GERD ( Gasrtro-esophageal reflux disease )
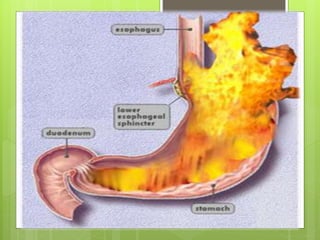
Gastroesophageal reflux disease (GERD) is a condition in which the stomach contents (food or liquid) leak backwards from the stomach into the esophagus (the tube from the mouth to the stomach). This action can irritate the esophagus, causing heartburn and other symptoms.
And Case study at the end
6. What is GERD
GERD states it is a condition that occurs
when the refluxed stomach contents lead
to trouble.
Disorder in lower esophagus sphincter
GERD affects all ages especially after 40
years
7. The gender doesn't play a role in the
disease .
The mortality of GERD is rare .
Death occur in Barrett’s esophagus that
lead to esophagus adenocarcinoma
10. The X-rays track its path
through patient digestive
system .
o Patient drink a preparation
containing this solution
11. An upper endoscopy
visually examine upper
digestive system with a tiny
camera on the end of a long,
flexible tube.
12. Esophageal manometry
Esophageal manometry is a test to measure how
well the esophagus is working.
A thin, pressure-sensitive tube is passed through
patient nose, down the esophagus, and into patient
stomach.
13. What is GERD ?
GERD states it is a condition that occurs
when the refluxed stomach contents lead
to trouble symptoms and/or complications.
GERD affects all ages espacially after 40
years.
The gender doesn't play a role in the
disease
The mortality of GERD is rare .
14. Phathophysiology
The main problem in the
development of GERD is the
abnormal reflux of gastric
contents from the stomach into
the esophagus.
15. This is due to :
1- Lower Esophageal Sphincter Pressure
2- anatomical causes
16.
17. GERD Causes
*Lower Esophageal Sphincter Pressure
Different mechanisms by which defective
LES pressure lead gastroesophageal
reflux.
18. 1- LES relaxations that are not
associated with swallowing. Although
the exact mechanism is unknown.
2- postprandially, may play an important
role in symptom-based esophageal
reflux syndromes.
3- intraabdominal pressure (stress
reflux)
19. Anatomical factor
Disruption of the normal anatomic barriers
by a hiatal hernia (when a portion of the
stomach
protrudes through the diaphragm into the
chest) was once thought to be a primary
etiology of
gastroesophageal reflux
22. Composition of Refluxate
the combination is gastric acid, pancreatic
enzymes pepsin, and/or bile is a potent
refluxate in producing esophageal
damage.
The composition, pH , volume of the
refluxate
are important aggressive factors in
determining the GERD
27. Complication
Alarm symptoms symptoms may be
indicative of complications of GERD such
as
Stricture
Barrett’s esophagus
esophageal adenocarcinoma
32. The X-rays track its path
through patient digestive
system .
o Patient drink a preparation
containing this solution
33. An upper endoscopy
visually examine upper
digestive system with a tiny
camera on the end of a long,
flexible tube.
34. Esophageal manometry
Esophageal manometry is a test to measure how
well the esophagus is working.
A thin, pressure-sensitive tube is passed through
patient nose, down the esophagus, and into patient
stomach.
35. After the tube is in the stomach, the tube is pulled
slowly back into patient esophagus.
At this time, patient is asked to swallow
The pressure of the muscle contractions is
measured along several sections of the tube.
While the tube is in place, other studies of your
esophagus may be done. The tube is removed after
the tests are completed.
36. Ambulatory–pH monitoring
test
Small tube passed through the nose into
the esophagus at the level of the LES.
A pH sensor at the tip of the tube collected
on a portable computer.
37. Treatment
1) Non-Pharmacologic treatment
Lifestyle changes
2) Pharmacologic treatment therapy with antacids,
nonprescription H2-receptor antagonists, and/or
nonprescription proton pump inhibitors Provide
symptomatic relief, and prescription strength
acid-suppression therapy .
3) Anti-reflux surgery .
38. Elevating the head end of the bed by approximately (15
to 20 cm) with a foam wedge under the mattress .
Weight loss
Avoid food that may decrease lower esophageal
sphincter like ( fat, chocolate, cola, spearmint,
alcohol(wine), pepper, Garlic, onion )
Avoid food that have the direct irritant of esophageal
mucosa like (spicy, citrus juice, tomato, coffee,
Tobacco )
Include protein rich meal in diet (augment ( increase )
lower esophageal sphincter )
Always take drugs in the setting upright .
Avoidance of tight-fitting clothes .
Lifestyle modifications
39. DosesRecommended drug
30ml need after meal, and at bedtime
15ml need after meal, and at bedtime
Maalox
Gaviscon
10mg up to twice daily /2weekFamatodine ( Pepcid Ac )
75mg up to twice daily /2weekRantidine ( Zentac )
20mg up to twice daily /2weekOmeprazole ( Prilosec )
15mg up to twice daily /2weekLanzoprazole ( Prevacid )
Pharmacologic treatment
40. The goal of antireflux surgery is to reestablish the antireflux
barrier, to position the LES within the abdomen where it
is under positive ( intraabdominal ) pressure, and to close
any associated defect in the diaphragmatic hiatus by
reinforcing the crural muscles .
Antireflux surgery should be considered for patients :
Who fail to respond to pharmacologic treatment.
Who opt for surgery despite successful treatment
because of lifestyle considerations, including age, time,
or expense of medications.
Who have complications of GERD (e.g., Barrett’s
esophagus, strictures).
Who have atypical symptoms and reflux documented
with ambulatory pH monitoring .
Anti-reflux surgery
44. Patient with
compliant of
heartburn
Life style
modification
OTC drug
Anti-acid 2 W.
H2-receptor
antagonist twice
daily
PPI one a day
4-8 W.
PPI twice daily
4-16 W.
Reduce or
Stop
medicine
Mano&
Amb.
pH
Endoscopy
Surgical
intervent
ion
Maintenance
Therapy
With minimum
eff. dose
NO
No
No
No
No
Yes
Yes
A
L
A
R
M
S
y
m
p
t
o
m
s
45. Chief Complaint
“I’m having a lot of heartburn, especially after
eating. These pills and liquids I’ve tried seem to
work for a little while, but then they wear off.”
History of Present Illness
George Anderson is a 58-year-old man
complaints of heartburn four to five times a week
over the last 4 months .
episodes of regurgitation, after which he is left with
an acidic taste in his mouth
symptoms wake him up at night approximately
once a week
46. tried Extra Strength Maalox liquid first and then
Pepcid AC tablets .
He took the Pepcid AC 10 mg twice daily for 1 week .
This worked intermittently but didn’t provide enough
relief
Past Medical History
HTN × 12 years
CKD × 2 years
Type 2 DM × 5 years
47. Social History
• He drinks one to two beers a day after work,
4–5 days per week.
• He has a 25 pack-year history of tobacco use
and currently smokes 1 ppd.
Medication history
Amlodipine 5 mg once daily
Glyburide 5 mg twice daily
Aspirin 81 mg daily
Ibuprofen 200–400 mg PRN for headaches and
pain
48. Reports occasional tension
Headaches but no visual changes, aura, or dizziness .
(–) Shortness Of Breath , cough, or hoarseness .
(+) frequent episodes of a burning pain in his
stomach area and travels up his chest associated
with an acidic taste in his mouth .
(–) N/V
(–) Bright red blood per rectum or dark/tarry stools
(–) dysuria, nocturia, or frequency;
Reports some mild ankle swelling in both ankles
He has gained approximately 8 pounds over the last 6
months
49. Physical Examination
VS : BP 149/89, P 87, RR 17, T 36°C; Wt 99 kg, Ht 5'10''
Abd : Obese;
(+) BS;
MS/Ext : No CVA tenderness;
( 1+) pitting LE edema bilaterally
Labs
Fasting Glu 200mg/dL ( high)
TC 230 mg/dL ( high)
LDL 146 mg/dL ( high)
TG 187 mg/dL ( high)
HDL 39 mg/dL ( Low )
52. SOAP Notes
GERD
★Insufficient drug therapy
S: Uncontrolled GERD symptoms (Heartburn (4-5)times in
week , regurgitation, acidic taste in his mouth) .
O: ____________
A: May be due to the patient didn’t take enough
dose & time of Pepcid AC therapy .
Usual adult dose for GERD :20mg orally /twice
daily up to 6 weeks .
Or the patient didn’t take the first line therapy of
GERD ( PPI)
53. P:
Aim /
a- Alleviate the patient symptoms
b- Decrease frequency of recurrent disease .
c- Prevent GERD complications (strictures, Barrett’s
esophagus, or possibly adenocarcinoma )
Therapy /
Non pharmacological therapy :
Pharmacological therapy :
Using PPI, the drug of choice for patient with
moderate to severe GERD
Omeprazole 20mg orally twice daily up to 4 weeks .
54. Monitoring :
Efficacy of PPI ( Omeprazole ) : according to relied
of symptoms in the patient or Ambulatory PH
monitoring .
Toxicity of Omeprazole ( Ca+2, Mg+2, Vit B12 Levels )
.
55. ★Unsafe drug therapy
S: Uncontrolled GERD symptoms
O: ____________
A: also, may result from using CCB (Amlodipine ),
which decrease lower esophageal sphincter pressure
& delay gastric emptying .
P:
Aim :
• Alleviate the patient symptoms
• Decrease frequency of recurrent disease .
• Prevent GERD complications (strictures, Barrett’s
esophagus, or possibly adenocarcinoma ) .
56. Therapy :
• Stop Amlodipine, & start to use ACEI for HTN
treatment
• ACEI : are recommended as the first line therapy of
Hypertension in patient with CKD & DM .
57. S: GERD symptoms
O: ____________
A: Maalox antiacid ( Al(OH)3 + Mg(OH)2 )
( This drug contain Al+3 which lead to toxicity in this
patient, who is suffering from CKD ) .
Toxicity due to accumulation Al+3 in patient with CKD :
Osteomalacia
Alzehimers disease
P:
Aim :
To prevent toxicity of Al+3
Therapy :
Stop Maalox
58. ★Improper Drug Selection :
S: Headache, Pain .
O: ____________
A:
Ibuprofen 200mg PRN for headache & pain
The use of NSAID drugs or aspirin is an
additional risk factor that may suitable to the
development or worsening of GERD complication
.
( NSAIDs cause direct irritation )
P:
59. Aim :
• Alleviate the patient symptoms
• Decrease frequency of recurrent disease .
• Prevent GERD complications (strictures,
Barrett’s esophagus, or possibly
adenocarcinoma ) .
Therapy :
Stop Ibuprofen and replaced with Paracetamol for
headache and pain when needed .
60. Hypertension
★ Ineffective drug therapy
S: ____________
O: B.P = 149/89mmHg
A: this drug didn’t effective to decrease SBP<
140mmHg .
P :
Aim :
• Decrease SBP < 140mmhg & DBP < 90mmHg
• To reduce renal mortality & morbidity, also decrease
CV risk .
61. Therapy :
Non pharmacology therapy :
• Maintain normal body weight ( during weight
loss ) ( BMI 18-25 )
• BMI of this patient 31.2
• Eating food rich in Fruits, Vegetables, Grains,
Low in fats & cholesterol .
• Reduce dietary Na+ :2,4 g/day Na+ (not more )
• Exercise ( Walking ) 30min/day .
• Limit alcohol drinking .
• Smoking cessation .
62. Pharmacological therapy :
• Stop Amlodipine ( unsuitable for patient state ) ,
• Use ACEI ( Enalapril 5mg/twice daily ) .
• according to American recommendation, ACEI is used
as first line treatment in Hypertension patient with
Chronic Kidney Disease ( CKD ) or with Diabetes
mellitus
• ACEI has beneficial effect on renal function, make
efferent arteriolar vasodilatation , decrease
intraglomerular pressure .
Monitoring :
Efficacy of Enalapril : B.P measurement .
Toxicity of Enalapril : CrCl, K+ level .
63. ★Unsafe drug therapy :
S: Mild ankle swelling in both ankles.
O: ____________
A: this patient’s adverse effect result from using of
Amlodipine therapy .
P:
Aim :
• The removal of this adverse effect .
• Enhance quality of life of patient .
Therapy : Stop Amlodipine therapy.( replaced
with ACEI ) .
Monitoring : Disappearance of this adverse effect
( ankle swelling ) .
64. ★Inappropriate indication for drug use
S: ____________
O: TC 230 mg/dL , LDL 146 mg/dL , TG 187 mg/dL , HDL 39
mg/dL
A: This patient has high lipid profile ( Total cholesterol, LDL,
TG, Low HDL )
Which is additional risk for CV events, and he doesn't take
Anti-hyperlipidemia therapy .
P:
Aim /
• Normal level of lipid profile ( TC=less than 200 mg/dl,
LDL=below 100 , TG=below 150 , HDL=40-60 or more
• Decrease risk for CV
65. Therapy :
• non-pharmacological :
• Weight loss
• Reduce intake of Fat & Cholesterol
• Increase intake of Omega 3
• Pharmacological
Use of statin : Atorvastatin 20 mg
66. Diabetes mellitus
★Insufficient & Improper Drug Selection :
S: ____________
O: Fasting glucose = 200 mg/dl A1C = 8,6 %
A:
Glyburide didn't decrease his blood glucose.
This patient didn't use preferred initial agent which is
has beneficial effect in this pt. (wt. gain, high risk of
CV event )
67. ★Unsafe drug therapy :
S: ____________
O: BMI = 31.2 obese
A:
Obesity in this pt. may results from use Glybruide
(it's is one of adverse effect: wt. gain),
This is risk factor which increase CV events in the
other risk factors present in this pt.
68. P:
Aim
Control blood glucose level
Prevent DM complications ( nephrophathy, neurpathy
& retiropathy )
Therapy :
NON pharmacological :
• Diet
• Weight loss
• Physical activity
69. Pharmacological :
• Stop glyburide ( not effective in decrease glucose
level, And has disadvantage : weight gain)
• Replaced it with Metformin, initiate with dose 500 mg
twice daily
No dose adjustment in this patient ( which is
suffering from CKD ) .
70. According to :
Cockreft-gault Eq. CrCl = 59.34 ml/min ( in stage 3 -
moderate- )
Dose adjustment of Metformin in renal disease if
CrCl<30 ml/min
Monitoring of Metformin :
Efficacy :
Fasting glucose test
A1C
Toxicity :
Vit B12 level ( it cause vit B12 deficiency ) .