Ante partum haemorrhage with mcq
•
14 gefällt mir•4,515 views

Video lectures on YouTube Channel name Lecture by Abhilasha verma

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Ante partum haemorrhage with mcq
Ähnlich wie Ante partum haemorrhage with mcq (20)
Mehr von Abhilasha verma
Mehr von Abhilasha verma (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Ante partum haemorrhage with mcq
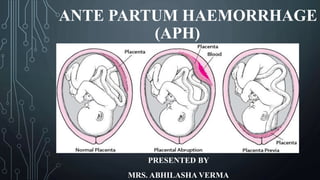
- 1. ANTE PARTUM HAEMORRHAGE (APH) PRESENTED BY MRS. ABHILASHA VERMA
- 2. DEFINITION “ It is defined as bleeding from or into genital tract after stage of viability but before birth of baby” According to WHO viability = 20 weeks, 500 gm weight, body length 25 cm. ABHILASHA VERMA 2
- 3. CAUSES AND TYPES OF APH APH Placental Bleeding(70% ) Placenta Previa (35%) Placenta Abruptia (35%) Unexplaine d (25%) Extra Placental Bleeding 5% Local cervico- vaginal Lesion Cervix Polyp Carcinoma cervix Varicose Vein Local trauma ABHILASHA VERMA 3
- 4. PLACENTA PREVIA DEFINITION “Placenta is implanted partially and completely over lower uterine segment over and adjacent to internal os is called placenta previa” or “Bleeding occur because changes which normally takes place in the lower segment before and during labour cause placental separation from it before delivery, is known as placenta previa.” ABHILASHA VERMA 4
- 5. INCIDENCE • 1 3rd cases of APH are due to placenta previa. • 1 in 200 pregnancies • 80% ( Multiparous woman) • Age > 35 years • Multiple pregnancy ABHILASHA VERMA 5
- 6. ETIOLOGY • Exact cause unknown • Poor decidual reaction of upper segment, fertilized egg Lower segment • Big surface area of placenta • Defective decidua • Others – Multi parity, previous CS, Uterus scar, smoking during pregnancy. ABHILASHA VERMA 6
- 7. CAUSE OF BLEEDING • As placental growth slow down in later months, lower segment progressively dilate, in elastic placenta shed off leads to opening up of utero-placental vessels and leads to bleeding. ABHILASHA VERMA 7
- 8. TYPES OF PLACENTA PREVIA Based on degree of placenta extension to lower segment. Type I Lateral / Low lying Type II Marginal Type III Incomplete or Partial Type IV Central ABHILASHA VERMA 8
- 9. TYPES OF PLACENTA PREVIA ABHILASHA VERMA 9
- 10. TYPE- I “LATERAL OR LOW LYING PLACENTA PREVIA” • Major part of placenta attached to the upper segment and only lower margin reaches on to lower segment but not up to OS. • Low risk of ante partum haemorrhage. ABHILASHA VERMA 10
- 11. TYPE II “ MARGINAL PLACENTA PREVIA” • Placental edges reaches to the margins of internal Os but doesn’t cover it. • Depending upon position it is of two types Type II Anterior Type II Posterior ABHILASHA VERMA 11
- 12. TYPE III “INCOMPLETE OR PARTIAL PLACENTA PREVIA” • Placenta covers internal Os when internal Os is closed but only partially covers it when it is fully dilated. ABHILASHA VERMA 12
- 13. TYPE IV “ COMPLETE OR CENTRAL PLACENTA PREVIA” • Placenta completely covers internal Os all time even after it is fully dilated. ABHILASHA VERMA 13
- 14. CLINICAL MENIFESTATIONS OR SIGN / SYMPTOMS • Anaemia and visible blood loss. • Abdominal Examination- Soft , relaxed uterus, no tenderness. Floating head Stallworthy sign ( Posterior placenta) Slow FHR on pressing head down into pelvis soon after recover promptly when pressure released. Vaginal bleeding ( Classical sign) painless, causeless, sudden onset ( usually during end of 1st trimester or during second trimester) FHR easily heared , fetal parts easily palpated. Mal-presentations are common ( Transverse/ Breech) ABHILASHA VERMA 14
- 15. DIAGNOSIS- USG confirm placental location COMPLICATION “ MATERNAL” During pregnancy During labour During puerparium APH with shock Early ROM Sepsis Malpresentation Cord prolapse Subinvolution Premature labor Slow dilation of cervix Embolism Death due to haemorrhage Intra Partum haemorrhege PPH Retained Products Trauma to cervix and lower segment FETAL COMPLICATION Low Birth weight Asphyxia IUFD Birth Injury Maternal and fetal morbidity and mortality ABHILASHA VERMA 15
- 16. MANAGEMENT OF PLACENTA PREVIA GENERAL MEASURES Prevention measures- • Adequate antenatal care to improve health and anaemia correction. • Antenatal diagnosis of low lying placenta at 20 week USG. • Warning haemorrhage should not be ignored. At Home- • Immediately put to bed. • Inspection of clothing soaked in blood. • Quick and gentle examination. ABHILASHA VERMA 16 HOSPITAL TRANSFER • Arrangement made to shift patient to equipped hospital having facilities of blood transfusion, emergency CS, NICU, etc. • Start IV RL< continue during transport. • Arrange blood donors. Admission To Hospital- Specific management done. Management depends upon- Amount of bleeding. Condition of mother and fetus. Placenta location.
- 17. Management Of Placenta Previa IMMEDIATE ATTENTION Assessment of case: Amount of blood loss. FHR auscultation. Abdominal examination to note tenderness. Inspection of vulva for active bleeding. Blood sample taken- Hb, grouping and cross matching FORMULATION OF LINE OF TREATMENT Expectant Management Definitive management Scheme of management of Placenta previa ABHILASHA VERMA 17
- 18. EXPECTANT MANAGEMENT • Johnson and Macafee protocol 1945 Indication- • GA> 37 week • Bleeding <500 ml • Patient not in labor • Mother and fetus aren’t in emergency. Measures- Complete bed rest with bathroom and toilet facilities. Inspection of vulvar pads Investigations Fetal surveillance USG every 2-3 weeks Supplementary hematinics Avoid straining at stool ( Mild laxatives) Minimal ambulation when bleeding stops. Correction of maternal blood loss. ABHILASHA VERMA 18 DEFINITIVE MANAGEMENT Indication- Bleeding at 37 weeks or more Patient in labor. Continue active bleeding( Moderate) Measures- C S delivery = Placenta edges 2 cm from internal os NVD = Placenta edges 3 cm
- 19. SCHEME OF MANAGEMENT OF PLACENTA PREVIA ABHILASHA VERMA 19
- 20. DOUBLE SET UP EXAMINATION PLACENTA PREVIA Two team approaches are used in double set up .. That is one team is ready for NVD and 2nd team ready to perform CS if necessary. Rarely performed in operating room Palpation of placental edges and fetal head with set up of immediate CS. High risk of intra operative blood loss because obstetrician may cut into placenta during uterine incision. Increased risk of placenta accreta CS delivery under regional anaesthesia if- Complete PP Fetal head not engage ABHILASHA VERMA 20
- 22. ABRUPTIO PLACENTAE DEFINITION “It is the form of ante partum hemorrhage (APH) where bleeding occurs due to premature separation of normally situated placenta.” Bleeding is almost always maternal but placenta tear may cause fetal bleeding. INCIDENCE 1 : 200 Pregnancies 15-20% perinatal mortality 2-5 % maternal mortality ABHILASHA VERMA 22
- 23. ETIOLOGY Exact cause is unknown in most cases. High birth order pregnancies. Advancing maternal age. Poor socio-economic condition. Malnutrition and cigarette smoking ( Vaso spasm) Short cord (Mechanical Pulling) Trauma: Needle injury Accident Ex. Cephalic version. Continue………………. ABHILASHA VERMA 23
- 24. Sudden uterine compression PROM and delivery of 1st twin baby. Supine hypotension syndrome – Passive engorgement of uterine and placental blood vessels result in rupture and extravasation of blood. Poor placentation. Folic acid deficiency. Abnormal implantation and septum Torsion of uterus. Placental anomalies. ( Circumvallate placenta) ABHILASHA VERMA 24
- 26. REVEALED ABRUPTIO PLACENTA • Most common type. • Following placental separation blood released and effused sooner or later escapes under placental margins and make its own way between membrane and uterine wall down to internal os of cervix, where pass through vagina. CONCEALED ABRUPTION PLACENTA • Blood collects behind separated placenta and/or collects in between membrane and decidua. • Collected blood is prevented from coming out of cervix by presenting part. • Blood isn’t visible outside ( Rare case) ABHILASHA VERMA 26 MIXED ABRUPTIO PLACENTA It is quite uncommon, some part of blood collected inside ( Concealed) and some part of blood is expelled out ( Revealed). There may be one variety dominate over another.
- 28. CONCEALED & REVEALED ABRUPTIO PLACENTA ABHILASHA VERMA 28
- 29. CLINICAL FEATURES OF AP Parameters Revealed Concealed ( mixed) Symptoms Abdominal discomfort, pain followed by slight vaginal bleeding Acute intense abdominal pain followed by vaginal bleeding, continue pain Character of bleeding Dark color bleeding Dark color bleeding, blood stained serous drainage General condition Propionate to visible blood loss, shock usually absent Shock, out of proportionate to visible blood loss. Pallor Related with visible blood loss Severe, out of proportionate severe pallor Features of pre-eclampsia Absent Frequently present Uterine height Acc. To GA Enlarged and more globular then GA Fetal parts Easily identified Difficult to find FHS Usually present Usually absent ABHILASHA VERMA 29
- 30. INVESTIGATIONS ABHILASHA VERMA 30 Parameters Revealed Concealed Blood Hb% Low values proportionate to visible blood loss Lower values out of proportionate to visible blood loss Coagulation profile Usually unchanged Clotting time increase Low platelet count Low fibrinogen count Urine protein Absent Present
- 31. DIFFERENTIAL DIAGNOSIS Revealed type confused with placenta previa. Concealed or mixed type confused with- • Ruptured uterus • Rectus sheath hematoma • Intestinal or appendicular perforation • Twisted ovarian tumor • Volvulus • Tonic uterine contraction ABHILASHA VERMA 31
- 32. CLINICAL GRADING OR DEGREE OF ABRUPTIO PLACENTA 1) Grade – 0 • Absent c/m • Diagnosis made after inspection of placenta following delivery. 2) Grade – 1 (40%) • Slight vaginal bleeding • Irritable, tender uterus may be minimum or absent • FHS good • Maternal BP and fibrinogen unaffected 3) Grade- 2 (45%) • Mild to moderate vaginal bleeding • Uterine tenderness always • Increase maternal Bp and pulse • Decrease fibrinogen level • Absent shock • Fetal distress and shock ABHILASHA VERMA 32 Grade –3 (15%) Bleeding moderate to severe Marked uterine tenderness Shock present Fetal death is rule Coagulation defect Anemia present
- 33. MANAGEMENT OF PLACENTA ABRUPTION USG guided safe needle puncture aminocentes is Early detection Avoid trauma Folic acid administration Avoid supine hypotensio n syndrome Avoid sudden decompression of uterus ABHILASHA VERMA 33 PREVENTIVE MEASURE
- 34. TREATMENT ABHILASHA VERMA 34 Assessment of case - • Amount of blood loss • Maturity of fetus • Type and degree of separation. • Labor status Emergency measures – • Blood sent for Hb, hematocrit estimation, coagulation profile, ABO , Rh, urine protein estimation. • Blood donors arrange. Definitive treatment (Immediate delivery) Patient in labor- • Accelerate labor by low rupture of membrane • Oxytocin drip • Vaginal delivery Patient not in labor- • Induction of labor • CS
- 35. SCHEME OF MANAGEMENT OF ABRUPTIO PLACENTA ABHILASHA VERMA 35
- 36. PREVIOUS YEARS QUESTIONS ABHILASHA VERMA 36
- 37. 1. Placenta previa and Abruptia are examples of: a) APH RIMS & R SAIFAI UP 2013 b) PPH c) Eclampsia d) Vesicular mole Answer (a) 2. A woman is 37 weeks pregnant and she is bleeding profusely with no pain is suggestive of: Safdarjung Hos. Delhi Nursing Officer 2018 a) Ante partum hemorrhage b) Unavoidable hemorrhage c) Accidental hemorrhage d) Concealed hemorrhage Answer (a) ABHILASHA VERMA 37
- 38. 3. Ante partum hemorrhage (APH) is associated with all of the following except: a) Post partum hemorrhage (PGI Rohtak Staff Nurse 2017) b) Anemia c) Increased perinatal mortality d) Post term pregnancy Answer (d) 4. Vaginal bleeding after 28th weeks of pregnancy which is sudden onset, painless, causeless and recurrent is known as: a) Abortion (RUHS M.Sc. Nursing Entrance 2018) b) Abruptio Placentae c) Placenta previa d) Vasa previa Answer (c) ABHILASHA VERMA 38
- 39. 5. What is the color of blood in placenta previa? a) Bright red UPPSC, UP STAFF NURSE NURSE 2017 b) Brick red c) Brown Red d) None Of these Answer (a) 6. A client arrives at the hospital at 38 weeks gestation with profuse vaginal bleeding. She states that it occurred suddenly without any contractions. Which condition may the client be experiencing that require immediate notification of the health care provider? a) Placenta previa BHU NURSING OFFICER SEP. 2019 b) Concealed abruption c) Placenta accrete d) Ruptured uterus Answer (a) ABHILASHA VERMA 39
- 40. 7. Sign and symptoms of the placenta previa include: a) Sharpe abdominal pain RUHS M.Sc.Nursing entrance 2014 b) Early rupture of membrane Jhalawar Med. College Staff Nurse 2010 c) Increased low back pain d) Painless vaginal bleeding Answer (d) 8. Placenta Previa is characterized by all of following EXCEPT: a) Painless bleeding RUHS M.Sc. Nursing Exam 2017 b) Present in 1st trimester c) Causeless bleeding d) Recurrent bleeding Answer (b) ABHILASHA VERMA 40
- 41. 9. Following risk is associated with placenta previa: a) Disseminated Intra vascular coagulation ( DIC) IGNOU Post B.sc Nursing 2012 b) Chronic hypertension RUHS Post B.Sc. Nursing Entrance 2017 c) APH d) Infection Answer (c) 10. Possibility of common complications after delivery into a mother suffering with placenta previa: a) Infertility ESIC Staff Nurse Bhiwari 2019 b) Uterine atonicity c) Hemorrhage d) Amenorrhoea Answer (c) ABHILASHA VERMA 41
- 42. 11. Maternal complication during labor labor in placenta previa: a) Early ROM RAK M.Sc. Nursing Entrance 2014 b) Asphyxia c) Low birth weight babies d) Birth injuries Answer (a) 12. An occurrence in which umbilical cord vessels pass through placental membranes and lie across the cervical os is termed as: a) Abruptio placenta AIIMS Raipur Staff Nurse Aug 2019 b) Placenta previa c) Placenta accrete d) Vasa previa Answer (d) ABHILASHA VERMA 42
- 43. 13. Management during minor placenta previa: a) Blood transfusion AIIMS BHOPAL Nursing Officer May 2018 b) Complete rest c) Caesarean section d) Drug therapy Answer (b) 14. Mother is diagnosed with partial placenta previa. The nurse tells the client that the usual treatment for partial placenta previa is- a) Bed rest BCCL Staff Nurse 2015 b) Administration of platelets c) Immediate caesarean section d) Induction of labor with oxytocin Answer (a) ABHILASHA VERMA 43
- 44. 15. Definitive treatment of placenta previa are: a) Bed rest RAK M.Sc. Nursing entrance 2018 b) Supplementary hematinic c) Use tocolytic d) Caesarean section Answer (d) 16.A multigravida 32 years old lady, admitted at 10 weeks with bleeding per vagina, which of the action the nurse should first to do first: a) Perform a per vaginal examination ESIC Staff Nurse Delhi 2012 b) Provide perineal pads c) Take consent for Caesarean section d) Check FHR and BP Answer (b) ABHILASHA VERMA 44
- 45. 17. A client with painless vaginal bleeding has just been diagnosed as having placenta previa. Which of following procedure usually performed to diagnose placenta previa: a) Aminocentesis ESIC Staff Nurse Kolkata & Banglore 2012 b) Digital or speculum examination c) External fetal monitoring d) Ultrasound Answer (d) 18. In caring for a client diagnosed with placenta previa, the nurse should avoid which of the following: a) Inspecting the perineum BPS GOVT. MED. COLL. KHANPUR, HARYANA b) Performing ultrasound c) Performing a pelvic examination d) All of above Answer (c) ABHILASHA VERMA 45
- 46. 19. The nurse gently performs leopold’s maneuvers on a client with a suspected placenta previa and expects to find the: a) Fetal head firmly engaged RAK M.Sc Nursing Entrance 2009 b) Fetal presenting part high and floating c) Fetal small parts difficult to palpate d) Uterus hard and tetanically contracted Answer (b) 20.If a vaginal examination is to be performed on a client with possible placenta previa, the nurse must be prepared for immediate: a) Forceps delivery RAK M.Sc. Nursing entrance 2010 b) Induction of labor c) Caesarean section d) X ray examination Answer (c) ABHILASHA VERMA 46
- 47. 21. When the placenta covers the internal os partially when closed but does not entirely do so when dilated ia known as: a) Marginal placenta previa RAK M.Sc.Nursing entrance 2016 b) Low-lying placenta previa c) Central placenta previa d) Incomplete placenta previa Answer (d) 22. Which of following considered as dangerous placenta previa- a) Type I Posterior SSB DD & DNH Nursing officer Feb 2018 b) Type II Anterior RUHS M.Sc. Nursing Entrance 2018 c) Type II Posterior RAK M.Sc. Nursing Entrance 2014 d) Type I Anterior Answer (c) ABHILASHA VERMA 47
- 48. 23. Abruptio placenta means premature separation of- a) Normally situated placenta NPCIL Staff Nurse June 2019 b) Abnormal placenta c) Abnormally situated placenta d) Fetal membrane Answer (a) 24 Accidental hemorrhage is also known as: a) Vasa previa NVS (Navodaya) Staff Nurse Sep. 2019 b) Placenta previa c) Abruptio placentae d) Circumvallete placenta Answer (c) ABHILASHA VERMA 48
- 49. 25. The condition “Abruptio placentae’ refers to- a) Abortion NVS Staff Nurse Jan 2018 b) Ante partum hemorrhage c) PPH d) Low lying placenta Answer (b) 26. Incidence of abruptio placentae occur in: a) Third trimester GMCH Mewat Haryana 2014 b) Second trimester c) First trimester d) None of these Answer (a) ABHILASHA VERMA 49
- 50. 27. Premature separation of normally implanted placenta during the second half of pregnancy, usually with severe hemorrhage is known as: a) Placenta previa DSSSB Staff Nurse 2013 b) Ectopic pregnancy BSF Staff Nurse 2014 SI c) Incompetent cervix d) Abruption placentae Answer (d) 28. The most common pathological cause of late pregnancy bleeding: a) Placenta previa IGNOU Post B.Sc. Nursing 2016 b) Gestational hypertension c) Fetal distress d) Abruptio placentae Answer (d) ABHILASHA VERMA 50
- 51. 29. Couvelaire uterus condition associated with- a) Post term placenta RAK M.Sc. Nursing Entrance 2014 b) Revealed abruptio placenta c) Concealed abruptio placenta d) Placenta previa Answer (c) 30. Couvelaire uterus is seen in- a) Placenta previa PGI Rohtak Staff Nurse 2015 b) PIH c) Accedental hemorrhage d) PPH Answer (c) ABHILASHA VERMA 51
- 52. It is pathological entity in association of severe form of concealed abruptio placentae. There is massive intravasation of blood into uterine musculature up to serous coat. ( Only laparotomy can diagnose this condition) 52
- 53. 31. Following are the causes of separation of a normally situated placenta, EXCEPT: a) Sudden uterine decompressionAIIMS Raipur Staff nurse 2017 b) Defective decidua c) Supine hypotension syndrome d) Thrombophlebitis Answer (b) 32.Which of following is termed as fetal blood vessels lying over the internal os, in front of presenting part- a) Vasa previa RRB Staff Nurse 2019 b) Cord presentation RUHS M.Sc. Nursing Entrance 2019 c) Cord prolapse d) Occult cord prolapse Answer (a) ABHILASHA VERMA 53
- 54. 33. Among following, event during pregnancy that require immediate attention by the physician: a) Back ache AIIMS Bhopal Nursing Nursing Officer May 2018 b) Bleeding per vvagina c) Dependent edema d) Frequency of micturition Answer (b) ABHILASHA VERMA 54
- 55. THANK YOU ABHILASHA VERMA 55