Fetal circulation
•
6 gefällt mir•762 views

FETAL CIRCULATION -CHANGES AT BIRTH / IMPLICATIONS IN CHD

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Fetal circulation
Ähnlich wie Fetal circulation (20)
Mehr von Adhi Arya
Mehr von Adhi Arya (9)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Fetal circulation
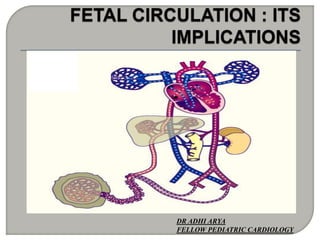
- 1. DR ADHI ARYA FELLOW PEDIATRIC CARDIOLOGY
- 2. Circulation undergoes continuous maturation during gestation, both morphologically and functionally, and these changes during development may be greatly influenced by congenital cardiac lesions Knowledge of fetal circulation is important to our understanding of the manner in which various CHD influence the normal circulation. Clinical manifestations of congenital heart disease are intimately related to postnatal changes in the circulation
- 3. Fetal circulation Implications in congenital malformations
- 4. History Difference from neonatal/adult circulation Salient features of fetal circulation Normal flow/Anatomic shunts/ Admixture sites Concept of CVO/ distribution of CVO Factors affecting fetal CO and its response to decreased CO
- 6. Based on studies done on fetal lambs Fetal USG Fetal MRI •Course and distribution same •Quantities of blood ejected by ventricles and distributed to various organs different •Different gestation periods/ proportion to organs /12% vs 3%
- 7. Fetal USG •Based on flow velocities and vessel diameter. •Heterogenous because of measurements at different sites and inter-observer variation . •Diameter is squared , even small errors lead to big errors in flow calculation
- 8. FETAL POSTNATAL GAS EXCAHNGE PLACENTA LUNGS RV/LV CIRCUIT PARALLEL SERIES DOMINANT VENTRICLE RV RVLV FETAL MYOCARDIUM LESS CONTRACTILE ELEMENTS LESS COMPLIANT ADMIXTURE SITES IVC/LA R-L L-R Shunts NONE
- 9. Unique features of myocardium Preferential streaming within the IVC between liver and heart Functional separation of aorta at isthmus Higher O2 saturation in left hepatic venous blood Stiffness and impaired relaxation of the fetal myocardium---reflected in pattern of Doppler echocardiography across the AV valves
- 12. Gives Br to L lobe , divides in to DV and arcuate branch Portal vein joins arcuate Branch supplies rt side RHV enters IVC separately LHV joins DV and enters IVC SVC blood to RV – tubercle of Lower
- 13. Streaming in IVC , DV vel-55 cm/s RHV blood 15 cm/s
- 14. IVC LA L->R( UV blood returning to placenta without being given to fetal body) R->L ( Blood from SVC or IVC distributed to body without being delivered to placenta ) 45% of SVC blood, 53% of IVC blood
- 15. Left to right and right to left shunts in fetus constitute 33% of CVO of fetal heart
- 16. In fetus, blood distributed to palcenta and to various parts of body –derived from systemic as well as umblical venous return Blood to organs derived from both ventricles So expressed as CVO
- 24. Effects studied on fetal lambs Heart rate –Pacing/ Vagal stimulation Preload/Afterload Myocardial contractility Baroreceptors /chemoreceptors
- 25. PACING RA Pacing 250-300 LVO 15 % inc, no eff on RVO. Rates > 300 output fell, progressively LA pacing LVO reduced by 50%;RVO inc LA pressure exceeds RA and flow across foramen ovale hampered, reducing LVO
- 26. VAGAL STIMULATION Vagal stimulation inc SVR( inc afterload) , inc intrapleural pressure( dec VR)--decreases CVO So fall in CO is also due to associated changes not only decr HR
- 27. Fetal heart is normally operating near the top of its ventricular function curve, so that a fall in preload results in a decrease in output. Second alternate theory is of ventricular constraints due to extrinsic compression of fetal heart
- 28. At constant arterial pressure levels, progressive elevation of left atrial pressure increased left ventricular stroke volume even with atrial pressures as high as 10–15 mmHg
- 29. Few sarcomeres Parallal arrangement of myofibrils absent T tubule system less developed Poor sympathetic innervation Beta receptor concentration variable So in cases of fetal bradycardia, SV cannot be increased much
- 30. Mature with advancing gestation Baroreceptors induced by arterial HT— bradycardia, vasodilation Chemoreceptor by hypoxemia— brady(reflexly induced by vagal stimulation)
- 31. Acute hypoxemia –brady(vagal) and HT( catecholamine induced) <12mm Hg- depressent effect on myocardium Chronic – resetting of chemoreceptor sensitivity—HR increases but not fully Increased systemic venous pressures – HYDROPS
- 32. Hydrops (inc systemic venous pressure) Obstruction Volume of blood flow Blood oxygen content
- 35. DA obstruction- pulmonary circulation Maternal NSAIDs Increased PA pressure Increased pulmonary vascular smooth muscles PPHN
- 36. Aortic arch obstruction COA Neurodevelopmental problems
- 37. 1.Ventricular development: inflow or outflow reduction Inflow reduction: hypoplastic chamber (FO, mitral atresia) Outflow obstruction(AS/PS): ESV inc , atrial filling pressure increase, hypertrophy, foramen ovale diverts the venous return to normal ventricle, CVO is maintained
- 38. 2.Ascending aorta and arch 10% CVO passes through isthmus Aortic atresia: no forward flow, hypoplastic arch Pulm atresia: entire CVO through aorta, dilated ascending aorta 3.Ductus size and angle Aortic atresia :Wide oblique inferior angle/ inc size Pulm atresia:Acute inferior angle / dec size
- 40. Aortopulmonary transposition Ascending aortic blood flow desaturation, cerebral malformations Pulmonary blood flow has high oxygen content, pulmonary vasodilation, increased PBF, increased venous return to LA, LA pressure higher, flap of foramen ovale shifted to right Oxygenated blood from PA passing through ductus causes its constriction
Hinweis der Redaktion
- Pulmonary blood flow is represented by RVO minus ductus arteriosus flow. Pulmonary blood flow has also been calculated from direct measurement of right and left branch pulmonary arteries insome studies
- Pulmonary blood flow is represented by RVO minus ductus arteriosus flow. Pulmonary blood flow has also been calculated from direct measurement of right and left branch pulmonary arteries insome studies
- Pulmonary blood flow is represented by RVO minus ductus arteriosus flow. Pulmonary blood flow has also been calculated from direct measurement of right and left branch pulmonary arteries insome studies
- (Blood going from RV->PA to Des Ao through PDA – none of this passes retrograde to ascending aorta)