
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie MEASLES - soon to be eradicated ..!!
Ähnlich wie MEASLES - soon to be eradicated ..!! (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
MEASLES - soon to be eradicated ..!!
- 3. Synopsis -Introduction -Causative agent -Epidemiological factors Measlesin INDIA -Complications -Prevention Problemstatement -Outbreakcontrol measures -Eradicationof measles -Summary
- 4. INTRODUCTION Measles (RUBEOLA) is an acute highlyinfectious disease of childhood. Generally the symptoms are fever, catarrhal symptoms of respiratory tract such as cough, coryza followed by a typical rash. Measles is associated with high morbidity and mortalityin developing countries. Measle occur only in HUMANS. There is no animal reservoir of infection.
- 5. MEASLES
- 6. CAUSATIVE AGENT Measles is generally causedby a specific virus of the group MYXOVIRUSES. It is an RNA PARAMYXOVIRUS. This virus cannot survive outside the human body for any length of time , but retains infectivity when stored at sub- zero temperature. This virus has been grown in cell cultures.
- 7. EPIDEMIOLOGICAL DETERMINANTS AGENT FACTORS AGENT– RNA PARAMYXOVIRUS SOURCEOF INFECTION–the only source of infectionis A CASE OF MEASLES. INFECTIVEMATERIAL– Secretions of the nose,throat, respiratory tract of a case of measles during prodromal stageand earlystageof rash COMMUNICABILITY–highly infectious, but it declines after the appearance of rash. PERIOD= 4 days before and 4 days afterthe appearance of rash. PREVENTION- isolationof the patient. SECONDARYATTACKRATE – infection confers life long immunity, rare.
- 8. HOST FACTORS AGE– Affects virtually everyone in infancy or childhood. Between 6 months and 3 years of age in developingcountries, and above 5 years in developed countries. SEX- incidence equal IMMUNITY- No age is immune. One attackconfers life long immunity. Infants are protected by maternal antibodies upto6 months of age. NUTRITION– severe in malnourished child, possibly relatedto cell mediatedimmunity.
- 9. ENVIRONMENTAL FACTORS Paramyxovirus can spread in any season. Tropical zones = most cases occur during dry season Temperate zones= duringwinterseason Epidemics of measlesare common in INDIAduringwinter and early spring (JANUARYTO APRIL) TRANSMISSION Directly fromperson to person = droplet infection The portal of entry is RESPIRATORYTRACT.
- 10. INCUBATION PERIOD Incubation period is commonly 10 days fromexposure to onset of fever 14 days to appearance of rash When measles infection is artificially induces, incubation period is shortened to around 7 days. CLINICAL FEATURES 1) PRODROMALSTAGE 2) ERUPTIVEPHASE 3) POST–MEASLESSTAGE
- 11. PRODROMALSTAGE Begins 10 days after the infection and lasts until day 14 Characterized by fever, coryza with sneezing and nasal discharge ,cough, redness of eyes, lacrimation and often photophobia Before the appearance of rashes, KOPLIK’SSPOT like table salt crystals appear on the buccal mucosaopposite the first and second molars KOPLIK’SSPOTS– They are small , bluish white spotson a red base, usually smaller than the head of a pin. Their presence is PATHOGNOMONICto measles.
- 13. KOPLIK’S SPOTS
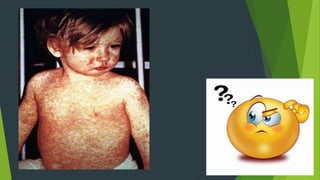
- 14. ERUPTIVE PHASE Characterized by a typical ,dusky-redmacular or maculo-popular rash. Begins behind the earsand spreads rapidly in a few hours over the face and neck and extends down the body . It takes 2-3 days to progress to lower extremities The rash fades in the same order of appearance leaving a brownish discoloration whichmay persist for 2 months or more.
- 15. RASHES DEVELOPED DURING ERUPTIVE PHASE
- 16. POST MEASLES STAGE The childwill have lost weight and will remain weak for a number of days. Failure to recover Gradual deterioration into chronic illness due to increased susceptibility to other bacterial and viral infections Maybe growthretardation , diarrhea , pyogenic infections, reactivation of pulmonary tuberculosis
- 17. MEASLES – IN INDIA In INDIA, MEASLES – a majorcontributor to childhoodmortality Prior to immunization program, cyclical increase in the incidence of measles were recoreded every THIRDYEAR . Several outbreaks are recordedin tribal and remote areas. 1987- 2.47 lakh cases were reprted , wheras after implementation of UIP, reduced to 23,348 cases with 33 deaths in 2014. But in INDIAthe estimates are much higher because a large numberof cases go unreported. WHO – Measles – 2%of under 5 deathin INDIA
- 18. MEASLES IN INDIA
- 19. MEASLES IN INDIA
- 20. DIAGNOSIS Diagnosis of measles is basedon the TYPICAL RASHand KOPLIK’S SPOT seen in oral mucosa. The diagnosis would normally be incorrect in any febrile exanthemin which red eyes andcough are absent In developedcountries, where measles is uncommon , specificIgMantibodies are usedfor diagnosis.
- 21. COMPLICATONS Measles is oftenregarded as an unimportant infection, But this is not true. The mostcommoncomplications are 1)Measles– associateddiarrhea 2)Pneumonia, Respiratorycomplications 3)OTITISMEDIA( it is a groupof inflammatorydiseases of the middle ear) Out of all these , Pneumonia is the most common life threatening complication It occurs less than10% in developed countries and 20- 80 % cases in developing countries.
- 22. COMPLICATIONS NEUROLOGICAL COMPLICATIONS 1) febrile convulsions 2) encephalitis 3) sub – acute PAN- encephalitis PREGNANCY Not known to cause congenital abnormalities to the foetus. Spontaneous abortion and Premature babies. Vitamin A 50,000 IU for < 6 months 100,000 IU for < 6-11 month 200,000 IU for children > 12 months
- 23. MEASLES AND CHICKENPOX Sometimes measles and chickenpox occur together First infection may diminish the severity of the second infection
- 24. PREVENTION OF MEASLES Measles Vaccination Immunogobulins MEASLES VACCINATION A) Vaccine– Only liveattenuated vaccines are used Presentedas a freeze driedproduct Eachdose = 0.5 ml contains > 1000 viral infective units of the vaccine strain Also containsorbitol , hydrolysedgelatin, a small amount of neomycin Reconstitutedvaccine loses 50% potency= 1 hour at 20 degree Celsius All potency = at 37 degree Celsius Also sensitive to sunlight , storedin darkin coloured glass vials.
- 25. AGE– WHOexpandedprogramon immunization recommends immunization at 9 months of age. This has been adoptedin INDIA Developed countries = at 12 months of age ADMINISTRATION– reconstituted vaccine , generally administered subcutaneously, also intramuscularly REACTIONS– Wheninjected intothe body, the virus multiplies and induces a mild measles illness( fever and rash ) , 5-10 days after immunization Fever 1-2 days / Rash – 1-3 days No spreadof vaccines fromvaccines to contacts IMMUNTY– This vaccine has convincingly demonstrated to provide immunity to evenmalnourishedchildren Immunity develops 11-12days after vaccination
- 26. CONTACTS– susceptible contacts 9-12months protectedwithMV but within3 days of exposures Because incubation period by vaccines = 7 days, but incubation period of naturallyacquired measles =10 days CONTRAINDICATIONS– combinedvaccines should be avoidedby patients with highfever, pregnantwoman Earlystage of HIV not a contradindication SADVERSE EFFECTSOF VACCINE– toxic shocksyndrome TSS . MEASLESAND HIV routinelyadministeredto suspectible but asymptomaticHIV positive childrenand adults Areas withhigh incidence of HIV- vaccinationat 6 age months
- 27. COMBINED VACCINE Combinedwith other live attenuatedvaccines MMR VACCINE = measles, mumps , rubella MMRVVACCINE = measles, mumps, rubella andvaricella MR = measles andrubella
- 28. IMMUNOGLOBULINS Prevented by immunoglobulins ( human ) early in the incubation period Dose – 0.25 ml/kg of body weight. Should be given within 3-4 days of exposure
- 29. PROBLEM STATEMENT Measles is endemic virtually in all parts of the world. Epidemics- proportion of susceptible children reaches about 40%. When the disease is introduced into a virgin community, more than 90% of the communitywill be affected. Measles is nowrare in industrialized countries, but still a common illness in many developing countries. Primary reason- failureto deliverat leastonedoseof measlesvaccineto all infants.
- 30. CHALLENGES The challenges for elimination of Measles include High infectious nature of measles Populations that are inaccessible due to conflict Weak immunization systems The increasing refusal of immunization by some populations The changing epidemiology of measles whichhas led to increased transmission among adolescents and adults.
- 31. WHO STRATEGY FOR ELIMINATION OF MEASLES In 1980, before widespreaduse of measles vaccine , an estimated2.6 million measles deathoccur worldwide. Recognizing this threat, WHOand UNICEF developed an accelerated measles mortalityreductionstrategyof delivering 2 dosesof MEASLESCONTAINING VACCINE[ MCV] to all children throughroutine services and supplementary immunizing activities [ SIAS] Implementation -2001 Estimated measles deathhas fallenfrom 7,33,000 in year 2000 to 1,14,900 in year 2014. During the period2000 to 2014 ,measles vaccinationprevented 17.1 millioncases.
- 32. UPCOMING STRATEGY WHO& UNICEF- GLOBALMEASLESANDRUBELLA STRATEGICPLAN( 2012-2020) AIMS: 1) Achieve andmaintain highlevels of population immunity- 2 doses of MCR vaccines 2) Establish effective survilance to monitor disease and evaluate progress.
- 33. OUTBREAK CONTROL MEASURES The following control measures have been recommended Isolation of the patient for 7 days after onset of the rash Immunization of contacts within 2 days of exposure PROMPT IMMUNIZATION at the beginning of the onset is essential to limit the spread
- 34. ERADICATION OF MEASLES Like small pox, MEASLES is amenable to eradication Favourable fact = Only 2 dose of vaccine is enough New vaccines- heat stable Immunization coverage of atleast 96%of children under 1 year of age
- 36. SUMMARY Measles also known as rubeola is an acute highly infectious disease Causedby an RNA paramyxovirus Symptoms – coryza, cough, Koplik’s spot, typical rash Clinical features- Prodromal stage, eruptive phase, post-measles phase Transmission – only a case of measles More commonin developing countries, less commonin developedcountries Prevention– vaccination, immunoglobulins 1 dose of vaccine – 99%of protection Combined vaccines – MMR , MMRV, MR Like chickenpox measles is amenable to eradication
- 37. PREVENTION IS BETTER THAN CURE