Bombings Injury Patterns And Care Pocket Guide
•
2 gefällt mir•1,017 views

This document provides guidance on injury patterns, triage considerations, and treatment for victims of bombings and explosions. It discusses primary, secondary, tertiary, and quaternary blast injuries as well as crush injuries, compartment syndrome, and blast lung injury. Specific injuries covered include head injuries, ear injuries, abdominal injuries, burns, and fractures. The document emphasizes the importance of assessing for and treating multiple or combined injuries in blast victims. It provides considerations for scene safety, triage, fluid resuscitation, monitoring, and disposition of patients following explosive events.

Empfohlen
Weitere ähnliche Inhalte
Andere mochten auch
Andere mochten auch (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Bombings Injury Patterns And Care Pocket Guide
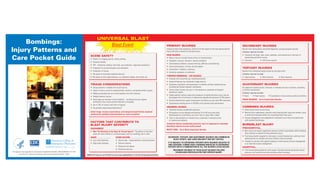
- 1. UNIVERSAL BLAST Bombings: Blast Event PRIMARY INJURIES SECONDARY INJURIES Injury Patterns and Unique to high-order explosives; results from the impact of the over-pressurization Results from flying debris and bomb fragments causing shrapnel wounds. wave with body surfaces by the blast wave. Common injuries include: Care Pocket Guide HEAD INJURIES • Trauma to the head, neck, chest, abdomen, and extremities in the form of SCENE SAFETY penetrating and blunt trauma. • May or may not include history of loss of consciousness • Check in at staging area for safety briefing. • Fractures • Soft tissue injuries • Headache, seizures, dizziness, memory problems • Personnel safety • Gait/balance problems, nausea/vomiting, difficulty concentrating. • PPE – Protective clothing, hard hats, eye protection, respiratory protection. • Visual disturbances, tinnitus, slurred speech. TERTIARY INJURIES • Protection of uninvolved public and volunteers. • Disoriented, irritability, confusion. • Protection of injured. Results from individuals being thrown by the blast wind. • Extremity weakness or numbness. Common injuries include: • Be aware of secondary explosive devices. TYMPANIC MEMBRANE – EAR INJURIES • Be aware of multi-agent devices, e.g. chemical release, dirty bomb, etc. • Head injuries • Skull fractures • Bone fractures • Evaluate and resuscitate per standing protocols. • Impaired hearing may complicate triage process. QUATERNARY INJURIES TRIAGE CONSIDERATIONS • Secondary evaluation and examination to identify all blast-related injuries including perforated tympanic membranes. All explosion-related injuries, illnesses, or diseases not due to primary, secondary, • Unique patterns, multiple and occult injuries. • Serious blast injuries can occur in the absence or presence of tympanic or tertiary mechanisms. • Death is often a result of combined blast, ballistic, and thermal effect injuries. membrane rupture. Common injuries include: • Walking wounded and non-critical patients are time intensive. • Stable patients without signs and symptoms of significant blast injury, may be • Burns • Head injuries • Exacerbation of pre-existing medical conditions • Hidden/internal injuries discharged after 4 to 6 hours of observation despite the presence of TM rupture. CRUSH INJURIES – Go to Crush Injury Section • Overtriage can increase critical mortality – resulting from poor patient • Patients should have urgent consultation and follow up care with ENT specialist. distribution from scene and self-referrals to hospitals. • Spontaneous healing occurs in 50-80% of all patients with perforations. • Up to 75% of victims self-refer to hospital. COMBINED INJURIES ABDOMINAL INJURIES • Do patients require decontamination? • Treatment follows established protocols. • Avoid tunnel vision on one injury. Initial triage, trauma resuscitation, and transport should follow standard • Monitor fluid replacement amounts when treating blast lung with another injury • Perforations can be delayed and develop 24 to 48 hours post blast. protocols for multiple injured patients or mass casualties. to avoid fluid overload which can exacerbate blast lung injury. Manifestations of peritonitis can occur hours or days after a blast. • Airway management and oxygenation/ ventilation are critical and performed • There is the possibility of missed injury, especially in semiconscious with standard techniques. or unconscious patients. FACTORS THAT CONTRIBUTE TO Treatment follows established protocols, but it is important to remember BURN/BLAST INJURY BLAST INJURY SEVERITY that these injuries may be easily missed. PREHOSPITAL ENVIRONMENT BLAST LUNG – Go to Blast Lung Injury Section • Burn injury will require significant amounts of fluid resuscitation while avoiding • Was The Bombing In An Open Or Closed Space? The effects of the blast fluid overload to prevent further pulmonary injury. wave are more intense in a confined space such as a building, bus or train. • Fluid resuscitation targeted to vital signs, to avoid hypotension; judicious fluid SECONDARY, TERTIARY, AND QUATERNARY INJURIES ARE COMMON IN AGENT OTHER FACTORS administration to maintain perfusion without volume overload. BLAST EVENTS, AND LARGE MAJORITY ARE NOT CRITICAL. • Low-order Explosive • Device type – large (vehicle) or small (suitcase) • Transfer to a facility with specific expertise in both trauma and burn management, IT IS UNLIKELY TO EXPERIENCE PATIENTS WITH INJURIES ISOLATED TO • High-order Explosive • Delivery method or at least the trauma management. ONE CATEGORY. A MORE LIKELY SCENARIO WOULD BE TO EXPERIENCE • Distance from device PATIENTS WITH A COMBINATION OF ALL THE INJURIES LISTED BELOW. HOSPITAL ™ • Protective barriers • Fluid resuscitation guided by urine output. Consider monitoring central venous TREATMENT FOR MOST OF THESE BLAST INJURIES FOLLOWS This project was supported by Cooperative Agreement Number U38/CCU624161-01-3107 ESTABLISHED PROTOCOLS FOR THAT SPECIFIC INJURY. pressure, and systemic vascular resistance when indicated. from the U.S. Centers for Disease Control and Prevention (CDC). 10/07 Additional resources can be found at: www.acep.org/blastinjury or www.bt.cdc.gov/masscasualties/
- 2. CRUSH INJURY BLAST LUNG INJURY Blast Event Blast Event MANAGEMENT FIELD AMPUTATION OXYGENATION INDICATED? Field Amputation • High flow O2 sufficient to prevent hypoxemia via non-rebreather mask, CPAP, or ENTRAPPED PATIENT TREATMENT INITIAL TRIAGE, TRAUMA RESUSCITATION, AND TRANSPORT INDICATIONS • Best performed by an endotracheal intubation. SHOULD FOLLOW STANDARD PROTOCOLS FOR MULTIPLE • Fluid resuscitation before extrication • Consider alkalinization appropriately trained • Inability to safely extricate the patient. • Hemothorax or Pneumothorax INJURED PATIENTS OR MASS CASUALTIES u 1 L NS bolus, 1-1.5 L/hr infusion u ampule Sodium Bicarbonate (50 mEq) 1 physician, such as a trauma • Continued environmental toxins that CLOSE OBSERVATION prior to extrication, followed by 1 ampule of Was the Bombing in an Open or Closed Space? or orthopedic surgeon. • Limb Stabilization pose a hazard to victims or rescuers. Sodium Bicarbonate with each liter of NS • Chest decompression for clinical presentation of tension pneumothorax. There is a higher incidence of blast lung injury in enclosed spaces • Ensure adequate analgesia • Minimize potential systemic effects • When the extrication time would be infused at 1-1.5 L/hr. Maintain a second IV • Fluid administration and anesthesia. w/o Sodium Bicarbonate. of reperfusion (tourniquets) long enough that it would endanger the • Provide enough fluid to ensure tissue perfusion but avoiding volume overload. patient’s life without field amputation. AIR EMBOLISM* Vital signs, oxygen, EKG, IV — Additional treatment and transport SIGNS OR SYMPTOMS SUGGESTIVE • Position in prone, semi-left lateral, or left lateral positions; transport to a facility NO CRUSH INJURY TREATMENT – PREHOSPITAL OF BLI OR RESPIRATORY DISTRESS with a hyperbaric chamber. CRUSH SYNDROME *Close observation for any patient suspected of BLI for the development of tension SIGNS – Apnea, tachypnea or hypopnea, hypoxia and cyanosis, cough, IS CRUSH SYNDROME OR COMPARTMENT • Primary survey and initial stabilization (ABCs) pneumothorax transported by air. wheezing, dullness to percussion, decreased breath sounds, or hemoptysis SYNDROME SUSPECTED? • Fluid resuscitation before patient is extricated with severe or SYMPTOMS – Dyspnea, hemoptysis, cough, and chest pain prolonged entrapment of limb or pelvis (more than a hand or foot). Areas commonly affected: • Lower/ Upper extremities • Pelvis CLINICAL CONCERNS – Blast lung, hemothorax, pneumothorax, pulmonary COMPARTMENT SYNDROME HOSPITAL DIAGNOSTIC EVALUATION • Gluteal region • Abdominal muscles contusion and hemorrhage, A-V fistulas (source of air embolism), penetrating • Primary survey and initial stabilization (ABCs) chest trauma, and blunt chest trauma. Evaluate patient for >10% BSA burns, • Chest radiography • Suspect compartment syndrome due to mechanisms of injury, examination, skull fractures, and penetrating torso or head injuries • Arterial blood gases, computed tomography, and doppler ultrasound can be used to SIGNS AND PRESENTATION SIGNS OF COMPARTMENT and patient complaints. help diagnose BLI and air emboli. OF CRUSH SYNDROME SYNDROME • Treat other injuries • Most lab and diagnostic testing conducted per resuscitation protocols – based upon The general condition of a patient Pain, Pallor, Paresthesia, Paralysis, • Immobilize affected part; do not use constricting bandages or MAST trousers. with crush injury is dictated by: Pulselessness Progression of symptoms nature of explosion (e.g. confined space, fire, etc.). COMPROMISED (1) other injuries, (2) delay in extrication, (the 6th P) NO YES and (3) environmental conditions. VENTILATION Clinical concerns: CRUSH INJURY TREATMENT – HOSPITAL Common presentations are: • Bone fractures with extravasation of blood HOSPITAL DISPOSITION AND OUTCOME CRUSH SYNDROME • Hypothermia or hyperthermia or edema within a closed compartment. • Fluid resuscitation • Brisk diuresis (2 ml/kg/hr) • No definitive guidelines for observation, admission, or discharge following emergency dehydration/shock • High velocity penetrating injury to muscles department evaluation for patients with possible BLI following an explosion. • Diagnose and treat other • Pain control • Mental status varies from alert to comatose in closed compartment with extensive Vital Signs, Oxygen, Monitor IV tissue disruption. metabolic derangements: • Patients diagnosed with BLI may require complex management and should be • Anxiolysis Clinical concerns: u Hyperkalemia • Can also occur in sub acute fashion due to admitted to an intensive care unit. Patients with any complaints or findings • The systemic effects are due to prolonged immobilization on hard surface. u Hypocalcemia suspicious for BLI should be observed in the hospital. rhabdomyolysis and reperfusion of Airway Management hypoxic and damaged tissues. • Compartment syndrome typically occurs in COMPARTMENT SYNDROME • Discharge decisions will also depend on associated injuries; other issues related Protocol major muscle groups enclosed by inelastic, • Reperfusion of body part results in to the event, including the patient’s current social situation. • Primary survey, stabilization and • If injury is open: fibrous sheaths. If ventilatory failure occurs or the systemic effects of crush injury. resuscitation, secondary survey. • In general, patients with normal chest radiographs, blood gasses, and pulse u Antibiotics, tetanus, jet irrigation. is imminent, patients should be • Principal areas for compartment syndrome • Patients may appear well until extricated, • Diagnosis through examination oximetry who have no complaints suggesting a BLI, can be considered for u Debridement of nonviable tissues. Appropriate are upper extremities, including thenar and intubated; caution should be used and then precipitously decompensate. and confirmation with compartment discharge after 4-6 hours of observation. hypothenar eminences of hand, and lower u arly amputation for severely E as positive pressure and mechanical Treatment • Skeletal muscle damage is greatest pressure measurements. extremities, including the foot. ventilation may increase the risk of injured limbs may be required to • Data on the short and long-term outcomes of patients with BLI is currently limited. after reperfusion. and Transport • Treat systemic effects of compartment further pulmonary injury • Untreated compartment syndrome will reduce sepsis. However, in one study conducted on survivors one year post injury, no patients had • Cardiovascular instability due to massive produce the same effects as a crush injury. syndrome similar to crush injury. pulmonary complaints, all had normal physical examinations and chest radiographs, • Fasciotomy fluid shift, electrolyte abnormalities, and and most had normal pulmonary function tests. direct myocardial toxicity. Additional resources can be found at: www.acep.org/blastinjury or www.bt.cdc.gov/masscasualties/ Additional resources can be found at: www.acep.org/blastinjury or www.bt.cdc.gov/masscasualties/