
Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie CyberKnife SRS System Explained
Ähnlich wie CyberKnife SRS System Explained (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
CyberKnife SRS System Explained
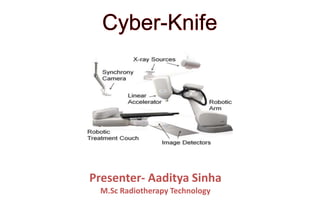
- 1. Presenter- Aaditya Sinha M.Sc Radiotherapy Technology
- 2. What is a CyberKnife? A frameless robotic radiosurgery system used for treating benign as well as malignant tumors and other medical conditions: • The CyberKnife concept, invented by Dr. John Adler, a neurosurgeon in Stanford, USA, came into practice by1990s. • Presently, Accuray Inc., Sunnyvale, CA, USA is the firm manufacturing the Cyberknife system
- 3. Stereotactic Radiosurgery/Radiotherapy (SRS/SRT) • Stereotactic means using a precise 3-D mapping technique to guide a procedure. • Radiosurgery refers to stereotactically guided conformal irradiation of a defined target volume in a single session. • SRT is delivered in multiple fractions. • Now-a-days SBRT i.e. Stereotactic Body Radiotherapy is increasingly being used.
- 4. Key requirements for optimal SRS/SRT/SBRT Requirement Rationale • Small target reducing the volume improves tolerance • Sharply defined target no inclusion of normal tissues • Accurate dose delivery no margin and hence smaller volume • High conformity reduced treatment volume • Sharp dose fall-off better sensitive organs/normal tissues sparing
- 5. GTV CTV PTV Target Volumes • GTV - Gross Target Volume includes tumor that can be seen in treatment planning images (typically CT, MR or PET). • CTV - Clinical Target Volume includes the GTV plus regional lymph nodes and tissue adjacent to the GTV that may contain microscopic tumor cells. • PTV - Planning Target Volume includes CTV plus a margin of healthy tissue to account for inter- and intrafraction organ motion. In order to treat the CTV, the planner must design a treatment plan for the PTV. ICRU50 ICRU62
- 6. Problem areas in accurate targeting • Inter-fraction and intra-fraction tumour movement/shift : i) Caused by respiratory, skeletal muscular, cardiac and gastrointestinal systems : intra-fraction ii) Set-up errors : inter-fraction
- 7. On-board imaging • Generally on-board imaging namely portal imaging, CBCT etc correct for inter-fraction errors such as patient set-up errors and organ filling errors.
- 8. Management of Respiratory Motion • Respiratory gated techniques. • Breath-hold techniques. • Forced shallow breathing methods. • Real-time tumor tracking methods. • Adding margin around CTV
- 9. Note of Caution • Respiratory motion is just one potential source of error in radiotherapy. Other important errors, particularly for lung tumors, are gross tumor volume (GTV) and clinical target volume (CTV) definition variations and set-up errors. • Some of these errors are almost an order of magnitude larger than that of respiration-induced motion. Also, set- up errors for lung and breast cancer are of the same or a higher order than that of respiratory motion.
- 10. • It uses the proprietary tracking technology for motion management correcting for intra-fraction motion. • It is the only technology where the beam tracks the tumor except for MLC based tracking.
- 11. Various Components of CK (X-band)
- 12. Various Components… • 6 MV Compact X-band linac • Robot with 6 degrees of freedom • 12 interchangeable circular collimator • 5-60 mm dia at SSD 80 cm • SSD can vary from 65-100 cm • Orthogonal X-ray system • Synchrony External tracking system
- 14. MLC With the new InCise Multileaf Collimator, the CyberKnife M6 Series is the only clinical solution to combine the benefits of the Multileaf Collimator (MLC) beam shaping with continual image guidance and non- isocentric, non-coplanar treatment delivery.
- 15. 6D Robotic Couch
- 16. Robotic Couch • With a full six degrees of freedom, the RoboCouch System can automatically control anterior/ posterior, superior/ inferior, left/right, pitch, roll and yaw corrections—for the sub-millimeter demands of full body radiosurgery and high-precision radiation therapy. • It provides access to targets in any part of the body. • 500 lb. weight capacity.(227 Kg)
- 17. Synchrony Tracking System Principles: The goal of Synchrony is to track the tumor motion in real-time so that the CyberKnife robot can adjust the radiation beam continuously throughout the treatment to ensure that the beam motion follows the motion of the tumor. Currently, Synchrony is the only system in wide clinical use that can track tumor motion in 3 dimensions using real-time feedback from the patient, which does not use continuous fluoroscopy throughout the treatment.
- 18. Synchrony Respiratory Tracking System • Patient wears a vest with optical markers that serve as a surrogate for tumor position. • Camera system monitors position of markers.
- 19. Synchrony Respiratory Tracking System • Before the treatment, a correspondence model between the markers and the tumor position is constructed using the camera and multiple orthogonal X-ray. • Model is updated continuously during treatment by further x-ray imaging. • During delivery, the tumor position is tracked using the live camera signal and the correspondence model. • The robotic is moved in real-time to maintain alignment with the tumor.
- 20. Plan Prescription • The prescription isodose for CK is typically 80% isodose line. • A plan is considered ideal if 80% of the tumor volume is covered by the prescription dose. In some cases, it may be very difficult to achieve this goal due to the proximity of critical organs and the larger penumbra of the larger cones.
- 21. Planning Process • If tumor tracking is to be done with fiducials, 2-4 gold markers (0.8 mm dia, 5 mm long) are inserted into or close to the tumor with CT/USG guidance one week prior to actual planning. • Breath-hold ( end inspiration/expiration) CT scan is taken for contouring ,marker identification and DRR generation. • A 4D CT is done to assess the fiducial motion. If its more than 2mm in any direction, only then Synchrony is used.
- 22. Tumour Tracking Modeling • If a fiducial marker is implanted within a tumour or close to it, their relative motion would be linear and hence modeling more accurate. Here the tumour and the markers follow the same trajectory. • One marker in the tumour is enough for tracking. However, at least two need to be implanted to know of marker slippage.
- 23. • At the beginning of treatment, a mathematical model (correspondence between external markers as seen by the camera and the internal fiducial markers seen by the x-rays) is built, which is then used to determine the tumor position in real time. • Two orthogonal diagnostic images are taken at least 8 times at different phases of the respiratory cycle. • By registering these images with 2 DRRs which are generated from the planning CT, the absolute position of the tumor relative to the fiducials can be determined.
- 24. • To build a reliable model, it is best to image once at the end of inspiration, once at the end of expiration, 3 times at different phases of inspiration and an additional 3 times at different phases of expiration—a total of 8 images. • Each time a pair of orthogonal images is taken synchronously, they are digitized, positions of internal fiducial markers are registered, and each image is time- stamped.
- 25. CyberKnife Delivery • Radiation is delivered at a discrete set of linac positions called nodes. • A typical treatment plan will use 110 nodes distributed approximately uniformly over about one half of a sphere centered on the treatment site.
- 26. • The treatment, which generally lasts 30 - 90 minutes, typically involves the administration of 100 - 200 radiation beams ( from the possible 1200 directions) delivered from different directions, each lasting from 10 to 15 seconds. The patient may leave the facility immediately upon completion of the procedure.
- 27. Applications • SRS, SRT and SBRT for various sites • Cranial benign/malignant tumours • Lung, prostate tumours • Cranial /extracranial mets
- 28. Advantage of Cyberknife: • Frameless • Fractionated delivery • Can be used for both intracranial and extracranial stereotactic delivery. Disadvantages: • The use of a pencil beam based delivery is inefficient and can lead to treatment times that can be several hours.
- 29. Thank You
Hinweis der Redaktion
- 5