow caused by a fixed and elevated
maintaining a relatively constricted intravascular volume, the CO pulmonary vascular resistance. This can ultimately lead to right-to-left
should be concomitantly monitored and maintained. For each indi- shunting of deoxygenated blood with resultant hypoxemia. Reductions
vidual patient, optimal PCWP and CO values (i.e., values that maintain in blood return to the heart can decrease right ventricular preload so
blood pressure and tissue perfusion) should be determined. that the pulmonary vasculature is further hypoperfused. The resultant
hypoxemia has been associated with sudden death. Intrapartum man-
Aortic Stenosis agement requires maintenance of a relatively hypervolemic state, and
The major problem encountered with aortic stenosis is the patient’s any interventions that may lead to significant reduction in preload or
potential inability to maintain CO because of severe obstruction or in decrease in SVR should be avoided. Placement of a PAC may be quite
the setting of decreasing left ventricular preload (see Chapter 39). challenging in these patients, and many experts believe the risks of
Unlike mitral valve stenosis, aortic valve stenosis requires that attempts placement may outweigh any potential benefit.
be made to maintain the patient in a relatively hypervolemic state,
although the fixed CO may lead to pulmonary edema. The time sur- Anaphylactoid Syndrome of Pregnancy
rounding labor and delivery is particularly risky for these patients. To Anaphylactoid syndrome of pregnancy (i.e., amniotic fluid embolus)
maintain an adequate CO, adequate venous return to the heart is is a rare but devastating complication of pregnancy characterized by
crucial. Decreased venous return can result from excess blood loss, acute onset of hypoxia, hypotension or cardiac arrest, and coagulopa-
hypotension, and ganglionic blockade from a regional anesthetic or thy occurring during labor, during delivery, or within 30 minutes after
even vena caval occlusion in the supine position. Pulmonary artery delivery.52,53 This same constellation of findings may have other causes,
catheterization may be indicated in patients with significant aortic such as hemorrhage, uterine rupture, or sepsis, and each should be
stenosis to accurately estimate intravascular volume and guide fluid excluded before assigning a diagnosis of amniotic fluid embolism. The
replacement. combination of sudden cardiovascular and respiratory collapse with a
coagulopathy is similar to that observed in patients with anaphylactic
Pulmonary Hypertension or septic shock. In each of these settings, a foreign substance (e.g.,
Pulmonary artery hypertension may arise as a primary lesion or result endotoxin) is introduced into the circulation. This initiates a cascade
from an underlying cardiac abnormality (see Chapter 39). Primary of events resulting in activation and release of mediators such as his-
pulmonary hypertension is characterized by an unexplained elevation tamines, thromboxane, and prostaglandins, which lead to dissemi-
in pulmonary artery pressures (>25 to 30 mm Hg). Prognosis is grim nated intravascular coagulation (DIC), hypotension, and hypoxia. The
6. 1172 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
inciting factor is presumed to be present in amniotic fluid that is
120
introduced into the maternal circulation, but the precise factor that
initiates the sequence have not been identified. It is a commonly held
110
misconception that the presence of fetal debris in the pulmonary cir-
culation is diagnostic of an amniotic fluid embolus. Fetal debris can 100
Left ventricular stroke work index
be found in the pulmonary circulation in most normal laboring
patients, and it is identified only in 78% of patients who meet the 90
criteria for the diagnosis of amniotic fluid embolism.52,53
Management of amniotic fluid embolism is entirely supportive. 80
(gm m m 2)
Replacement of blood and clotting factors, adequate hydration and
blood pressure support, ventilatory support, and invasive cardiac mon- 70
itoring in addition to resuscitation efforts usually are required for these
patients. The data suggest mortality rates approach 61% or higher. 60
Most patients do not survive the initial course and die within 5 days.
For those who survive, neurologic impairment is common.52 50
40
Hypertensive Disorders of Pregnancy
Most clinical hemodynamic monitoring studies in obstetrics have
30
enrolled patients with hypertensive disorders of pregnancy (see Chapter
35). From a purely clinical perspective, clear indications for this inva- 0
sive technology have not been established. Arguments for its use center 0 5 10 15 20 25 30
on reports demonstrating a broad spectrum of hemodynamic findings Pulmonary capillary wedge pressure
in this group of patients. For patients identified to be relatively hypo- (mm Hg)
volemic, optimizing intravascular volume status should improve
uteroplacental perfusion, reduce SVR, and blunt hypotensive compli- FIGURE 57-5 Ventricular function in pregnancy-induced
cations associated with conduction anesthesia and antihypertensive hypertensive patients. On plots of ventricular function curves that
therapy. Oliguria (particularly if unresponsive to fluid therapy) and correlate pulmonary capillary wedge pressure with left ventricular
refractory pulmonary edema, both recognized complications of severe stroke work index, most preeclamptic and eclamptic patients fall into
preeclampsia, may also be better defined and managed with invasive a relatively hyperdynamic range. (Combined data from Benedetti TK,
Cotton DB, Read JC, et al: Hemodynamic observations in severe
monitoring.
pre-eclampsia with a flow-directed pulmonary artery catheter. Am J
Vasospasm is a central feature of preeclampsia. In one series of 51 Obstet Gynecol 136:465, 1980; Hankins GDV, Wendel GP,
untreated preeclamptic patients, an elevated SVR value was identified Cunningham FG, et al: Longitudinal evaluation of hemodynamic
with invasive monitoring.54 Preeclampsia likely represents an overall changes in eclampsia. Am J Obstet Gynecol 15:506, 1984; Phelan
vasoconstrictive condition that is frequently influenced by underlying JP, Yurth DA: Severe preeclampsia. I. Peripartum hemodynamic
disease processes such as chronic hypertension, duration and severity observations. Am J Obstet Gynecol 144:17, 1982; and Rafferty TD,
of illness, and various therapeutic modalities. Berkowitz RL: Hemodynamics in patients with severe toxemia during
Using ventricular function curves that correlate PCWP (i.e., left labor and delivery. Am J Obstet Gynecol 138:263, 1980.)
ventricular preload) with left ventricular stroke work index (i.e., myo-
cardial contractility), investigators found that most preeclamptic and
eclamptic patients fall into a relatively hyperdynamic range.55 The nine or fractional excretion of sodium. Although these urinary param-
values shown in Figure 57-5 are superimposed on ventricular function eters are routinely used in non-obstetric patients to differentiate
graphs derived from nonpregnant subjects. The preeclamptic patient prerenal and renal causes of oliguria, they have proved to be unreliable
probably has at least a normal and probably a somewhat hyperdynamic in patients with preeclampsia. In preeclampsia complicated by oliguria,
functioning heart during pregnancy. As expected, this cardiac function, urinary diagnostic indices may suggest a prerenal cause despite normal
as estimated by CO, appears to be inversely related to SVR. intravascular volume, demonstrated by invasive pressure measurement
Some investigators have recommended that patients with preg- determinations. From a physiologic standpoint, it is postulated that the
nancy-induced hypertension be classified by different hemodynamic kidney misinterprets local renal artery vasospasm to indicate a volume-
subsets so that management protocols can be tailored to individual depleted state.
needs. Clark and associates56 first reported the use of this approach for
dealing with the oliguric preeclamptic patient. They found that these Septic Shock
patients had low PCWP values (i.e., hypovolemic) and elevated SVR Septic shock refers to the systemic inflammatory response syndrome
(i.e., severe vasoconstriction) or were volume replete with normal to associated with infection, persistent hypotension, and major organ
elevated vascular resistances. A third group had markedly elevated dysfunction despite initial fluid resuscitation.57 Although the hemody-
PCWP and SVR readings with depressed cardiac function.56 Manage- namic effects of septic shock have been well described in the non-
ment of these groups of oliguric patients varies. In the first subset, obstetric literature, limited information is available for obstetric
patients respond favorably to volume expansion therapy. The next two patients. One study described the hemodynamic profiles of 10 obstet-
groups of patients are best managed with vasodilators and aggressive ric patients at various gestational ages, who were identified to have
afterload reduction therapy. septic shock and required invasive monitoring. In this small series, SVR
Another important issue in the management of oliguric patients and myocardial function were depressed but improved with therapy.58
with preeclampsia is the use of standard urinary diagnostic indices, Mabie and coworkers59 described similar findings in a more recent
such as urine-to-plasma ratios of osmolality, urea nitrogen, and creati- series of 18 obstetric patients with septic shock. The main hemody-
7. CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient 1173
namic characteristics of those who succumbed to septic shock included
lower blood pressure, stroke volume, and left ventricular stroke work
index than survivors.59 Sepsis and septic shock are addressed in more Respiratory Failure
detail later in this chapter.
Substantial anatomic and physiologic changes occur over the course of
pregnancy that impact respiratory function (see Chapter 7). Minute
ventilation increases in a normal pregnancy and is determined by
Noninvasive Hemodynamic respiratory rate and tidal volume. The 40% increase in tidal volume
Assessment (i.e., amount of air exchanged during a cycle of inspiration and expira-
tion) primarily drives the increase in minute ventilation. As a result,
The PAC is the gold standard for measurement of hemodynamic status the levels of CO2 decline, creating an alkalotic state. To accommodate
in the critically ill patient. However, according to available data, use of for the decrease in CO2, the kidneys excrete bicarbonate (HCO3−). An
the PAC to guide therapy does not favorably affect survival and carries arterial blood gas determination in a normal pregnant woman there-
substantial risks. fore reflects a slightly increased pH, decreased PCO2, and decreased
Transesophageal echocardiography (TEE) has emerged as a nonin- serum HCO3− (i.e., respiratory alkalosis with compensatory metabolic
vasive tool for the bedside assessment of the hemodynamic status of acidosis), as outlined in Table 57-5. As the pregnancy progresses,
nonpregnant, critically ill adults. In an anesthetized patient, a small increasing abdominal girth leads to an upward displacement of the
transducer is introduced into the esophagus and real-time data diaphragm, widening of the subcostal angle by 50%, and increased
collected. TEE can accurately measure left ventricular preload, left chest circumference. The end result is a decrease in the functional
ventricular filling pressure, CO, left ventricular ejection fraction, and residual capacity by 20%. The functional residual capacity reflects the
severe right ventricular dysfunction.60-62 TEE is often used in hypoten- amount of air remaining in the alveoli at the completion of expiration.
sive patients to determine the cause of the hypotension, such as inad- As the functional residual capacity decreases, the alveoli collapse, and
equate filling or depressed contractility (Table 57-4). TEE can detect gas exchange decreases.67
other abnormalities, including left ventricular obstruction, structural Common causes for respiratory failure in pregnancy include
abnormalities, proximal pulmonary emboli, and valvular disease. It is pulmonary edema, asthma, infection, and pulmonary embolus.68,69
also useful in evaluating the left atrium and mitral valve because of the In a series of 43 gravidas requiring mechanical ventilation while
proximity of these structures to the transducer, and it appears to be undelivered, 86% delivered during the admission, and of these,
superior in evaluating congenital cardiac defects. 65% underwent cesarean section, with an associated mortality rate
Only a few small series have compared data derived from a PAC of 36% for those delivered by cesarean section. Overall maternal
with two-dimensional transthoracic and Doppler echocardiography in and perinatal mortality rates were high (14% and 11%,
obstetric patients. In one report of 12 patients requiring PAC for pre- respectively).68
eclampsia management, CO measured by Doppler echocardiography Debate continues about whether delivery improves respiratory
correlated well with CO assessed by thermodilution using a PAC.63 status in these patients. Tomlinson and coworkers70 described their
Another study of 16 obstetric patients found good correlation between experience with 10 patients who delivered while mechanically venti-
thermodilution assessment of CO and Doppler echocardiography.64 lated. In all but one patient, the cause of respiratory failure was pneu-
In a study of 11 critically ill obstetric patients, Belfort and colleagues65 monia.70 The only demonstrable benefit after delivery was a 28%
demonstrated no difference between Doppler echocardiographic and reduction in FIO2 in the ensuing 24 hours. The investigators concluded
PAC-derived estimation of stroke volume, CO, cardiac index, left ven- that routine delivery of these patients was not recommended. This is
tricular filling pressure, pulmonary artery systolic pressure, and right the only study published that was designed specifically to address this
atrial pressure.65 The data from these reports are encouraging, but question. However, data from other series support the conclusion that
echocardiographic estimation of pulmonary artery pressure was sig- delivery does not uniformly result in significant maternal improve-
nificantly overestimated in 32% of obstetric patients with suspected ment. Mortality rates after delivery while requiring ventilatory support
pulmonary artery hypertension.66 The technique appears to be well- range from 14% to 58%, and cesarean section may further increase this
tolerated, but further study is warranted. risk.68,69,71
TABLE 57-5 CHANGES IN ARTERIAL BLOOD
TABLE 57-4 ORIGIN OF HYPOTENSION
GAS MEASUREMENTS IN
End-Diastolic PREGNANCY
Cross-Sectional
Area Ejection Fraction Cause Measurements Pregnant Values Nonpregnant Values
Decreased >0.8 Hypovolemia pH 7.4-7.46 7.38-7.42
Increased <0.2 Left ventricular failure PCO2 (mm Hg) 26-32 38-45
Normal >0.5 Low SVR or severe MR, PO2 (mm Hg) 75-106 70-100
AR, or VSD HCO3− (mEq/L) 18-21 24-31
O2 saturation (%) 95-100 95-100
AR, aortic regurgitation; MR, mitral regurgitation; SVR, systemic
vascular resistance; VSD, ventricular septal defect. Modified from Dildy G, Clark SL, Phelan JP, et al: Maternal-fetal blood
From Cahalan MK: Intraoperative Transesophageal Echocardiography: gas physiology. In Critical Care Obstetrics, 4th ed. New York,
An Interactive Text and Atlas. New York, Churchill Livingstone, 1996. Blackwell, 2004.
8. 1174 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
ventilator-associated pneumonia was observed. However, no difference
Acute Respiratory Distress Syndrome in mortality was demonstrated by prone positioning.76 Only one study
Acute respiratory distress syndrome (ARDS) is characterized by rapid has shown a mortality benefit with early and prolonged prone posi-
onset of progressive respiratory distress. Evaluation reveals bilateral tioning of ARDS patients. The major difference in this study was the
pulmonary infiltrates without evidence of cardiac failure or increased length of time patients were maintained prone—on average 17 hours
hydrostatic pressure (i.e., PCWP < 18 mm Hg). These patients require daily for a mean of 10 days. The 136 patients were randomized within
high concentrations of oxygen and frequently need intubation. ARDS 48 hours of intubation.77
is also defined by a diminished ratio of the partial pressure of oxygen Prone positioning can be accomplished manually or with a special
to the fraction of inspired oxygen (PaO2/FIO2 200). If the ratio falls bed designed to rotate the patient. Complications related to prone
between 200 and 300, acute lung injury is present that is not severe positioning include pressure sores, endotracheal tube displacement or
enough to be called ARDS. obstruction, loss of venous access, vomiting, and edema. Data on prone
In pregnant women, infections with varicella or herpes simplex ventilation in the pregnant patient are lacking. Anticipated problems
virus, severe preeclampsia, eclampsia, and hemorrhage most com- include the gravid abdomen and difficulties in accomplishing fetal
monly precipitate respiratory failure.68,72 Septic patients are at par- monitoring while prone.
ticular risk for developing acute pulmonary injury and ARDS as a
consequence of pulmonary vascular damage that facilitates the leakage
of intravascular fluid into the pulmonary interstitial spaces. Mortality Pulmonary Edema
rates are quite high, and patients who survive often have pulmonary Pregnant women are predisposed to developing pulmonary edema for
function compromised by fibrosis and scarring of pulmonary tissue. various reasons, including increased plasma volume and CO in con-
The treatment of ARDS focuses on identifying and treating under- junction with decreased colloid oncotic pressure (COP), which occurs
lying causes such as infection and then providing respiratory, hemo- normally over the course of pregnancy. Alterations in the balance of
dynamic, and nutritional support to facilitate lung healing. Respiratory hydrostatic and oncotic pressure between the pulmonary vessels and
support may precipitate additional lung injury, and efforts to maintain the interstitial spaces can lead to an egress of fluid from the vascular
adequate oxygen delivery should also minimize lung trauma in an space into the interstitium and manifest clinically as pulmonary edema.
effort to facilitate healing of the lungs. Approximately 1 in 1000 pregnancies is complicated by pulmonary
Management of respiratory failure in nonpregnant, critically ill edema. In a review of almost 63,000 pregnancies, Sciscione and
patients has historically used a goal of maintaining a tidal volume of coworkers78 reported pulmonary edema occurring most often during
10 to 15 mL/kg. In ARDS, high tidal volumes may lead to alveolar the antepartum period (47%), with 39% occurring in the postpartum
overdistention or repeated recruitment and collapse of alveoli, predis- period and the remaining 14% in the intrapartum period.78 In this
posing to alveolar damage and release of inflammatory mediators that series, the two most common attributable causes of pulmonary edema
worsen pulmonary damage. In 2000, the ARDSNet published results were cardiac disease and tocolytic use (25.5% each). The remaining
of 861 patients with ARDS randomized to traditional tidal volumes cases of pulmonary edema were caused by fluid overload (21.5%) and
(12 mL/kg) or to a low tidal volume of 6 mL/kg.73 The traditional tidal preeclampsia (18%). The management of patients with pulmonary
volume group also maintained a goal of 50 cm of H2O or less, com- edema is focused on establishing the diagnosis, determining the cause,
pared with lower peak pressures of 30 cm of H2O in the low tidal and improving oxygenation.
volume group. Low tidal volumes and lower peak pressures were asso-
ciated with lower mortality rates (31% versus 40%) and shorter periods
of intubation compared with conventional tidal volumes and peak
Colloid Oncotic Pressure
pressure goals. Increased tidal volume and other normal changes in Abnormalities
pulmonary physiology may affect the utility of this approach in preg- Four forces affect fluid balance between vascular and interstitial spaces.
nant women. The COP is the force exerted primarily by albumin and other proteins
within the capillary, which holds fluid within the vascular space. The
oncotic pressure within the interstitial space also works to hold fluid
Prone Ventilation in the interstitium. Hydrostatic forces within the vessel and the inter-
Mechanical ventilation in the prone position has improved oxygen- stitium exert the opposite effect.
ation in up to 80% of patients with ARDS and acute lung injury. COP decreases over the course of pregnancy, and by term, it
Approximately 50% of patients maintain improved oxygenation after approximates 22 mm Hg.79 This is approximately 3 mm Hg lower than
they return to the supine position.74 Mechanical ventilation in the pre-pregnancy values as a result of the dilutional effect from plasma
prone position is believed to achieve several beneficial physiologic expansion. An isolated decrease in oncotic pressure, as may occur in
changes: improved aeration of well-perfused dorsal atelectatic lung pregnancy or in patients with nephrotic syndrome, is usually well
areas, improved alveolar recruitment, relief of cardiac compression on compensated and does not lead to pulmonary edema unless compli-
the lung posteriorly, and improved mobilization of secretions. cated by additional factors such as increased intravascular pressure or
Several randomized trials have compared supine with prone posi- pulmonary injury resulting in vascular permeability.80 Excessive intra-
tioning in nonpregnant patients with ARDS and acute lung injury. In venous fluids, blood loss, decreasing COP after delivery, and the post-
one randomized trial of 304 patients, prone positioning maintained partum autotransfusion effect can place patients at further increased
for an average of 7 hours daily was not associated with a decrease in risk for pulmonary edema.
mortality, but significant improvement in oxygenation was observed
in 70% of patients, with most of the benefit occurring in the first hour
of prone positioning.75 Another multicenter, randomized trial of
Hydrostatic or Cardiogenic
791 patients with hypoxemic respiratory failure with multiple causes, Pulmonary Edema
including ARDS, found similar results. In addition to improved oxy- Pulmonary edema due to primary cardiac issues with or without alter-
genation with prone positioning at least 6 hours daily, a decrease in ations in COP is referred to as hydrostatic or cardiogenic pulmonary
9. CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient 1175
edema. CO is controlled through continuous adjustments in heart states and neurogenic shock. In obstetric patients, shock most
rate and stroke volume. At some point, the heart is no longer able commonly results from hemorrhage and sepsis. Regardless of the
to increase the CO in response to increasing preload because of intrin- cause, therapy is directed at restoring tissue oxygenation by eliminating
sic cardiac abnormalities or excessive fluid administration, resulting in the originating cause, providing adequate volume replacement, and
overload. If left ventricular outflow is restricted, blood intended to improving cardiac function and circulation. Difficulty in reversing this
empty into the left atrium remains in the pulmonary vasculature, phenomenon explains the high mortality rates for patients with
which is reflected by the increased PCWP, left ventricular end-diastolic shock.
pressure, and pulmonary artery pressure. The net result is an increase
in the pulmonary intravascular hydrostatic pressure. When this pres-
sure exceeds the interstitial pressures, fluid is forced out of the pulmo- Sepsis and Septic Shock
nary vasculature into the interstitial spaces, resulting in pulmonary
edema. Incidence and Mortality
A transthoracic or transesophageal echocardiogram can distinguish Sepsis accounts for 9.3% of deaths occurring in the United States and
whether pulmonary edema is cardiogenic in origin. Evidence of poor complicates approximately 1 in 8000 deliveries.86 Fortunately, only a
ventricular systolic function is identified by a decreased ejection frac- small percentage of these deaths can be attributed to gynecologic or
tion, as seen in patients with a cardiomyopathy. Echocardiography may obstetric problems. Bacteremia is not uncommon in obstetric pati-
also identify valvular abnormalities that may lead to compromised ents, but these patients appear to be less likely to progress to septic
cardiac function and predispose patients to pulmonary edema, such as shock.59,87,88 An epidemiologic review of sepsis in the United States
aortic or mitral stenosis. gathered discharge data on more than 10 million cases of sepsis over
a 22-year period ending in 2000.89 According to this study, the inci-
dence of sepsis in the population is increasing at a rate of 8.7% annu-
Pulmonary Edema in the Setting ally. However, the percentage of pregnant women diagnosed with
of Preeclampsia sepsis in that period decreased by 50%, from 0.6% to 0.3%. African
Pulmonary edema develops in approximately 2.5% of patients with Americans and men appear to be at higher risk for developing sepsis,
preeclampsia, most commonly in the postpartum period.43,81,82 The but mortality rates did not appear to differ from those of whites and
cause is not completely understood, but it likely results from a combi- women, respectively.
nation of problems. Impaired left ventricular function may be a result Mortality rates overall have declined significantly to approximately
of chronic hypertension, particularly if it develops in the antepartum 17%, but the marked increase in sepsis diagnosis in the population
period. Substantially increased SVR may also impair left accounts for tripling of the rate of hospital death from sepsis. Between
ventricular function and lead to pulmonary edema, especially in the 1987 and 1997, infectious causes accounted for 13% of maternal
setting of iatrogenic fluid overload. Preeclamptic patients often lose deaths.10,11 Mortality rates associated with septic shock in pregnancy
significant amounts of albumin through the urine and exhibit decreased are uncertain and are derived primarily from older, small series of
albumin production, both of which can lower the COP. In preeclamp- cases, but they generally appear to be much lower than for the non-
tic patients, the COP can decrease to 18 mm Hg by term and drop pregnant population. Estimates range from 12% to 28% for obstetric
further after delivery to 14 mm Hg.43 Endothelial damage also leads to septic patients58,59,87,90 to 40% to 80% for the nongravid population.91
increased capillary permeability. Preeclamptic patients with pulmo- Improved outcomes for pregnant patients have been attributed to a
nary edema that fails to respond to oxygen, diuresis, and fluid restric- younger patient population, type of organisms, sites of infection more
tion, especially when combined with oliguria, may require pulmonary easily accessed and treated, and lower rates of coexistent diseases.
artery catheterization to guide further therapy. In a series of 10 patients
with severe preeclampsia who underwent placement of a PAC, the Definitions
findings varied. Five patients demonstrated a decreased gradient The American College of Chest Physicians and the Society of Critical
between the COP and PCWP, but two patients had a cardiac explana- Care Medicine published consensus guidelines in 1991 that were
tion for the pulmonary edema, and three patients had increased pul- designed to create consistency in the definitions used to describe septic
monary vascular permeability.83 conditions. Updated guidelines were published in 2003.57 These defini-
tions represent the understanding that these conditions exist along
a continuum of increasing severity while sharing a common patho-
Tocolytic-Induced Pulmonary Edema physiology. This continuum begins after the body develops a systemic
In the past, the use of parenteral β-agonists such as terbutaline and response to an infection and may progress to multiorgan dysfunction
ritodrine was more common and became associated with the develop- with hemodynamic instability and even death.
ment of pulmonary edema.78,84 However, as the use of intravenous The later classification system questions the utility of the diagnosis
β-agonists for tocolysis has decreased, the incidence of pulmonary of systemic inflammatory response syndrome (SIRS), suggesting that
edema related to tocolytic use appears to have diminished. Magne- the criteria previously set forth are too sensitive and nonspecific. SIRS
sium does not appear to independently increase the risk of pulmo- was defined as the clinical response to infection manifested by two
nary edema.85 or more of the following: temperature of 38° C or higher or 36° C or
lower; pulse of 90 beats/min or higher; respiration rate of 20 breaths/
min or higher or a PaCO2 less than 32 mm/Hg; or a white blood cell
Shock count of 12,000 or more or 4000 or less or more than 10% immature
neutrophils. When SIRS criteria are met and infection is confirmed or
Shock is the physiologic response to impaired tissue oxygenation. suspected, the patient is then considered to be septic. The latest guide-
Oxygen deficiency at the cellular level may result from inadequate lines expanded on this concept in the definitions (Table 57-6). These
delivery of oxygen, such as in hypovolemic states, cardiac failure, and definitions do not take into account the physiologic changes of preg-
hemorrhage or from improper uptake or use of oxygen, as in septic nancy and therefore may overdiagnose sepsis.
10. 1176 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
TABLE 57-6 DIAGNOSTIC CRITERIA OF SEPSIS summarized in Table 57-7. The initial phase is characterized by vaso-
SYNDROMES dilation, increased capillary permeability, and endothelial damage.
Clinically, the patient may have evidence of infection or fever and may
Condition Definition have positive blood cultures. Peripheral vasodilation causes flushing
and warm extremities. It also leads to a decrease in blood pressure with
Infection Pathologic process caused by the invasion of
diminished cardiac preload, which leads to a tachycardic response in
normally sterile tissue or fluid or body cavity by
pathogenic or potentially pathogenic an effort to maintain or increase the CO. Initial laboratory findings
microorganisms vary. An elevated white blood cell count may be followed by neutro-
Bacteremia Presence of bacteria in the bloodstream penia. Hyperglycemia is typical as a result of altered adrenal respon-
Sepsis Systemic inflammation accompanied by infection siveness, insulin resistance, and increased levels of catecholamines and
Severe sepsis Sepsis complicated by major organ dysfunction cortisol.
Septic shock Persistent unexplained arterial hypotension in the If uninterrupted, sepsis progresses and is characterized by intense
setting of severe sepsis vasoconstriction. This leads to poor perfusion, which is manifested by
cool extremities and altered organ function as a result of inadequate
Data from Levy MM, Fink MP, Marshall JC, et al: 2001 SCCM/ESICM/
ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care oxygenation (i.e., cold shock). Oliguria is typical, as are respiratory
Med 31:1250-1256, 2003. failure and ARDS. The CO decreases as a result of inadequate venous
return and increasing peripheral resistance. In the advanced stages of
septic shock (i.e., secondary or irreversible shock), symptoms progress
Gram-positive organisms have surpassed gram-negative organisms and reflect the global effects of inadequate tissue perfusion and oxy-
as the most common cause of sepsis in the general population, unlike genation: hypotension, respiratory failure, renal failure, DIC, myocar-
the situation for pregnant patients. Common organisms isolated from dial depression, electrolyte disturbances, obtundation, and metabolic
pregnant patients in septic shock include Escherichia coli, groups A and acidosis.
B streptococci, Klebsiella species, and Staphylococcus aureus.59 The
source of infection in pregnant women is typically the genitourinary Management
tract and includes lower urinary tract infections, pyelonephritis, cho- If the patient is at a viable gestational age and is undelivered with evi-
rioamnionitis, endometritis, and rarely, septic abortion, necrotizing dence of sepsis or septic shock, the fetal status should be monitored
fasciitis, and toxic shock syndrome.58,59,87,88,92 closely with continuous fetal heart rate monitoring and ultrasound
evaluation to estimate fetal weight, assess amniotic fluid volume,
Pathophysiology of Sepsis and confirm gestational age. Uterine perfusion and oxygenation are
Sepsis is a complex phenomenon that originates with invasion of the adversely affected as the sepsis progresses. Contractions are often
host by an offending organism. After infection, macrophages are encountered, possibly as a result of decreased uterine perfusion and
recruited, bind to the organism, and initiate a collection of responses decreased oxygen delivery to the myometrium. Tocolysis should be
resulting in the activation of the inflammatory and coagulation cas- undertaken with caution because the side effects of the medications
cades. Initially, the sepsis response was postulated to be the result (e.g., tachycardia, vasodilation) may impair physiologic adaptations to
of an exaggerated inflammatory response. Initial pharmacologic sepsis. If maternal status can be corrected and fetal status remains
approaches therefore targeted suppression of the inflammation process, reassuring, delivery can be avoided. The decision about whether to
including corticosteroids and agents to block cytokines such as proceed with delivery may be challenging, particularly if maternal
tumor necrosis factor α (TNF-α) and interleukin 1β (IL-1β).93 These status is deteriorating. The fetus may not tolerate labor because of poor
approaches have been largely unsuccessful, a testament to the uterine perfusion and maternal hypoxemia; conversely, the mother
complexity of the sepsis syndromes. The roles of anti-inflammatory may be too unstable to safely undergo a surgical procedure. If the
mediators and genetics in the sepsis cascade has been increasingly source of infection is the uterus, as in septic abortion or chorioamnio-
appreciated.94 Activation of the inflammatory cascade after infection nitis, evacuation of the uterus is necessary.
causes release of interleukins, tumor necrosis factors, interferons, pros- Sepsis management has several goals:
taglandins, platelet-activation factor, oxygen free radicals, nitric oxide,
complement, and fibrinolysins.95 Identification of the source of infection
Hemostatic mechanisms are also affected in severe sepsis. Initiation Institution of empiric antibiotic therapy
of the clotting cascade results from macrophages and monocytes Early, aggressive improvement in circulating volume
involved in production of inflammatory mediators. Endothelial damage Optimization of hemodynamic performance
also contributes to the procoagulant effect, causing platelet activation Maintenance of oxygenation
and suppression of protein C activity. These derangements in the Volume resuscitation
hemostatic balance lead to clotting factor consumption, fibrin deposi-
tion, thrombin generation, and decreased platelet levels.96 The resultant Aggressive fluid replacement to improve circulating intravascular
microthrombi are thought to negatively affect end-organ damage and volume is a mainstay of sepsis management and has improved CO,
contribute to the clinical features of severe sepsis and septic shock, such oxygen delivery, and survival. Studies have demonstrated a survival
as oliguria, ARDS, and hepatic dysfunction. In severe cases, consump- benefit for patients with septic shock managed with protocol-driven,
tion of clotting factors is substantial enough to cause hemorrhagic early, aggressive volume resuscitation. Early goal-directed therapy
complications from DIC. Figure 57-6 outlines the sepsis cascade. (EGDT) involves tailoring treatments and resuscitative efforts to
achieve specified endpoints, which include normal mixed venous
Clinical Manifestations oxygen saturation, arterial lactate concentration, base deficit, and pH
Septic shock has been classified as three progressive clinical stages: in an effort to reduce end-organ dysfunction and ultimately reduce
warm shock, cold shock, and irreversible (secondary) shock, which are mortality.
11. CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient 1177
Bacterial products
and components
Macrophage
TNF-a
Activation of coagulation IL-1
and complement system IL-6
Tissue factor release PAF
Fibrinolytic activity NO
etc.
Neutrophil activation, Platelet activation, Metabolism of T-cell release of
aggregation, aggregation arachidonic acid IL-2, INF-g,
degranulation Release of GM-CSF
Release of O2 radicals thromboxane A,
and proteases PGS, LTS
Endothelial damage
Tissue injury
Organ dysfunction
FIGURE 57-6 The sepsis cascade. Hemostatic mechanisms are affected in patients with severe sepsis,
and derangements in the hemostatic balance lead to clotting factor consumption, fibrin deposition, thrombin
generation, decreased platelets, tissue injury, and organ dysfunction. GM-CSF, granulocyte-macrophage
colony-stimulating factor; IL, interleukin; LTS, leukotrienes; NO, nitric oxide; PAF, platelet-activating factor;
PGS, prostaglandin synthesis; TNF-α, tumor necrosis factor α. (Modified from Bone RC: The pathogenesis of
sepsis. Ann Intern Med 115:457-469, 1991.)
TABLE 57-7 STAGES OF SHOCK
Warm (Early) Shock Cold (Late) Shock Secondary (Irreversible) Shock
Flushing Cyanosis Renal failure
Warm extremities Cool extremities Disseminated intravascular coagulopathy
Rapid capillary refill Delayed capillary refill Myocardial failure
Decreased mental status Increased vascular resistance Refractory hypotension
Hypotension Decreased cardiac output Obtundation
Increased cardiac output Respiratory failure or adult respiratory distress syndrome
Tachycardia Oliguria
Tachypnea
In 2001, Rivers and colleagues97 published the results of a prospec- 12 mm Hg. The volume of fluid administered to both groups of
tive, randomized trial of EGDT compared with standard therapy for patients was similar in the first 72 hours (>13 L), but the EGDT group
patients in septic shock in a single institution. Therapy for patients received more volume in the initial 6 hours of therapy (5 versus
in the EGDT group was initiated in the emergency room setting 3.5 L). This aggressive approach decreased the mortality rate by 16%
before transfer to the intensive care unit and included placement (30.5% versus 46.5%).
of central venous catheters with the ability to measure continuous Clinicians have questioned whether modification of this protocol,
venous oxygen saturation (SCvO2). An elevated SCvO2 value reflects particularly elimination of continuous venous oxygen saturation
inadequate perfusion and uptake of oxygen in the tissues. Red blood (SCvO2), could produce similar results. In 2006, Lin and coworkers98
cell transfusions were administered to maintain the hematocrit at randomized patients to EGDT without measurement of SCvO2 and
30% or higher, and inotropic agents were added if the SCvO2 level was confirmed survival benefit. Patients randomized to receive modified
inadequately corrected (<70%). The protocol called for a 500-mL EGDT were significantly less likely to die (71.6% versus 53.7%), spent
crystalloid bolus every 30 minutes until the CVP reached 8 to fewer days in the hospital, were intubated for a shorter time, and were
12. 1178 CHAPTER 57 Intensive Care Monitoring of the Critically Ill Pregnant Patient
at less risk for developing sepsis-associated central nervous system and infection are the uterus and genitourinary tract, and gram-negative
renal dysfunction compared with controls. bacteria constitute the primary organisms. In the non-obstetric popu-
Because of the encouraging survival and morbidity data, EGDT is lation, gram-positive organisms represent most of the organisms iso-
being widely adopted in the management of severe sepsis, but it remains lated in septic patients, followed closely by gram-negative bacteria.89
to be confirmed whether this approach will produce similarly improved Cultures should be collected from blood and any suspected site, includ-
outcomes in a pregnant population. The precise goals to appropriately ing the uterus if necessary, for identification of the organism and
guide therapy in a pregnant population also must be defined. determination of antibiotic sensitivities. Empiric antimicrobial therapy
targeted at the suspected organism should not be delayed pending
Optimization of Hemodynamic Performance culture results.100-103
In addition to replacing intravascular volume to improve perfusion In an obstetric and postpartum population, antibiotic coverage
and cardiac preload, early pharmacologic interventions to improve usually consists of β-lactam antibiotics (i.e., penicillins, cephalospo-
vascular tone, cardiac contractility, and cardiac preload confer a rins, carbapenems, and monobactams) with or without an aminogly-
considerable survival advantage.97,98 If the patient fails to respond coside (see Chapter 38). Monotherapy with a carbapenem or third- or
appropriately to aggressive fluid resuscitation efforts, vasopressors are fourth-generation cephalosporin is as effective as a β-lactam antibiotic
indicated to improve vascular tone, resulting in improved cardiac in combination with an aminoglycoside in non-neutropenic patients
return and CO, peripheral perfusion, and oxygen delivery. In the initial with severe sepsis.104 In undelivered patients, tetracycline derivatives
publication on EGDT, the requirement for vasopressors was signifi- and quinolones should be avoided. When culture results become avail-
cantly diminished by early, aggressive fluid resuscitation (37% versus able, antibiotic therapy can be adjusted if necessary.
51%), but there was no difference in the requirement for inotropic After appropriate antibiotic therapy has been initiated and the
agents between the two groups (9% versus 15%).97 In this study, vaso- process of stabilization of the patient has begun, attention should be
pressors were initiated to maintain mean arterial pressure above directed to source control. This entails removal of indwelling lines and
65 mm Hg. Use of a similar protocol minimized the delay in initiation catheters, with replacement if necessary. Indications for more aggres-
of vasopressors and reduce mortality.98 sive surgical approaches are less clearly defined. Generally, more inva-
Dopamine hydrochloride is the most commonly employed first- sive surgical approaches are not emergent and can be accomplished
line vasopressor in the intensive care setting. Dopamine’s α- and β- after the condition of the patient has stabilized.105 Exceptions are infec-
adrenergic effects are dose dependent. Low doses (<10 μg/kg/min) tions involving clostridia and group A streptococci, such as necrotizing
improve myocardial contractility, CO, and renal perfusion without fasciitis. In this scenario, delay in excision of affected tissues can have
negatively affecting myocardial oxygen consumption. As the dose a dramatic negative effect on the patient’s condition.106 Evaluation of
increases (>20 mg/kg/min), α-adrenergic effects predominate, result- the abdomen by ultrasound or computed tomography (CT) can assist
ing in increasing SVR in addition to increased CO. In a viable gestation in identification of an intra-abdominal abscess. When drainage of an
requiring vasopressor support, fetal monitoring is essential because intra-abdominal abscess is necessary, the percutaneous approach is
dopamine has decreased uterine perfusion in an animal model.99 preferable. In obstetric conditions, evacuation of the uterus by suction
Dobutamine is similar to dopamine, but it has primarily β1-adrenergic curettage in septic abortion or delivery of the neonate in viable gesta-
effects. Dobutamine therefore improves CO with minimal impact on tions should occur after initiation of antibiotics and stabilization of
heart rate or vascular resistance. In the EGDT protocol, dobutamine the patient. Postpartum hysterectomy may be necessary if the patient
was used to improve oxygen consumption in patients who failed to fails to respond to antibiotics and the uterus is the suspected source.
respond to fluid resuscitation, dopamine infusion to improve mean
arterial pressure, and red cell transfusion to correct anemia.97 Table Adjunctive Therapies in Sepsis Management
57-8 lists other commonly used vasopressor agents for the manage- INSULIN THERAPY
ment of severe sepsis and septic shock. In the critically ill population, hyperglycemia is a common phe-
nomenon attributable to insulin resistance and escalations in glucagon,
Source Control and Antimicrobial Therapy cortisol, and catecholamine levels, which promote glycogenolysis and
Prompt identification of the probable source of infection is essential gluconeogenesis.107 In 2001, Van den Berghe and colleagues108 pub-
to initiate appropriate antimicrobial therapy and improve outcomes lished a large, prospective, randomized trial that demonstrated that
for septic patients. In an obstetric population, common sources of tight glycemic control (blood glucose level of 80 to 110 mg/dL) in
critically ill patients decreased overall mortality by 34%. Septic patients
exhibited an even more impressive 76% reduction in mortality as a
TABLE 57-8 INOTROPIC DRUGS FOR result of aggressive euglycemia with insulin therapy.108 Other signifi-
MANAGEMENT OF SHOCK cant benefits of tight glycemic control included fewer ventilator days,
less time in the ICU, decrease risk for developing septicemia, and a
Agent Dose Hemodynamic Effect reduced need for dialysis.
Dopamine Pregnant women demonstrate insulin resistance and to have higher
Low dose <10 μg/kg/min ↑ CO, vasodilation of renal circulating insulin levels than their nonpregnant counterparts. They
arteries are also predisposed to developing fasting hypoglycemia because of
High dose 10-20 μg/kg/min ↑ CO, ↑ SVR higher levels of insulin and continuous delivery of glucose to the fetus.
Dobutamine 2.5-15 μg/kg/min ↑ CO, ↓ SVR or ↑ SVR However, the impact of aggressive euglycemia in the critically ill preg-
Phenylephrine 40-180 μg/min ↑ SVR nant patient remains to be studied.
Norepinephrine 2-12 μg/min ↑ CO, ↑ SVR
Isoproterenol 0.5-5 μg/min ↓ CO, ↑ SVR
CORTICOSTEROIDS
CO, cardiac output; SVR, systemic vascular resistance; ≠, increase; Ø, Empiric administration of corticosteroids in high doses does not
decrease. improve survival of unselected septic patients and may worsen out-