Dr Treacy's Removal of Bio-Alcamid Filler from Lip
•
1 gefällt mir•1,129 views

A 20-year-old woman presented with nodular swellings in her lips that had been present for over two years after injection with the filler Bio-Alcamid. Previous treatments with steroids provided no relief from the worsening swellings. Surgical excision of the nodules was performed, and biopsies showed no foreign body giant cells or crystalline structures. Various treatments are discussed for filler complications including steroids, 5-FU, anti-inflammatories, and surgical excision when conservative therapies fail. Bio-Alcamid has been removed from the market in many countries due to significant reported adverse reactions.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie Dr Treacy's Removal of Bio-Alcamid Filler from Lip
Ähnlich wie Dr Treacy's Removal of Bio-Alcamid Filler from Lip (20)
Mehr von Dr. Patrick J. Treacy
Mehr von Dr. Patrick J. Treacy (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Dr Treacy's Removal of Bio-Alcamid Filler from Lip
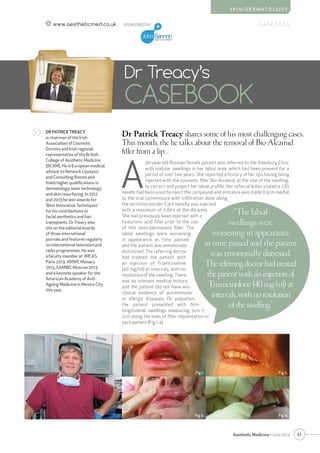
- 1. 61 CASE FILES Aesthetic Medicine • June 2014 S K I N / D E R M AT O L O G Y www.aestheticmed.co.uk Dr Patrick Treacy shares some of his most challenging cases. This month, the he talks about the removal of Bio-Alcamid filler from a lip… Dr Treacy’s CASEBOOK DR PATRICK TREACY is chairman of the Irish Association of Cosmetic Doctors and Irish regional representative of the British College of Aesthetic Medicine (BCAM). He is European medical advisor to Network Lipolysis and Consulting Rooms and holds higher qualifications in dermatology, laser technology and skin resurfacing. In 2012 and 2013 he won awards for ‘Best Innovative Techniques’ for his contributions to facial aesthetics and hair transplants. Dr Treacy also sits on the editorial boards of three international journals and features regularly on international television and radio programmes. He was a faculty member at IMCAS Paris 2013, AMWC Monaco 2013, EAMWC Moscow 2013 and a keynote speaker for the American Academy of Anti- Ageing Medicine in Mexico City this year. >> SPONSORED BY A 20-year-old Russian female patient was referred to the Ailesbury Clinic with nodular swellings in her labial area, which had been present for a period of over two years. She reported a history of her lips having being injected with the cosmetic filler Bio-Alcamid, at the site of the swelling, to correct and project her labial profile. Her referral letter stated a 23G needle had been used to inject the compound and entrance was made 0.5cm medial to the oral commissure with infiltration done along the vermilion border. Each hemilip was injected with a maximum of 0.6ml of Bio-Alcamid. She had previously been injected with a hyaluronic acid filler prior to the use of this semi-permanent filler. The labial swellings were worsening in appearance as time passed and the patient was emotionally distressed. The referring doctor had treated the patient with an injection of Triamcinolone (40 mg/ml) at intervals, with no resolution of the swelling. There was no relevant medical history and the patient did not have any clinical evidence of autoimmune or allergic diseases. On palpation, the patient presented with firm longitudinal swellings measuring 3cm × 2cm along the lines of filler implantation in each patient (Fig 1-4). “The labial swellings were worsening in appearance as time passed and the patient was emotionally distressed. Thereferringdoctorhadtreated thepatientwithaninjectionof Triamcinolone(40mg/ml)at intervals,withnoresolution oftheswelling.” Fig 1. Fig 3. Fig 4. Fig 2.
- 2. 62 Aesthetic Medicine • June 2014 S K I N / D E R M AT O L O G Y CASE FILES SPONSORED BY The nodules were prominent anteriorly and projected from inside the oral cavity. The patient was willing to accept surgical correction and histopathological evaluation of her underlying problem. Surgical excisions were carried outbydirectuseofasize11scalpel blade, without the use of local anaesthesia, by allowing the nodules to point under digital manipulation. The wound was thoroughly cleaned and the vermillion tissues were approximated in some cases with 5-0 Vicryl Rapide sutures (Ethicon, Inc) to achieve haemostatis. (Fig 5-6) The operation sites healed well and most had healed within a few days. The excision biopsies showed no evidence of foreign body giant cells or irregular crystalline structures. DISCUSSION The search for the ideal filling material has been ongoing for centuries. The ease of use, effectiveness and low morbidity of hyaluronic acid types have made them popular among patients1 . Various other materials, including collagens, autologous fat, hyaluronic acids and injectable liquid injectable silicone have also been used for this indication.2 Bio-Alcamid(Polymekon,Brindisi,Italy)isanon-reabsorbable polymeric material composed of 96% of apyrogenic water and 4% of an alkylimide-amide group. Unlike other materials, Bio-Alcamid can sometimes be removed even after long time after implantation.3 The gel is colorless and trans-parent. It is supplied in packs containing two sterile 1ml syringes for the lips (Bio-Alcamid LIPS) and one 3ml syringe for the face (Bio-Alcamid FACE).4 Some studies consider Bio-Alcamid to be almost an ideal injectable substance for the treatment of facial aesthetic defects.5 It also used medically to treat soft tissue deficits such as pectus excavatum, gluteal atrophy, acne scars as well as HIV facial lipoatrophy and Poland syndrome.6 Since its initial use, numerous reports of adverse reactions havebeenreportedincludingsignificantinfectionsandmigration resulting in significant facial deformity.7 Because of this, Bio- Alcamid has been taken off the market in many countries and the original manufacture has since stopped production.8 CONCLUSION Treatment options for filler complications include intralesional steroids, 5-fluorouracil (5-FU), anti- inflammatory and immunomodulatory drugs like minocycline, rifampicin or hydroxychloroquine. Anecdotal reports also suggest some relief with the use of non-steroidal anti-inflammatory drugs (NSAIDs), antihistamines and tacrolimus. In case of widespread lesions or repeated failure of conservative therapies, surgical excision is the treatment of choice. Surgical extirpation can also allow a dermatologist to prevent the cutaneous side effects of intradermal steroid or 5-FU injection and a histopathological confirmation can be done to rule out the possibility of a granuloma. AM REFERENCES 1. GlavasI.P.:Fillingagents.OphthalmolClin.NorthAm.8:249- 257,2005. 2. NarinsR.S.andBeerK.:Liquidinjectablesilicone:Areviewofits history,immunology,technicalconsiderations,complications, andpotential.Plast.Reconstr.Surg.,118(3S):77S-84S,2006 3. Hönig,J.(2008).“CheekAugmentationwithBioAlcamidin FacialLipoatrophyinHIVSeropositivePatients”.Journalof CraniofacialSurgery19(4):1085–1088. 4. EvaluationoftheSafetyandEfficacyofBio-AlcamidforFacial SoftTissueAugmentation.MohammedAbdElMageed.Egypt,J. Plast.Reconstr.Surg.,Vol.31,No.2,July:129-137,2007 5. TreacyP.;GoldbergD.,UseofaBioPolymerFillerforFacial LipodystrophyinHIV-Positivepatientsundergoingtreatment withAntiRetroViralDrugs.JournalofDermatologicalSurgery Volume32,Number6,June2006,pp.804-808(5)June6,2006 6. GoldanO,GeorgiouI,Grabov-NardiniG,etal. Earlyandlate complicationsafteranonabsorbablehydrogelpolymerinjection: aseriesof14patientsandnovelmanagement.DermatolSurg 2007;33(Suppl2):S199-206. 7. RossAH,MalhotraR. Long-termorbitofacialcomplicationsof polyalkylimide4%(Bio-Alcamid).OphthalPlastReconstrSurg 2009;25(5):394-7. 8. DeBoulleK.Managementofcomplicationsafterimplantationof fillers.JCosmetDermatol.2004;3:2–15. www.aestheticmed.co.uk “Anecdotal reports also suggest some relief with the use of non-steroidal anti-inflammatory drugs (NSAIDs), antihistamines and tacrolimus.”