Mksap13 pulmonary medicine-and_critical_care
•Download as DOC, PDF•
6 likes•895 views

mksap

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mksap13 pulmonary medicine-and_critical_care
Similar to Mksap13 pulmonary medicine-and_critical_care (20)
More from sarfaraz ahmed
More from sarfaraz ahmed (10)
Recently uploaded
Recently uploaded (20)
Mksap13 pulmonary medicine-and_critical_care
- 1. 1 Pulmonary Medicine and Critical Care:Question 1 A 57-year-old man with advanced chronic obstructive pulmonary disease (COPD) and systemic hypertension is evaluated because of a 6-day history of productive cough and shortness of breath. He uses inhaled albuterol and ipratropium bromide, a long- acting theophylline preparation, and lisinopril. He uses supplemental oxygen at night and during ambulation. Ciprofloxacin is prescribed for an exacerbation of CO PD. Three days later, having had nausea for a day, the man is brought to the emergency department after he is found nearly unconscious. Arterial oxygen saturation is 89%, with the patient breathing room air. Electrocardiogram shows normal sinus rhythm with nonspecific ST-T changes in the lateral chest leads. Which of the following is likely to have interacted with ciprofloxacin and caused the symptoms that brought the man to the emergency department? A. Albuterol B. Theophylline C. Ipratropium bromide D. Lisinopril E. Oxygen Pulmonary Medicine and Critical Care:Question 2 A 17-year-old previously healthy man presents with a history of shortness of breath on exertion, particularly during basketball season, when he sometimes needs to sit down during practice to catch his breath. He does not notice any shortness of breath with routine activity. There is no family history of asthma. On physical examination, he is in no respiratory distress. His lungs are clear, with no wheezing during either tidal breathing or forced expiration. His heart is normal. Baseline spirometry is normal. What is the next diagnostic step? A. Allergy testing B. Methacholine challenge testing C. Exercise testing with postexercise spirometry D. Overnight oximetry E. Repeat lung volumes and diffusing capacity Pulmonary Medicine and Critical Care:Question 3 A 62-year-old woman is evaluated because of abnormal results on chest radiograph. She smokes 1 pack of cigarettes per day, with a 50-pack-year history. She has a morning cough productive of small amounts of yellow sputum. She has hypertension, for which she takes metoprolol, and type 2 diabetes mellitus, which is managed with diet and metformin therapy. Her body mass index is 30. Her blood pressure is 145/90 mm Hg. Chest radiograph shows a 1.5-cm nodule in the left upper lobe; no previous radiographs are available for comparison. Which of the following should be measured before sending this patient for a positron emission tomography scan to evaluate the nodule? A. Serum sodium B. Blood pressure C. Serum creatinine D. Serum glucose
- 2. 2 Pulmonary Medicine and Critical Care:Question 4 A 67-year-old man presents with a 6-month history of progressive exertional dyspnea and nonproductive cough. His weight has been stable. He was treated with several courses of oral antibiotics for “bronchitis” but his symptoms have not abated. He has a 40-pack-year cumulative smoking history; he stopped smoking 6 years ago. On physical examination, there are no signs of heart failure, but bibasilar coarse inspiratory crackles are audible, and he has early clubbing of the fingers. Chest radiograph shows increased reticular markings in the periphery of both lower lobes that were not evident on radiograph done 3 years ago. Which of the following additional aspects of the patient’s history are most important in evaluating him? A. Travel history B. Occupational history C. Allergy history D. Family history Pulmonary Medicine and Critical Care:Question 5 A 28-year-old woman is evaluated in February because of a 6-week history of severe cough. She describes coughing paroxysms often followed by emesis. She has no postnasal drip. On physical examination, the patient is afebrile. The chest is clear to auscultation and chest radiograph is normal. Laboratory studies show a leukocyte count of 12,000/μL, with 30% neutrophils, 65% lymphocytes, 2% monocytes, and 3% eosinophils. Which of the following is the most likely diagnosis? A. Gastroesophageal reflux disease B. Cough-variant asthma C. Bordetella pertussis D. Sinusitis E. Sarcoidosis Pulmonary Medicine and Critical Care:Question 6 A 25-year-old man is evaluated because of a 3-month history of episodic dyspnea at rest. The episodes occur approximately three times per week and are accompanied by cough. His symptoms awaken him at night approximately three times per month. He had asthma as a child, which resolved. His temperature is 36.5 C (97.7 SF), pulse rate 85/min and regular, respiration rate 14/min, and blood pressure 125/75 mm Hg. The only abnormality noted on physical examination is bilateral wheezing without crackles. Chest radiograph is normal. Spirometry shows a forced expiratory volume in 1 sec (FEV1) 78% of predicted, and a forced vital capacity 93% of predicted. He has a 17% (430 mL) improvement in FEV1 after using bronchodilators. Which of the following is the most appropriate treatment regimen for this patient? A. Albuterol B. Albuterol and a long-acting β-agonist C. A long-acting β-agonist D. Albuterol and a low-dose inhaled corticosteroid
- 3. 3 Pulmonary Medicine and Critical Care:Question 7 A 67-year-old woman is evaluated in the emergency department because of a 2-day history of fever and a cough productive of purulent sputum. She is intubated for hypoxic respiratory failure due to pneumonia and hospitalized in the intensive care unit. Her medical history is remarkable only for hypertension for which she takes a calcium channel blocker. She has never worked outside the home, has no pets, and has not traveled recently. Which of the following would be appropriate initial antibiotic therapy? A. A second-generation cephalosporin and macrolide B. A second-generation cephalosporin C. A third-generation cephalosporin, aminoglycoside, and macrolide D. An antipseudomonal β-lactam/β-lactamase combination and fluoroquinolone Pulmonary Medicine and Critical Care:Question 8 A 38-year-old woman who has never smoked is evaluated because of well- circumscribed nodule in the right lower lobe, which was discovered on a chest radiograph during a routine physical examination. There is no family history of cancer, the patient has never had cancer herself, and the lesion is completely calcified. A CT scan of the chest done 2 years ago showed a 0.8-cm nodule in the right lower lobe. Another CT scan is ordered, and it shows the nodule is eccentrically calcified and has grown. What is the best next step in this patient’s management? A. Lobectomy B. Transthoracic needle aspiration C. Positron emission tomography scan D. Remove the nodule Pulmonary Medicine and Critical Care:Question 9 A 67-year-old man with a history of chronic obstructive pulmonary disease is evaluated because of a 3-month history of progressive dyspnea and wheeze. One year ago, the patient had five-vessel coronary artery bypass graft surgery with a prolonged postoperative stay in the intensive care unit because of acute respiratory distress syndrome. On physical examination the patient has a persistent wheeze. His jugular venous pressure is normal. The flow-volume loop is shown.
- 4. 4 Results of pulmonary function tests are as follows: Forced expiratory volume in 1 sec (FEy1) 2.22 L (64% of predicted) Forced vital capacity (FVC) 4.96 L (107% of predicted) FEV1/FVC 45% Forced expiratory flow (FEF25%-75%) 2.13 L/sec (60% of predicted) Which of the following is the most likely cause of this patient’s worsening dyspnea? A. Exacerbation of chronic obstructive pulmonary disease B. Congestive heart failure C. Late seq uela of acute respiratory distress syndrome D. Tracheal stenosis E. Constrictive pericarditis Pulmonary Medicine and Critical Care:Question 10 A 59-year-old woman is evaluated because of shortness of breath of acute onset. She has developed worsening insomnia and fatigue since she was diagnosed with adenocarcinoma of the breast 2 months ago. There is no known metastatic disease and therapy is to begin next week. She has no cough or chest pain. Her temperature is 37.2 C (98.9 SF), pulse rate is 105/min, respiration rate is 22/min, and blood pressure is 158/88 mm Hg. Arterial oxygen saturation measured by pulse oximetry with the patient breathing room air is 95%. Her lungs are clear to auscultation. There is no jugular venous distention. Heart sounds are normal without murmurs, rubs, or gallops. The abdomen is not tender, and there is no edema of the extremities. Chest radiograph shows no abnormalities, and electrocardiogram shows only sinus tachycardia. Ventilation/perfusion scan shows two large segmental perfusion defects; the ventilation scan shows only mildly heterogeneous washout. Which one of the following is the best next step in the management of this patient? A. CT scan using an intravenous radiographic contrast agent B. Intravenous thrombolytic therapy C. Intravenous heparin therapy D. Doppler ultrasound imaging of the lower extremities Pulmonary Medicine and Critical Care:Question 11 A 70-year-old man is referred because of 2-year history of progressive exertional dyspnea and an abnormal lung examination. He has no significant cough, hemoptysis, or chest pain, and he has never smoked. He worked as an insulation installer for 30 years and retired 10 years ago. On physical examination, fine end-inspiratory crackles are auscultated at both lung bases. He has clubbing of the fingers. Chest radiograph and pulmonary function tests are ordered. In addition to bilateral lower lobe reticular interstitial opacities, what radiographic feature is likely to be found in this patient? A. Eggshell calcification of lymph nodes B. Upper lobe pulmonary nodules C. Calcified pleural plaques D. Cavitating pulmonary nodules and masses E. Bilateral hilar adenopathy
- 5. 5 Pulmonary Medicine and Critical Care:Question 12 A 46-year-old woman who works as a nurse is evaluated because of a 2-year history of episodic wheezing and a squeaky voice.” This past spring, her symptoms worsened, requiring her to seek medical attention; she was placed on a short -acting β-agonist that did not provide much relief. She has no history of wheezing and says that these changes began after a severe influenza infection 3 years ago. Currently she feels well and has had no symptoms for several months; she is not taking any medications. Physical examination shows no abnormalities, and baseline spirometry is normal. What is the best test to evaluate this patients condition? A. Methacholine challenge testing B. Bronchoscopy to evaluate her trachea C. Exercise echocardiogram D. CT scan of the sinuses Pulmonary Medicine and Critical Care:Question 13 A 43-year-old man is evaluated because he falls asleep while working at his computer during the day. He typically goes to bed at 11 PM and sleeps until 6AM. He is uncertain whether he snores, and he has no history of choking arousals. Even though he sleeps 7 hours per night during the week, he does not feel that his sleep is restful; he says that he tosses and turns throughout the night. Nearly every morning he has a headache. He drinks coffee at work to avoid falling asleep. He has not had any recent automobile accidents. He has no other medical problems, except that he admits to recent problems with sexual dysfunction. He takes no medicines and drinks alcohol only occasionally. On physical examination, he is 175 cm (69 in) tall and weighs 81 .6 kg (180 Ib). His neck is 44.5 cm (17.5 in), and he has a crowed oropharynx. His blood pressure is 125/70 mm Hg. His palate is low-lying, and his uvula is elongated. Chest and heart examination reveals no abnormalities. He has no peripheral edema or clubbing. Which of the following risk factors, considered alone, is most predictive of obstructive sleep apnea in this patient? A. Drinking alcohol in the evening B. Excessive daytime sleepiness C. Nocturnal sexual dysfunction D. Neck circumference E. Morning headaches Pulmonary Medicine and Critical Care:Question 14 A 25-year-old man with cystic fibrosis returns to the emergency department because of a third episode of abdominal pain with nausea and vomiting wit hin the past 2 years. He takes trimethoprim-sulfamethoxazole for suppression of chronic respiratory infection and pancrelipase for treatment of pancreatic insufficiency. On physical examination, he is afebrile, and his blood pressure is normal. Coarse crackles and short wheezes are heard in both lungs. His abdomen is distended, firm, and diffusely tender. There is no jugular venous distention or peripheral edema. His total leukocyte count is 83004±. Liver function studies and serum amylase and lipase levels are normal. An abdominal radiograph suggests partial small bowel obstruction. Which of the following is the most likely cause of this patient’s abdominal pain? A. Exacerbation of chronic intestinal pseudo-obstruction B. Irritable bowel syndrome C. Diverticulitis D. Distal intestinal obstruction syndrome E. Exacerbation of chronic pancreatitis
- 6. 6 Pulmonary Medicine and Critical Care:Question 15 A 43-year-old man is evaluated because he is unable to complete 18 holes of golf without gasping for air. He has smoked 1 pack of cigarettes per day for 20 years. On physical examination, he has fine inspiratory crackles in both lower lobes. He has no wheezing or clubbing but does have trace edema of the lower extremities. Cardiac examination reveals i and 2 are normal without murmurs. A chest radiograph is normal. Lung function studies show forced expiratory volume in 1 sec (FEV1) 80% of predicted, forced vital capacity (FVC) 75% of predicted, and FEV1/FVC ratio of 90%. Lung volumes are reduced and diffusing lung capacity for carbon monoxide (DLCO) is 55% of predicted. Echocardiography shows normal left ventricular systolic and diastolic function without valvular abnormalities. What is the best next step in this patient’s evaluation? A. Left heart catheterization B. Cardiac stress test C. HRCT scan of the chest D. Bronchoscopy E. Pulmonary angiography Pulmonary Medicine and Critical Care:Question 16 A 72-year-old woman with a history of rheumatoid arthritis is evaluated because of persistent cough, purulent sputum production, and occasional scant hemoptysis. She reports no fever, but says she has difficulty gaining weight. She has never smoked cigarettes. She is hospitalized because of tachypnea and hypoxia. Spirometry shows moderately severe obstructive impairment. Chest radiograph shows tramlines without infiltrate. Gram stain of the sputum shows numerous leukocytes but no bacteria; culture results are pending. Previous IgE levels were normal. There is no eosinophilia. An immediate skin test forAspergillus is negative. A tuberculin skin test performed last year was nonreactive. Which of the following is appropriate therapy for this patient? A. Intravenous fluoroquinolone and aminoglycoside B. A β-lactam/β-lactamase combination C. Itraconazole D. A new-generation macrolide Pulmonary Medicine and Critical Care:Question 17 A 57-year-old man is evaluated because of a 1-year history of dyspnea on exertion. Examination reveals swan-neck deformities of the second, third, and fourth digits, and a boutonniere deformity of the fifth digit of both hands. He has 2+ pitting edema and chronic venous stasis changes of the lower extremities. The patient weighs 191 kg (421 Ib). Laboratory evaluation reveals a serum rheumatoid factor of 87 U/mL, and arterial blood gas values, with the patient breathing room air, are 296 mm Hg, PC0235 mm Hg, and pH 7.44. Results of pulmonary function tests are as follows. Forced expiratory volume in 1 sec (FEV1) 2.06 L (84% of predicted) Forced vital capacity (FVC)2.74 L (83% of predicted) FEV1/FVC 75% Forced expiratory flow (FEF25%-75%) 1 .58 L/sec (57% of predicted) Total lung capacity 4.01 L (76% of predicted) Functional residual capacity2.13 L (72% of predicted) Expiratory reserve volume0.16 L (10% of predicted) Diffusing lung capacity for carbon monoxide (DLCO) 23.65 mL/min/mm Hg (121% of predicted)
- 7. 7 Which of the following is the most likely cause of the patients dyspnea? A. Bronchiolitis obliterans B. Interstitial lung disease C. Congestive heart failure D. Obesity Pulmonary Medicine and Critical Care:Question 18 A 59-year-old man with advanced chronic obstructive pulmonary disease is evaluated because of a daily cough productive of white or yellow sputum, dyspnea after climbing one flight of stairs, and a recent 4.5-kg (10-Ib) weight loss with no associated change in appetite or food intake. The patient stopped smoking 4 years ago. On physical examination, he has diminished breath sounds throughout all lung fields. Arterial oxygen saturation measured by pulse oximetry with the patient at rest, breathing room air, is 87%. Chest radiograph suggests hyperinflation of the lungs but shows no pulmonary infiltrates or abnormalities of the cardiac silhouette. Pulmonary function studies show a forced expiratory volume in 1 sec (FEy1) 39% of predicted and forced vital capacity (FVC) 78% of predicted. Which of the following may prolong life in this patient? A. Albuterol B. Ipratropium bromide C. Theophylline D. Supplemental oxygen Pulmonary Medicine and Critical Care:Question 19 A 52-year-old woman is evaluated because of a 1-year history of progressive dyspnea on exertion. She is short of breath when climbing one flight of stairs and when dressing. She is a former heavy cigarette smoker and has a long history of hypertension. On physical examination, she has elevated jugular venous distention, a pronounced cardiac pulmonic valve component, and mild pitting edema of both ankles. Results of complete blood count, serum electrolytes, renal function, and liver function tests are normal. Tests for antinuclear antibodies, rheumatoid factor, HIV, and anti-Scl-70 antibodies are negative. Chest radiograph shows prominent central pulmonary arteries; the lung fields are clear. Echocardiogram shows concentric left ventricular hypertrophy with normal left ventricular systolic function (ejection fraction 55%) and a mildly dilated right ventricle with normal function. The aortic, mitral, and tricuspid valves are normal in structure. The estimated pulmonary artery systolic pressure measured at rest is 59 mm Hg (assuming an estimated right atrial pressure of 10 mm Hg). Spirometry and lung volumes are normal. Diffusing lung capacity for carbon monoxide (DLCO) is 40% of predicted. Ventilation/perfusion scan shows normal ventilation and mild heterogeneity of perfusion but no segmental or larger defects. Right heart catheterization shows right atrial pressure 10 mm Hg, right ventricular pressure 50/10 mm Hg, pulmonary artery pressure 50/20 mm Hg, pulmonary capillary wedge pressure 26, cardiac output 3.1 L/min, cardiac index 2.0 L/min/m2. Which one of the following is the most likely cause of this patients pulmonary hypertension? A. Left ventricular diastolic dysfunction B. Chronic pulmonary embolism C. Primary pulmonary hypertension D. Pulmonary veno-occlusive disease E. Constrictive pericarditis
- 8. 8 Pulmonary Medicine and Critical Care:Question 20 A 45-year-old man is evaluated because of a 6-month history of progressive left shoulder pain, which has not responded to nonsteroidal medications. He also has anorexia of recent onset, with a 2.3-kg (5-Ib) weight loss. He currently smokes 2 packs of cigarettes per day and has a 60-pack-year smoking history. On physical examination, he is in mild distress. He is afebrile; pulse rate is 80/min and regular, respiration rate is 14/min, and blood pressure is 120/65 mm Hg. Musculoskeletal examination shows no abnormalities, and he has normal strength and range of motion in his left arm and shoulder. Radiograph of his left shoulder shows no abnormalities, but radiography of his chest shows a mass in the left apex. CT scan of the chest confirms a posterior left upper lobe mass, which appears to be abutting the vertebral bodies. All mediastinal nodes are <1 cm in greatest dimension. Serum sodium, calcium, and alkaline phosphatase levels are normal, as are liver function studies. Pulmonary function tests show a forced expiratory volume in 1 sec (FEV1) of 2.5 L and forced vital capacity (FVC) of 4.0 L. Bronchoscopy shows no endobronchial lesions, but results of transbronchial biopsy of a specimen from the left upper lobe show squamous cell carcinoma. What is the best next step in this patient’s management? A. MRI of the chest B. HRCT scan of the left upper lobe C. Resection of the mass D. CT scan of the brain E. Radionuclide bone scan Pulmonary Medicine and Critical Care:Question 21 A 34-year-old woman is evaluated because of a 1-year history of increased dyspnea on exertion. She has no symptoms at rest but has to stop about 15 minutes into her aerobics class because of dyspnea and occasional cough. She usually recovers fully in about an hour. One year ago she was able to do aerobics for 45 minutes without difficulty. Her vital signs are normal, and her physical examination is normal, including clear breath sounds. Baseline spirometry is also normal. Which of the following would be best next step in the management of this patient? A. Oral leukotriene inhibitors B. Long-acting theophylline C. Inhaled ipratropium bromide prior to exercise D. Inhaled albuterol prior to exercise E. Inhaled corticosteroids Pulmonary Medicine and Critical Care:Question 22 A 47-year-old black man is evaluated because of a 2-month history of cough. Three months ago hypertension was diagnosed, for which he takes hydrochiorothiazide and benazepril. He attributes his cough to the change in the weather. He has a history of gastroesophageal reflux disease that is well controlled with a proton-pump inhibitor. He has no history of asthma. Which of the following would be the most appropriate next step? A. CT scan of the sinuses B. pH probe C. Methacholine challenge testing D. Discontinuation of his angiotensin-converting enzyme inhibitor E. Allergy testing
- 9. 9 Pulmonary Medicine and Critical Care:Question 23 A 66-year-old woman is brought to the emergency department after being rescued from a burning building. Oxygen was administered at the scene, and the oxygen saturation level was 100% by pulse oximetry on 100% oxygen delivered by face mask during transport to the emergency department. At the hospital, oxygen flow is decreased to maintain oxygen saturation at >92%. The patient is awake but appears somewhat confused. She complains of feeling dyspneic. On physical examination, she has first- and second-degree burns over 50% of her body. Bilateral crackles are audible in the lower lung fields and coarse breath sounds bilaterally. Measurement of arterial blood gases shows a partial oxygen pressure of 45 mm Hg, with oxygen saturation of 94% by pulse oximetry. Which of the following explains the discrepancy between the arterial blood gas findings and the oximetry? A. The carboxyhemoglobin level is elevated. B. The carbon dioxide level is elevated. C. The methemoglobin level is elevated. D. The total hemoglobin is elevated. E. The patient is anemic. Pulmonary Medicine and Critical Care:Question 24 A 62-year-old man with chronic obstructive pulmonary disease is interested in lung- volume-reduction surgery. After a course of pulmonary rehabilitation, his forced expiratory volume in 1 sec (FEV1) is 17% of predicted and his diffusing lung capacity for carbon monoxoide (DLCO) is 19% of predicted. A CT scan of the chest shows heterogeneously distributed emphysema. Which of the following statements about lung-volume-reduction surgery is true of this patient? A. He may be an excellent candidate because of his low FEV1 and DLCO. B. He is not a candidate because of his heterogeneously distributed emphysema and his low FEV1 and DLCO. C. He is not a candidate because of the low FEV1. D. He is not a candidate because of the low DLCO. Pulmonary Medicine and Critical Care:Question 25 A 45-year-old man is evaluated because he had a tuberculin skin test performed as part of an employment physical and it was read as positive, with induration of 22 mm. He is asymptomatic. The patient emigrated from Sri Lanka 15 years ago. He has no recollection of exposure to tuberculosis, but he remembers being told that he was given a ‘tuberculosis vaccine as a child. A chest radiograph is interpreted as normal. Which of the following is the most appropriate next step in this patient’s management? A. Treatment for active tuberculosis should be initiated. B. Treatment for latent tuberculosis should be initiated. C. Further testing is warranted to look for active tuberculosis, and sputum induction or bronchoscopy should be performed. D. Skin testing should not have been performed; his reac tion is a false-positive secondary to his earlier vaccination.
- 10. 10 Pulmonary Medicine and Critical Care:Question 26 A 53-year-old woman with a history of mild persistent asthma is evaluated because of a recent increase in her symptoms, with dyspnea and cough occurring daily and a cough that awakens her once a week. She is currently using low-dose inhaled corticosteroids. She has no symptoms of rhinitis or gastroesophageal reflux. On physical examination, she has intermittent wheezing bilaterally. Which of the following is the most appropriate change in her therapy? A. Initiate azithromycin therapy. B. Add a nebulized short-acting β-agonist. C. Add inhaled ipratropium bromide. D. Add a long-acting β-agonist. E. Add a leukotriene inhibitor. Pulmonary Medicine and Critical Care:Question 27 A 57-year-old man is evaluated because of a 3-month history of chronic cough associated with occasional streaky hemoptysis. He has no other systemic symptoms and has not traveled recently. He stopped smoking cigarettes 2 years ago, after a 45-pack-year smoking history. He has had two episodes of pneumonia in the past year, both in the right upper lobe, which resolved with antibiotics. On physical examination, he has decreased breath sounds over the right chest posteriorly. Chest radiograph shows a 3-cm proximal mass in the right upper lobe. Bronchoscopy shows an endobronchial mass in the right upper lobe, 3 cm from the carina. Biopsy of the mass shows it to be squamous cell carcinoma. A CT scan of the chest with contrast shows a speculated mass in the proximal right upper lobe with distal atelectasis. Two mediastinal nodes are found, each 1.5 cm in diameter, one in the right hilum and one in the subcarinal area. Pulmonary function is normal, with a forced expiratory volume in 1 sec (FEV1) of 3.1 L (95% of predicted). Which of the following is the best next step in the management of this patient? A. Resection of the mass B. Mediastinal node sampling C. Chemotherapy D. Radiation therapy E. Palliative care Pulmonary Medicine and Critical Care:Question 28 A 70-year-old man is evaluated because of shortness of breath. He has noted progression of his symptoms, primarily with exertion over the past 6 months. He is unable to walk one flight of stairs or two blocks on level ground without becoming short of breath. He has no chest pain, paroxysmal nocturnal dyspnea, orthopnea, or lower extremity edema. He has a 40-pack-year history of cigarette smoking, but stopped smoking 10 years ago. He worked in a naval shipyard 50 years ago but has spent most of his working life as a schoolteacher. On physical examination, his respiration rate is 18/min but he does not appear short of breath. Examination of the chest shows an increased anterior-posterior diameter. On auscultation he has diffusely decreased breath sounds and a prolonged expiratory phase with no wheezing. He has no cyanosis or clubbing. Spirometry shows forced expiratory volume in 1 sec (FEV1) 55% of predicted and forced vital capacity (FVC) 80% of predicted with a ratio of FEV1 to FVC 60%. Which of the following is the best test to evaluate this patients condition? A. Lung volumes and diffusing capacity B. Echocardiography C. Exercise spirometry D. Methacholine challenging testing
- 11. 11 Pulmonary Medicine and Critical Care:Question 29 A 57-year-old woman is evaluated because of a 6-month history of progressive dyspnea. She has never smoked cigarettes. She has been treated on several occasions for a “COPD exacerbation” with intravenous corticosteroids with some relief in symptoms. She states that symptoms are particularly bothersome in the evening. Pulmonary function tests are as follows: Forced expiratory volume in 1 sec (FEV1) 2.06 L (84% of predicted) Forced vital capacity (FVC)2.74 L (83% of predicted) FEV1/FVC 75% Maximum voluntary ventilation63 L/min (65% of predicted) Maximum inspiratory pressure39 cm H20 (52% of predicted) Maximum expiratory pressure58 cm H20 (42% of predicted) Total lung capacity 4.01 L (76% of predicted) Functional residual capacity 2.13 L (72% of predicted) Residual volume 1.42 L (73% of predicted) Diffusing lung capacity for carbon monoxide (DLco) 19.39 mL/min per mm Hg (99% of predicted) Which of the following is the most likely cause of this patients dyspnea? A. Chronic thromboembolic disease B. Chronic obstructive pulmonary disease C. Idiopathic pulmonary fibrosis D. Myasthenia gravis Pulmonary Medicine and Critical Care:Question 30 A man on a mountain climbing expedition is evaluated because of shortness of breath and a 2-day history of coughing. He is unable to keep pace with the other climbers. His cognition appears normal, and he is not drowsy. Present altitude is 5000 m (16,000 feet), and the group has ascended 2500 m (8000 feet) in the past 2 days. Which of the following statements is accurate regarding this patient’s condition? A. Carbonic anhydrase inhibitors are the treatment of choice. B. Rate of ascent contributes minimally to this disorder. C. Dexamethasone is the treatment of choice. D. Oxygen and descent to lower altitude are the treatment of choice. E. The patient is not at increased risk for recurrence of this disorder on future climbs. Pulmonary Medicine and Critical Care:Question 31 A 67-year-old man has a 12-year history of seropositive rheumatoid arthritis currently well controlled with methotrexate, 12.5 mg orally once weekly, and prednisone, 5 mgld orally. He smokes 2 packs of cigarettes per day. He has noted some subtle decrease in exercise tolerance and an occasional dry cough. On physical examination he has stable deformities of the hands and wrists consistent with rheumatoid arthritis and several old subcutaneous nodules on the extensor surfaces of his forearms. He has no cervical adenopathy, no abnormal jugular venous distention, and no peripheral edema. Coarse crackles are audible at both lung bases, and there is dullness to percussion with decreased breath sounds on the left. Chest radiograph shows minimal bilateral reticular infiltrates and a moderate left pleural effusion. Thoracentesis yields straw-colored fluid in which protein is measured at 4.5 g/dL (serum 5.6 gIdL) and glucose at 30 mg/dL (serum = 106 mgldL). Pulmonary function studies demonstrate: Forced expiratory volume in 1 sec (FEy1) 78% of predicted Forced vital capacity (FVC)75% of predicted
- 12. 12 FEV1/FVC 86%, Total lung capacity 70% of predicted Residual volume 72% of predicted Diffusing lung capacity for carbon monoxide (DLco) 86% of predicted Which of the following is most likely true regarding this patient’s lung disease? A. The crackles strongly suggest a diagnosis of congestive heart failure. B. This patient has an empyema in need of immediate surgical drainage. C. The patient has recurrent aspiration pneumonia. D. The patient’s signs and symptoms are consistent with rheumatoid arthritis- associated interstitial lung disease. Pulmonary Medicine and Critical Care:Question 32 A 52-year-old man is evaluated in the emergency department because of mild shortness of breath and chest pain, which began after he carried heavy suitcases from his car following a 9-hour drive. He has a history of chronic obstructive pulmonary disease, peptic ulcer disease, and Hodgkin’s lymphoma in remission 4 years after radiation therapy. One year ago, after an automobile accident, he had deep vein thrombosis of the right leg for which he received warfarin therapy for 3 months. Lungs are clear to auscultation. Heart sounds are regular and are not accompanied by gallops or murmurs. There is mild pitting edema at both ankles, which the patient says has been present since the automobile accident. Chest radiograph and electrocardiogram show no evidence of acute disease. A ventilation/perfusion nuclear scintigraphy scan shows several subsegmental matched defects and is interpreted as indicative of a low probability of pulmonary embolus. Which of the following is the best next step in the management of this patient? A. Restart heparin. B. Measure arterial blood gases. C. Measure the D-dimer level in the serum and re-initiate anticoagulation therapy if it is elevated. D. Measure the D-dimer level in the serum and perform Doppler ultrasound imaging of the lower extremities if it is elevated. Pulmonary Medicine and Critical Care:Question 33 A 70-year-old woman resident of a nursing home is evaluated in the emergency department because of decreasing mental status and hypothermia. She has a history of stroke and is currently taking only aspirin. She has been able to eat on her own and there have been no witnessed aspirations. She has not been treat ed recently with antibiotics. Her leukocyte count is 12,000/μL, and her hemoglobin is 12 gIdL. Serum electrolytes are within normal limits and she has mild chronic renal insufficiency. Chest radiograph shows a small interstitial infiltrate in the right lower lung field. She receives traditional empiric treatment for community-acquired pneumonia. Therapy for which of the following should also be considered? A. Pseudomonas aeruginosa B. Anaerobic bacteria C. Enteric gram-negative organisms D. Aspergillus fumigatus E. Mycobacterium tuberculosis
- 13. 13 Pulmonary Medicine and Critical Care:Question 34 A 28-year-old man with cystic fibrosis who was hospitalized 3 days ago to receive antibiotic therapy is evaluated because he has developed hemoptysis. He is a thin man in mild respiratory distress. Twenty minutes ago, he coughed up approximately 75 mL of clotted blood, but has not had any further bleeding. His vital signs are stable, and pulse oximetry is 92% with the patient breathing 2 L oxygen by nasal cannula. Bilateral crackles are audible on chest auscultation. He has a scaphoid abdomen. The remainder of his examination is normal. What is the best next step in this patient’s management? A. Administer ε-aminocaproic acid as a plasminogen-to-plasmin inhibitor. B. Arrange pulmonary consultation for urgent bronchoscopy. C. Change his antibiotics to cover resistantPseudomonas. D. Arrange an interventional radiology consultation for embolization. E. Arrange an anesthesia consultation for selective intubation. Pulmonary Medicine and Critical Care:Question 35 A 34-year-old woman, a nurse, is evaluated after having made a number of trips to the emergency department because of breathing difficulties that were treated as exacerbations of asthma. The patient was treated in the emergency department with nebulized β-agonists and a corticosteroid. The patient has been given prescriptions for inhaled corticosteroids, but she has never had a documented objective change in lung function after using them. Spirometry in an outpatient setting between exacerbations has been normal, and measurement of arterial blood gases done during one of her visits to the emergency department was normal. She has never smoked cigarettes. She has no symptoms of rhinitis, no nocturnal symptoms, no recent viral infections, and no symptoms of gastroesophageal reflux disease. On physical examination, she is anxious but in no respiratory distress. She is afebrile. Her pulse rate is 85/min and regular; respiration rate is 16/min, and blood pressure is 130/75 mm Hg. Her breathing is unlabored, and she has inspiratory and expiratory wheezes but is otherwise normal. What is the most likely explanation for this patients lack of response to corticosteroid therapy? A. The patient has chronic obstructive pulmonary disease. B. The patient has vocal cord dysfunction. C. The patient has corticosteroid-resistant asthma. D. The patient has asthma with allergic bronchopulmonary aspergillosis. Pulmonary Medicine and Critical Care:Question 36 An obese 62-year-old man is evaluated because of heartburn and frequent throat clearing. Gastroesophageal reflux disease (GERD) is diagnosed and therapy with a proton-pump inhibitor, twice daily, is initiated. He is advised of lifestyle modifications that help prevent GERD. Six weeks later, he is re-evaluated because the cough, although somewhat better, persists. He has no postnasal drip. His heartburn has resolved. Which of the following is the best next step in this patients management? A. Change his medication to intranasal corticosteroids and antihistamines. B. Order 24-hour esophageal pH monitoring. C. Refer him for fundoplication. D. Continue the proton-pump inhibitor therapy and re-evaluate him in 6 weeks.
- 14. 14 Pulmonary Medicine and Critical Care:Question 37 A 66-year-old woman with chronic obstructive pulmonary disease is evaluated because of chronic cough and dyspnea. She currently uses a long-acting bronchodilator twice per day, an inhaled corticosteroid twice per day, ipratropium four times per day, and albuterol four to six times per day. She smokes 1 pack of cigarettes per day. On physical examination, her vitals signs are normal. Her oxygen saturation at rest and with exertion is 94%. She has diminished breath sounds, a prolonged expiratory-to-inspiratory phase, and no wheezes. Her heart rate and rhythm are regular, with a normal i, a physiologically split S2, and no murmurs or rubs. Chest radiograph reveals hyperinflation, increased retrosternal airspace, and flattened hemidiaphragms bilaterally. Which of the following should be initiated at this time to address this patient’s cough and dyspnea? A. Increase her use of the long-acting bronchodilator. B. Prescribe supplemental oxygen. C. Provide emergency treatment for a tension pneumothorax. D. Discuss techniques to help her to quit smoking. E. Increase her dosage of inhaled corticosteroid. Pulmonary Medicine and Critical Care:Question 38 A 60-year-old man with a history of alcohol abuse is evaluated because of the insidious onset of dyspnea over the course of 6 weeks. He has no cough, chest or abdominal pain, or hemoptysis. He smoked 1.5 packs of cigarettes per day for 25 years and stopped smoking 4 years ago. He has a moderate-sized right pleural effusion. Chest radiograph shows the effusion with minimal contralateral mediastinal shift and is otherwise normal. Pleural fluid analysis shows clear yellow fluid with 500 nucleated cells/μL, 10% neutrophils, 25% lymphocytes, 60% macrophages, and 5% mesothelial cells. Pleural fluid values are as follows: Total protein 1.1 g/dL Serum lactate dehydrogenase4l U/L Serum amylase 20 U/L Glucose 100 mg/dL pH 7.45 Ratio of pleural fluid to serum (PF/S) total protein 0.2 Ratio of pleural fluid to serum lactate dehydrogenase (upper limits of normal) 0.35 Other laboratory results show a serum albumin of 2.4 g/dL, an INR of 1 .5, and a normal urinalysis. Electrocardiogram is normal. Which of the following is the most likely diagnosis? A. Congestive heart failure B. Hepatic hydrothorax C. Chronic pancreatitis D. Lung cancer E. Nephrotic syndrome
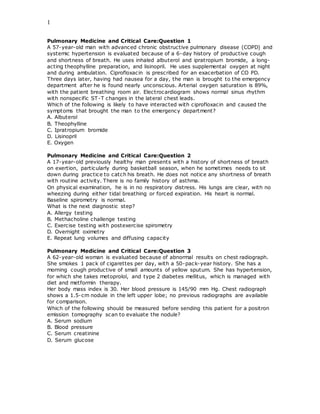
- 15. 15 Pulmonary Medicine and Critical Care:Question 39 A 45-year-old man alternates day, evening, and night shifts at weekly intervals in a factory. He drinks six to eight cups of coffee per day to fight off episodes of sleepiness. His wife reports that he snores and moves his legs often while sleeping. The accompanying image represents one segment of his overnight polysomnogram. Which of the following disorders does this polysomnogram show? A. Obstructive sleep apnea B. Restless legs syndrome C. Narcolepsy D. Central sleep apnea E. Cheyne-Stokes breathing Pulmonary Medicine and Critical Care:Question 40 A 67-year-old man is evaluated because of a 3-week history of cough productive of blood-streaked sputum. A chest radiograph shows an infiltrate in the right upper lobe. He is treated with antibiotics for 2 weeks, but the blood-streaked sputum persists. A CT scan of the chest shows a mass obstructing the right upper lobe and evidence of postobstructive pneumonitis. Examination of the mediastinum shows enlarged lymph nodes in the right paratracheal space. A positron emission tomography (PET) scan shows uptake in the mass itself and in the lymph nodes in the right paratracheal space. Fiberoptic bronchoscopy is performed; an endobronchial lesion is identified and a sample is taken for biopsy. The biopsy shows squamous cell carcinoma. Which of the following is the best next step in this patients management? A. Refer him for radiation therapy. B. Perform immediate mediastinoscopy. C. Refer him for surgery. D. Perform a repeat positron emission tomography scan.
- 16. 16 Pulmonary Medicine and Critical Care:Question 41 A 39-year-old woman is evaluated because of an abnormality on a chest radiograph obtained as a pre-employment screen. She is a lifetime nonsmoker. She has worked for several years as an assistant in a research laboratory specializing in molecular genetic screening assays. The patient’s chest radiograph is shown. Which of the following findings would warrant a trial of oral corticosteroid therapy? A. Bilateral anterior uveitis B. Hypercalcemia C. Fever and tender red nodules over the anterior shins D. Persistent cough Pulmonary Medicine and Critical Care:Question 42 A 72-year-old woman is evaluated because of morning headaches and swelling in the lower extremities that worsens as the day progresses. She is able to sleep supine, using one pillow at night, and notices shortness of breath walking distances greater than 20 feet. On physical examination, significant findings include diminished breath sounds, distant heart sounds, with pulmonic valve component equal in intensity to aortic valve component, and paradoxical splitting of the S2. Laboratory finding include a PaO2of 59mm Hg, PaCO2of44 mm Hg, and pH of 7.41. Electrocardiogram shows right ventricular hypertrophy with cor pulmonale and right axis deviation. Which of the following is the best rationale for long-term oxygen therapy for this patient? A. The PaO2 is less than or equal to 65 mm Hg (Medicare guideline) B. Her morning headaches C. Evidence of cor pulmonale and a PaO2 between 55 and 60 mm Hg D. Dyspnea
- 17. 17 Pulmonary Medicine and Critical Care:Question 43 A 57-year-old man with severe persistent asthma is evaluated on routine follow-up. He states that his asthma has been under good control for the last 3 months on high-dose inhaled corticosteroids and a long-acting β-agonist. He uses a short-acting β-agonist only three times per week as a rescue medication, and he has nocturnal symptoms very rarely. Peak expiratory flows have been stable. His physical examination is normal, including clear breath sounds, and spiromet ry is normal. It is decided that he will keep using the short-acting β-agonist as a rescue medication. Which of the following is the best next step in this patient’s management? A. Stop the long-acting β-agonist and decrease the dose of inhaled corticosteroid. B. Continue current therapy and have the patient return in 6 months. C. Stop the long-acting β-agonist and maintain the dose of inhaled corticosteroid. D. Continue the long-acting β-agonist and decrease the dose of inhaled corticosteroid. Pulmonary Medicine and Critical Care:Question 44 A 71-year-old woman is evaluated because of progressive fatigue, weakness, and dyspnea on exertion. A former smoker, she has a history of advanced emphysema and is on continuous long-term oxygen therapy. She currently uses a long-acting bronchodilator twice per day, theophylline and an inhaled corticosteroid twice per day, ipratropium four times per day, and albuterol four to six times per day. Physical examination is normal. Heart and lung examinations are consistent with long-standing, advanced emphysema. Her laboratory and radiographic findings are unremarkable. Which of the following is the best next step in this patient’s management? A. Refer her to a multidisciplinary rehabilitation program. B. Prescribe an antidepressant medication. C. Prescribe an empiric course of “pulse dose” corticosteroids at 500 mg/d for 3 consecutive days. D. Explain to her that she is on maximal medical therapy and that nothing more can be done for her emphysema. Pulmonary Medicine and Critical Care:Question 45 A 40-year-old worker is rescued from a fire at a fabrics warehouse. He is comatose and hypotensive. Paramedics administer 100% oxygen by face mask, initiate intravenous fluids, and transfer him to the emergency department. Upon arrival in the emergency department, he is still comatose. His pulse rate is 70/min, and respiration rate is 26/min. Mean arterial pressure is 50 mm Hg, and the monitor shows abundant ventricular ectopy. No burns are noted, and the patient is not cyanotic. There are no obvious signs of trauma. Pupils are reactive. Scattered rhonchi are audible. Neurologic examination shows lack of motor response to application of a painful stimulus. Laboratory studies: Serum sodium 143 meq/L Serum potassium 4 meq/L Serum chloride 100 meq/L Serum bicarbonate 10 meq/L Arterial blood gases PO2 300 mm Hg PCO2 25 mm Hg pH 7.20
- 18. 18 Carboxyhemoglobin 15% (normal = 1% to 3%) Endotracheal intubation is performed, and additional fluid is administered. Treatment with pressor agents and hyperbaric oxygen is initiated. What is the best next step in this patient’s management? A. Initiate intravenous bicarbonate therapy. B. Administer intravenous sodium thiosulfate. C. Order a CT scan of the brain and a cervical spine series. D. Administer intravenous methylene blue. E. Measure serum osmolarity, and calculate the osmolal gap. Pulmonary Medicine and Critical Care:Question 46 A 47-year-old man is evaluated because of cough that has persisted for 6 months. He has no postnasal drip, wheeze, or heartburn. His physical examination, chest radiograph, and spirometry are normal. He receives no benefit from a 3-month trial of twice-daily proton-pump inhibitors, intranasal corticosteroids, and antihistamines. He has a family history of allergies. Which of the following would suggest the diagnosis of this patients chronic cough? A. 24-hour esophageal pH monitoring B. CT scan of the sinuses C. Bronchoscopy D. Methacholine challenge testing E. CT scan of the chest Pulmonary Medicine and Critical Care:Question 47 A 67-year-old man with chronic obstructive pulmonary disease is evaluated because of chronic dyspnea, minimally productive cough, and limited exercise tolerance. He thinks his dyspnea on exertion has worsened. He stopped smoking cigarettes 8 years ago and is currently using an ipratropium inhaler four times per day and salmeterol discus twice per day. His body mass index, which 6 months ago was 21, is now 19. On physical examination, he is afebrile, his pulse rate is 94/min and regular, and respiration rate is 20/min. His breathing is unlabored at rest. He has signs of chest hyperinflation and decreased breath sounds without wheezing. He has no peripheral edema. The remainder of his examination is normal; results of a fecal occult blood test are negative. Baseline spirometry is unchanged. Forced expiratory volume in 1 sec (FEV1) 35% of predicted Forced vital capacity (FVC) 85% of predicted FEV1/FVC ratio50% PO2 62 mm Hg PCO2 45 mm Hg pH 7.38 (with the patient breathing room air) Chest radiograph reveals only hyperinflation. What is the best way to manage this patient’s weight loss? A. Provide dietary instructions to increase his caloric intake. B. Treat him with anabolic steroids. C. Refer him for pulmonary rehabilitation with exercise and nutritional counseling. D. Prescribe oxygen supplementation to improve his oxygen consumption. E. Add inhaled corticosteroids to his medical regimen.
- 19. 19 Pulmonary Medicine and Critical Care:Question 48 A 50-year-old man is evaluated in the emergency department because of fever, a nonproductive cough, and a 2-day history of myalgia and headache. He has also had some nausea and diarrhea. He is a heavy smoker. On physical examination, he is slightly disoriented. Temperature is 38.9 0C (102 0F), pulse rate is 110/min, respiration rate is 32/min. Chest radiograph shows fluffy infiltrates to the right upper and lower lobes. Results of laboratory testing show serum sodium of 128 meq/L, blood urea nitrogen of 42 mg/dL, serum creatinine of 2.2 mg/dL, and serum creatine kinase of 250 U/L. Which one of the following is best next step in the management of this patients pneumonia? A. Order direct fluorescent antibody testing of the sputum for Legionella B. Order serologic testing for Legionella C. Send a urine specimen for measurement of Legionella antigen D. Initiate empiric antibiotic therapy forLegionella Pulmonary Medicine and Critical Care:Question 49 A 28-year-old man, a suspected cocaine abuser, is found in a parking lot throwing himself against cars. En route to the hospital, he has a generalized tonic -clonic seizure that lasts approximately 3 minutes. His temperature is 38.8 C (101.8 F), pulse rate is 120/min, respiration rate is 18/min, and blood pressure is 170/98 mm Hg. He is agitated, diaphoretic, and voicing paranoid thoughts. Restraints are applied and intravenous access is obtained. Which one of the following should be initially administered to this patient? A. Labetalol B. Haloperidol C. Lorazepam D. Phenytoin E. Acetaminophen Pulmonary Medicine and Critical Care:Question 50 A 72-year-old man with chronic obstructive pulmonary disease is evaluated because he is planning a vacation in Hawaii and wants to ensure he can safely make the trip. He has a history of dyspnea when climbing more that one flight of stairs. On physical examination, his pulse rate is 76/min, respiration rate is 16/min, and blood pressure is 122/84mm Hg. He has mildly diminished breath sounds bilaterally, but otherwise the examination is unremarkable. There is no clubbing and no evidence of peripheral edema. Results of arterial blood gas measurements and spirometry (measured at ambient temperature with the patient breathing room air at a barometric pressure of 760 mm Hg) are as follows. PaO2 62 mm Hg PaCO2 40 mm Hg pH 7.40 What is the most appropriate recommendation for this patient? A. He should not travel by a commercial airline. B. He should be pretreated with carbonic anhydrase inhibitors before the flight. C. He should be pretreated with dexamethasone before the flight. D. He should use supplemental oxygen during the flight. E. The cabin pressure on commercial airlines is sufficient for this patients needs.
- 20. 20 Pulmonary Medicine and Critical Care:Question 51 A 37-year-old man with asthma is evaluated because he continues to have frequent attacks and now feels his short-acting β-agonist is not providing relief. He states he is using his medications, including a long-acting β-agonist inhaler, inhaled high-dose corticosteroids, and a short-acting β-agonist inhaler as rescue medication. He has symptoms daily and nocturnal symptoms about twice per week. On physical examination, he is in mild respiratory distress. He is afebrile. Pulse rate is 90/min and regular, respiration rate is 18/min, and blood pressure is 140/85 mm Hg. He has bilateral wheezing. Spirometry shows a forced expiratory volume in 1 sec (FEV1) 65% of predicted; it improves with bronchodilators to 85% of predicted. He has no history of recent viral upper respiratory infections or rhinitis or symptoms of gastroesophageal reflux disease. Which of the following is the best next step in this patients management? A. Add a leukotriene inhibitor. B. Switch to an oral β-agonist and have the patient return for a pill count. C. Observe the patient using the metered-dose inhaler. D. Initiate oral prednisone therapy and have the patient return for a pill count. E. Have the patient return with a symptom and treatment log. Pulmonary Medicine and Critical Care:Question 52 A 57-year-old woman with systemic lupus erythematosus is evaluated because the gradual onset of shortness of breath on exertion. She takes low-dose corticosteroids and nonsteroidal anti-inflammatory agents. Her current disease manifestations are primarily small-joint arthralgias and anemia. She has had no fever, chest pains, or cough. On physical examination, there is no peripheral edema or abnormal jugular venous distention. There are no crackles or rub on lung auscultation. Chest radiograph is normal except for low lung volumes and bibasilar platelike atelectasis. Pulmonary function testing shows: Forced expiratory volume in 1 sec (FEV1) 75% of predicted Forced vital capacity (FVC)73% of predicted FEV1/FVC 90% Total lung capacity 72% Residual volume 95% Diffusing lung capacity for carbon monoxide (DLco) 80% CT scan of the chest reveals symmetrical lower lobe volume loss without pulmonary infiltrates or fibrosis. Which of the following best characterizes this patients restrictive lung disease? A. Diffuse alveolar hemorrhage B. Small airways disease secondary to systemic lupus erythematosus C. Interstitial pneumonitis D. Respiratory muscle weakness
- 21. 21 Pulmonary Medicine and Critical Care:Question 53 A 32-year-old black man is evaluated because of a 4-month history of progressive dyspnea on exertion. On physical examination, the patient has elevated jugular venous pressure to the angle of the jaw with large V waves, a holosystolic murmur at the left lower sternal border, and an accentuated pulmonic valve component. The lungs are clear to auscultation. The abdomen is distended, with shifting dullness. The patient has 1+ peripheral edema. High-resolution CT scan reveals mosaic perfusion. Pulmonary function test results are listed below. Forced expiratory volume in 1 sec (FEV1) 2.06 L (84% of predicted) Forced vital capacity (FVC) 2.74 L (83% of predicted) FEV1/FVC 75% Forced expiratory flow (FEF 25%-75%) 1.58 L/sec (57% of predicted) Total lung capacity 4.01 L (76% of predicted) Functional residual capacity 2.13 L (72% of predicted) Residual volume 1.42 L (73% of predicted) Diffusing lung capacity for carbon monoxide (DLco) 4.30 mL/min per mm Hg (22% of predicted) Which of the following is the most likely cause of this patients dyspnea? A. Idiopathic pulmonary fibrosis B. Emphysema C. Chronic thromboembolic disease D. Congestive heart failure E. Cirrhosis Pulmonary Medicine and Critical Care:Question 54 A 61-year-old man is evaluated in the emergency department because of a 3-day history of cough productive of yellow sputum. He has a history of coronary artery disease, severe diabetes, and moderate emphysema. He routinely uses supplemental oxygen, 2 L/min. He states that he is more dyspneic than usual and is now short of breath even at rest. He reports no hemoptysis or chest pain. His oxygen saturation is 91% on 2 L supplemental oxygen; he is using accessory muscles of respiration and pursed-lipped breathing. Physical examination shows a prolonged expiratory-to-inspiratory phase on exhalation and a few scattered wheezes. He has tachycardia and bilateral pitting edema of the extremities. Chest radiograph shows changes consistent with emphysema but is otherwise unchanged from baseline. Complete blood count shows leukocytosis with a left shift. Two days ago, his arterial blood gas values were PaO2 70 mm Hg, PaCO248 mm Hg, and pH 7.37. Today, the values are PaO2 59 mm Hg, PaCO2 64 mm Hg, and pH 7.30. Which of the following is the best next step in this patients management? A. Prescribe oral prednisone, and instruct him to follow up with his primary physician in 1 to 2 weeks. B. Prescribe oral prednisone and an oral antibiotic, and instruct him to follow up with his primary physician in 1 to 2 weeks. C. Hospitalize him. D. Increase his supplemental oxygen to 3 L/min, prescribe oral prednisone and an oral antibiotic, and instruct him to follow up with his primary physician in 1 to 2 weeks. E. Reassure him that exacerbations are common in COPD, increase his supplemental oxygen to 3 L/min, and instruct him to follow up with his primary physician within 1 week.
- 22. 22 Pulmonary Medicine and Critical Care:Question 55 A 65-year-old man is evaluated because of a 2-year history of shortness of breath on exertion, fatigue of fairly recent onset, and weight loss. Symptoms have progressed to the point that he is dyspneic when engaged in the activities of daily living. He has had a dry cough for more than 1 year, but over the past 3 months, he has had a cough productive of yellow sputum with occasional streaks of blood. He has no fever or night sweats. He has a 20-pack-year history of cigarette smoking; he quit smoking more than 20 years ago. He is a retired surface miner. On physical examination, he is thin and appears chronically ill. He has fine inspiratory crackles and clubbing. Chest radiograph shows diffuse, small nodular densities with a 5-cm mass in the left upper lobe and a 3-cm mass with cavitation in the right upper lobe. Report of a chest radiograph taken 2 years ago describes bilateral nodular infiltrates but does not mention upper lobe masses. Which of the following would be the most appropriate next step in this patient’s management? A. Begin oral clindamycin. B. Schedule a positron emission tomography scan. C. Measure the serum rheumatoid factor level. D. Collect sputum for an acid-fast bacillus stain and culture. E. Schedule fiberoptic bronchoscopy. Pulmonary Medicine and Critical Care:Question 56 A 22-year-old previously healthy man is evaluated in the emergency department because of fever, productive cough, and shortness of breath. His temperature is 40 C (104 F), pulse is 120/min, respiration rate is 32/min, and blood pressure is 100/70 mm Hg. Measurement of arterial blood gases with the patient breathing room air shows PO2 of 55 mm Hg, PCO2 of 30 mm Hg, pH of 7.41. Chest radiograph reveals bilateral alveolar infiltrates with no effusions. Gram stain of the sputum reveals gram-positive diplococci. Which of the following is the most appropriate for this patient? A. Treat him as an outpatient with oral therapy. B. Treat him as an outpatient with intravenous therapy. C. Hospitalize him. D. Hospitalize the patient in the intensive care unit. Pulmonary Medicine and Critical Care:Question 57 A 52-year-old man is evaluated because of a 2-month history of nonproductive cough, myalgias, and low-grade fever. When his illness began, a chest radiograph showed bilateral alveolar infiltrates, and a presumptive diagnosis of community- acquired pneumonia was made. He was treated with oral azithromycin without effect, followed by a 10-day course of levofloxacin, also without effect. During the course of his illness he has lost 4.5 kg (10 Ib) without significant anorexia. He is a lifetime nonsmoker and works as an office manager. He has no pets and no unusual hobbies. On physical examination, his vitals signs are normal, except for a respiration rate of 20/min. He is in mild respiratory distress on exertion. On examination of the chest, bilateral crackles are audible, without wheezing. Chest radiograph shows bilateral alveolar infiltrates, which are changed in location from those seen on his original radiographs. Pulmonary function tests show forced expiratory volume in 1 sec (FEy1) 75% of predicted, forced vital capacity (FVC) 72% of predicted, total lung capacity 80% of predicted, and diffusing lung capacity for carbon monoxide (DLCO) 65% of predicted. Arterial blood gas values, with the patient breathing room air, are PO2 62 mm Hg, PCO 242 mm Hg, and pH 7.39.
- 23. 23 Which of the following is the most likely diagnosis? A. Hypersensitivity pneumonitis B. Cryptogenic organizing pneumonitis C. Resistant pneumococcal pneumonia D. Chlamydia pneumonia E. Bronchoalveolar cell carcinoma Pulmonary Medicine and Critical Care:Question 58 A 54-year-old man with known severe emphysema is evaluated because of a 6-week history of poor appetite, cough with intermittent production of blood-tinged sputum, and increased dyspnea on exertion. The patient has recently completed a 2-week course of oral antibiotics, but his symptoms have not abated. Recent pulmonary function testing shows severe obstructive lung disease with a forced expiratory volume in 1 sec (FEV1) of less than 20% of predicted on repeat studies. Chest radiograph shows a 2-cm left peripheral lung mass that was not present on a radiograph 18 months ago. CT scan of the chest confirms the mass and shows no evidence of mediastinal lymphadenopathy. Needle aspiration of the mass yields cells that show adenocarcinoma of the lung. Which one of the following statements is true in the consideration of this patient for lung transplantation? A. This patient should be referred immediately for lung transplantation. B. Lung transplantation may be considered if the tumor is removed by surgical wedge resection and no recurrence is observed after 2 years. C. The presence of cancer is an absolute contraindication to lung transplantation. D. This patient is too old to be considered for lung transplantation. Pulmonary Medicine and Critical Care:Question 59 A 68-year-old woman with hypertension, degenerative joint disease, and depression is hospitalized in the intensive care unit with altered mental status. No information about the patients medications is available. The patients temperature is 38.3 C (101 F), pulse rate is 118/min, respiration rate is 24/min, and blood pressure is 120/70 mm Hg. No focal neurologic abnormalities are noted, but she is obtunded. Her reflexes are normal. Electrocardiogram shows only sinus tachycardia with no acute changes, and chest radiograph shows bilateral interstitial infiltrates. Laboratory studies: Blood urea nitrogen 30 mg/dL Plasma glucose 65 mg/dL Serum sodium 148 meq/L Serum potassium 4.5 meq/L Serum chloride 108 meq/L Serum bicarbonate 18 meq/L Serum creatinine 1.6 mg/dL Serum osmolarity 302 mosm/L Which one of the following is the most likely toxin? A. Ephedrine B. Salicylate C. Ethylene glycol D. Lithium E. Acetaminophen
- 24. 24 Pulmonary Medicine and Critical Care:Question 60 A 68-year-old man with severe chronic obstructive pulmonary disease (forced expiratory volume in 1 sec 32% of predicted) is evaluated bec ause of severe dyspnea and the inability to carry out his activities of daily living. He is on maximal bronchodilator and oxygen therapy. Which of the following might pulmonary rehabilitation improve? A. Exercise tolerance B. Forced expiratory volume in 1 sec C. Oxygenation D. Survival Pulmonary Medicine and Critical Care:Question 61 A 40-year-old man is evaluated because of a positive tuberculin skin test after a pre- employment physical examination. There is a local reaction with induration measured at 22 mm. Chest radiograph is essentially normal. He is asymptomatic except for an occasional dry cough. He has no shortness of breath. Which of the following is the best next step in this patients management? A. Treatment for latent tuberculosis B. Sputum induction C. Isoniazid therapy for 9 months D. Rifampin and pyrazinamide therapy for 6 months E. CT scan of the chest Pulmonary Medicine and Critical Care:Question 62 A 46-year-old man is evaluated because of ankle edema and exertional dyspnea without angina. For several years, he has had fatigue, dysphagia with symptomatic gastroesophageal reflux, and pain with blanching in his fingers while shoveling snow. He takes a β-blocker for mild hypertension. On physical examination, he has perioral skin tightening, numerous telangiectasias on both sun-exposed and protected surfaces, and ‘sausage shaped” fingers without digital ulcerations. His lungs are clear. On cardiac examination, he has a right parasternal lift with a loud pulmonic valve component. The S2 does not split on inspiration. He has pitting edema to the mid-shin bilaterally and 8 cm of jugular venous distention while seated at 45 degrees from horizontal. Left vent ricular systolic and diastolic functions are normal on transthoracic echocardiogram. Both the right atrium and right ventricle are dilated with moderate tricuspid regurgitation. Pulmonary artery pressure is estimated to be 52 mm Hg by echocardiography. Which of the following statements is true about patients with these symptoms? A. Pulmonary hypertension is a frequent cause of death. B. Pulmonary hypertension indicates an overlap syndrome. C. Pulmonary hypertension occurs only in the setting of an assoc iated interstitial lung disease. D. Recurrent venous thromboembolism due to an associated hypercoagulable state is the usual cause of pulmonary hypertension. Pulmonary Medicine and Critical Care:Question 63 A 55-year-old man is evaluated in the emergency department because of an acute, severe asthma attack; he is hospitalized in the intensive care unit for aggressive medical therapy and monitoring. He is expectorating thick greenish sputum. His medical history includes hypertension, cholecystectomy, and glaucoma. Chest radiograph reveals hyperinflation only. Medical therapy in the emergency department included repeated doses of aerosolized albuterol and ipratropium, as well as methylprednisolone, 125mg administered intravenously.
- 25. 25 Peak expiratory flow rate is unimproved at 80 L/min. Which of the following is the most appropriate next step in this patient’s management? A. Nebulized ipratropium bromide administered by face mask B. Intravenous magnesium sulfate C. Broad-spectrum antibiotics targeting community-acquired respiratory pathogens D. Inhaled corticosteroids Pulmonary Medicine and Critical Care:Question 64 A 62-year-old woman with moderate emphysema is evaluated during a routine visit. She has chronic dyspnea on exertion but has no cough or sputum production. She uses supplemental oxygen, 2 L/min, when sleeping and on exertion. She currently uses albuterol and ipratropium four times per day, and salmeterol and theophylline twice per day. She is currently enrolled in a pulmonary rehabilitation program and is concerned about ‘catching a cold” from other people enrolled in the pulmonary rehabilitation program. What is the best advice for this patient? A. Take a daily antibiotic (long-term suppressive antibiotic therapy) to prevent pneumonia. B. Practice good hand washing, attempt to avoid close prolonged cont act with ill persons, and take pneumococcal and annual influenza vaccine. C. Avoid any social functions where there will be large crowds. D. Discontinue attendance at the pulmonary rehabilitation program. Pulmonary Medicine and Critical Care:Question 65 A 35-year-old man is evaluated because of a 2-week history of low-grade fevers, fatigue, cough, pleuritic chest pain, and increasing dyspnea on exertion. He is a construction worker and is having difficulty performing his usual tasks. He has a 10- pack-year history of cigarette smoking. On physical examination, he has right chest pain but no respiratory distress at rest. Temperature is 38.2 C (100.8 F), pulse rate is 112/min and regular, and respiration rate is 20/min. There is evidence of a right pleural effusion and no other abnormalities. Peripheral blood leukocyte count is 9,000/μL, with 80% neutrophils and 15% lymphocytes. Liver function test results are normal. Chest radiograph shows a moderate right pleural effusion with minimal contralateral shift and no parenchymal infiltrates. Thoracentesis yields minimally turbid yellow fluid with results as follows : Pleural fluid nucleated cell count 3000/1iL with 5% neutrophils, 85% lymphocytes, and 1% macrophages Pleural fluid total protein 5.2 g/dL Pleural fluid serum lactate dehydrogenase 230 U/L Pleural fluid glucose 80 mg/dL Pleural fluid pH 7.36 Pleural fluid Gram and acid-fast bacilli stains are negative. Tuberculin skin test is negative. Cytologic evaluation for malignant cells is negative. What is the most likely diagnosis? A. Tuberculous pleurisy B. Lung cancer C. Parapneumonic effusion D. Pulmonary embolism E. Benign asbestos pleural effusion
- 26. 26 Pulmonary Medicine and Critical Care:Question 66 A 72-year-old man is evaluated because of difficulty maintaining sleep once he goes to bed. He often awakens at around 2 AM. He reports no history of snoring, has no daytime symptoms, and has no difficulty initiating sleep. He has end-stage renal disease and undergoes outpatient dialysis three times per week. His medications include epoetin alfa, stress vitamins, lisinopril, and sertraline. On physical examination, blood pressure is 150/70 mm Hg. The pharynx is normal, chest is clear, and the heart is normal. There is no peripheral edema. Serum ferritin is 65 mg/dL. During a 5-hr sleep recording, the patient had 265 periodic limb movements, with 156 associated with arousal from sleep. One epoch from the patients sleep study is shown. Which of the following medications is most effective for the treatment of this patient’s sleep disorder? A. Clonazepam B. Pramipexole C. Oxycodone D. Gabapentin E. Ketorolac Pulmonary Medicine and Critical Care:Question 67 A 40-year-old woman, a nurse, is evaluated because of worsening asthma symptoms. She has had mild, intermittent asthma since college, for which she has been using an albuterol inhaler as needed, usually less than once a month. During the past 3 months, she has experienced cough, tightness of the chest, and wheezing, which improve after the use of inhaled albuterol. She uses the inhaler twice a day on average and has awakened at least twice a week with nocturnal cough. She works three consecutive 12-hour day shifts, and the cough is regularly worse at the end of each shift. During her days off, she has fewer asthma symptoms and feels significantly better by the time she returns to work. She has a history of allergic rhinitis that has also recently become more symptomatic. Approximately 6 months ago, she acquired a kitten that sleeps in the bedroom. She has lived in her home for 6 years, and it is carpeted and has heavy draperies. Chest examination is notable for good air entry. There are scattered end-expiratory wheezes. In addition to treatment with inhaled corticosteroids, which of the following interventions is most likely to benefit this patient?
- 27. 27 A. Treatment with an oral antihistamine B. Getting rid of the kitten C. Avoiding exposure to latex products D. Removing the carpets and draperies from her home E. Treatment with a leukotriene-modifying drug Pulmonary Medicine and Critical Care:Question 68 A 60-year-old woman is hospitalized for an exacerbation of chronic obstructive pulmonary disease. She is treated with ipratropium bromide by nebulizer every 4 hours; intravenous azithromycin, 500 mg/d; methylprednisolone, 125 mg intravenously every 6 hours; and oxygen by nasal cannula. During the first 2 hospital days, her condition remains unchanged. On hospital day 3, she develops increased dyspnea and a cough productive of sputum. On physical examination, she is awake and alert and in moderate respiratory distress. Her temperature is 36.7 C (98 F), pulse rate is 110/min, respiration rate is 20/min, and blood pressure is 150/90 mm Hg. Her lungs are hyperresonant to percussion, with accessory muscle use, poor air movement, mild wheezing, and no crackles. Chest radiograph demonstrates hyperinflation, with no other abnormalities. Leukocyte count is 16,000/μL. Arterial blood gas measurements, with the patient breathing 1.5 L oxygen, show PO2 of 55 mm Hg, PaCO2 of 55 mm Hg, and pH of 7.32. She is transferred to the intensive care unit for close observation and possible assisted ventilation. Which of the following is most appropriate additional management for this patient? A. Discontinue azithromycin and begin levofloxacin. B. Begin intravenous aminophylline. C. Increase methylprednisolone to 250 mg every 6 hours. D. Add albuterol to ipratropium bromide by nebulizer every 4 hours. E. Increase oxygen by nasal cannula to 3 L/min. Pulmonary Medicine and Critical Care:Question 69 A 22-year-old man is evaluated in the emergency department after being rescued from a house fire. The paramedics administered 100% oxygen by nonrebreather mask, and his oxygen saturation is 99% by pulse oximetry. Pulse rate is 115/min, respiration rate is 30/min, and blood pressure is 120/70 mm Hg. There is no stridor, no use of the accessory muscles of respiration, and the patient’s mental status is clear. There are mild facial burns as well as singed nasal hairs and soot in the posterior oropharynx. Lungs are clear with good air entry bilaterally. Which one of the following is most correct about this patient’s condition? A. The pressure of facial burns reliably predicts the presence of airway injury. B. Direct laryngoscopy or bronchoscopy should be performed for airway injury. C. This patient is at low risk for delayed 2 days postinhalation) injury to the lower airways. D. Dexamethasone should be empirically administered. Pulmonary Medicine and Critical Care:Question 70 A 19-year-old competitive female swimmer with no history of asthma is evaluated because of dyspnea and cough after any exercise, symptoms she has had since she was accidentally exposed to chlorine powder that was being added to a swimming pool in the university 6 weeks ago. Within hours of the exposure, she and several teammates noted burning of the eyes and mucous membranes, as well as briefly incapacitating chest tightness and cough. Physical examination shows no abnormalities, and results of chest radiograph and spirometry are also normal.
- 28. 28 Which of the following statements regarding this case is true? A. Spirometry is invariably abnormal. B. Inhaled corticosteroids and β-agonists are usually ineffective. C. Methacholine challenge testing is likely to show an abnormality. D. Symptoms generally resolve within 3 months of exposure. E. The patient must avoid further exposure to chlorinated water. Pulmonary Medicine and Critical Care:Question 71 A 23-year-old woman is evaluated in the emergency department because of generalized pruritic rash and difficulty breathing, both of which developed minutes after she ate at a nearby restaurant. The patient developed a rash some years ago after eating in a restaurant, but she is unsure whether she has food allergy. On physical examination, the patient is very anxious and in significant respiratory distress. Her temperature is 36.7 C (98 F), pulse rate is 120/min and regular, respiration rate is 30/min, and blood pressure is 85/50 mm Hg. Periorbital edema is present. Diffuse wheezing and prolonged expiratory phase are noted on auscultation. There is diffuse erythema over the trunk and extremities. The patient is promptly treated with subcutaneous epinephrine, intravenous fluids, inhaled β-agonist s, corticosteroids, and antihistamines. After 2 hours she feels better, her vital signs have returned to normal, and there is no wheezing on minimal prolongation of expiratory phase. Which of the following is the most appropriate next step in this patient’s management? A. Observe her in the emergency room for another hour, and discharge her if she remains stable. B. Discharge her and prescribe a tapering dose of corticosteroids for 1 week. C. Hospitalize her for further observation. D. Discharge her with an epinephrine and instructions to consult an allergist. Pulmonary Medicine and Critical Care:Question 72 A 74-year-old male nursing home resident with a history of mild dementia and chronic obstructive pulmonary disease is hospitalized bec ause of a 2-day history of upper respiratory symptoms and severe dyspnea. He is intubated and mechanical ventilation is begun. Therapy with intravenous corticosteroids, antibiotics, and bronchodilators is initiated. He soon becomes hypotensive and hypoxemic with rising peak airway pressures. Chest radiograph reveals a left-sided tension pneumothorax, and a chest tube is placed with immediate improvement in vital signs and oxygenation. Five minutes later, he becomes severely agitated, hypertensive, and diaphoretic, despite good oxygenation, acceptable airway pressures, and a functioning chest tube. Which one of the following is the best next step in this patients management? A. Vecuronium B. Fentanyl C. Midazolam D. Propofol E. Haloperidol
- 29. 29 Pulmonary Medicine and Critical Care:Question 73 A 60-year-old man with chronic obstructive pulmonary disease is evaluated because of persistent cough and sputum production. He reports no fevers or weight loss. He has had increased sputum production over the past 6 to 9 months and moderately severe reduction in forced expiratory volume in 1 sec (FEV1 55% of predicted). His symptoms have been unresponsive to antibiotics. He has an 80-pack-year history of cigarette smoking. Chest radiograph reveals multiple small nodules in the left upper lung zone without infiltrate. Serologic testing for HIV is negative. Sputum cultures are negative for bacteria. A test for acid-fast bacillus is negative, but culture grows Mycobacterium avium-intracellulare with 1+ growth. Which of the following is the best next step in this patients management? A. Treat him for Mycobacterium avium-intracellulare without further testing. B. Perform bronchoscopy with bronchioalveolar lavage and transbronchial biopsy. C. Order a HRCT scan of the chest. D. Order a sputum culture for Mycobacterium avium-intracellulare. Pulmonary Medicine and Critical Care:Question 74 A 21-year-old man presents with a 4-hour history of cough and dyspnea after spending the day moving stored hay. A college student, he lives with his parents and two younger siblings on the dairy farm where he was born and raised. No one else in the family has similar symptoms. He actively participates in small grain production, soybean grinding for animal feed, and the cutting, baling, and storage of hay. He has had similar episodes the past two summers; each time he was hospitalized for atypical pneumonia, and his symptoms resolved quickly with antibiotics and inhaled bronchodilators. On physical examination, his temperature is 38.4 C (101 .1 F), respiration rate is 22/min, and blood pressure is 142/84 mm Hg. He has a few bibasilar crackles. There is no jugular venous distention or peripheral edema. Chest radiograph reveals patchy infiltrates in the lower lobes and right middle lobe interpreted by the radiologist as compatible with bronchopneumonia. Complete blood count shows a leukocyte count of 14,500/μL with 11,400 polymorphonuclear cells, 200 band forms, and 150 eosinophils. What additional information would most strongly support the diagnosis? A. A precipitin band toThermoactinomyces sacchari on a farmers lung panel B. Immediate skin test reactivity to ‘mold’ extract C. Improvement with observation alone and recurrence of symptoms after returning to the farm D. Bedside spirometry demonstrating reversible airflow obstruction after bronchodilator administration Pulmonary Medicine and Critical Care:Question 75 A 50-year-old woman is evaluated on a winter morning because of a 1-week history of daily headaches with some nausea and flu-like symptoms. Other people in her house have had similar headaches. She typically awakens with a headache but feels better after going to work without any specific therapy. The headache recurs several hours after she arrives home. She is a nonsmoker. Her vital signs, physical examination, leukocyte count, and hemoglobin are normal. Which of the following tests is most likely to help make the diagnosis? A. Pulse oximetry B. Lactate level C. Electrocardiogram D. Carboxyhemoglobin level
- 30. 30 Pulmonary Medicine and Critical Care:Question 76 A 56-year-old construction worker, a heavy smoker, sustains severe trauma to his left chest. Chest pain is severe for several minutes but subsides over the next hour. Because the chest pain does not resolve completely, he is evaluated in the emergency department 2 hours later, where results of a chest radiograph and complete blood count with differential are normal. The next day, he leaves on a week-long vacation to South America. During that time, he has intermittent chest discomfort and gradually increasing dyspnea with exertion. Upon returning home, he sees his physician because of dyspnea. Chest radiograph shows a large left-sided pleural effusion with minimal contralateral shift. At thoracentesis, 500 cc of brownish-colored fluid is removed and analyzed with the following results. Pleural fluid nucleated cell count 4000/mL with 10% neutrophils, 30% lymphocytes, 15% macrophages, and 45% eosinophils Pleural fluid hematocrit 10% Pleural fluid total protein 4 g/dL Pleural fluid serum lactate dehydrogenase 200 UIL Pleural fluid glucose 80 mg/dL Pleural fluid pH 7.35 Cytology test results are negative. Pain medication is prescribed for the patient. When he returns 14 days later, complete blood count shows a leukocyte count of 9000/μL with 20% eosinophils and chest radiograph shows that the pleural effusion has decreased substantially. Which of the following is the most likely diagnosis? A. Benign asbestos pleural effusion B. Paragonimiasis C. Post-traumatic hemothorax D. Lung cancer E. Pulmonary infarction Pulmonary Medicine and Critical Care:Question 77 A 60-year-old man with a history of severe chronic obstructive pulmonary disease is evaluated in the emergency department because of an exacerbation of his illness characterized by increasing shortness of breath over the past 2 days. He has a 90- pack-year history of cigarette smoking (he stopped smoking 6 months ago) and dyspnea on exertion, with exercise tolerance of one-half block. He uses home oxygen. His baseline forced expiratory volume in 1 sec (FEV1) is 0.80 Land forced vital capacity (FVC) is 2.4 L. He has a cough productive of minimal clear sputum. On physical examination, his temperature is 38.3 C (101.0 F), pulse rate is 110/min, and respiratory rate is 30/min. He is alert and anxious, using accessory muscles; he has decreased breath sounds bilaterally and wheezing with a prolonged expiratory phase. Laboratory studies: Leukocyte count 1 0,200/μL Serum creatinine 1.3 mg/dL Blood urea nitrogen 30 mg/dL Serum bicarbonate 32 meq/L Arterial blood gases (with the patient breathing room air) PaO2 54 mm Hg PaCO2 56 mm Hg pH 7.29 Chest radiograph shows no pulmonary infiltrate. Despite treatment with albuterol and ipratropium by nebulizer, the patient remains dyspneic.
- 31. 31 Which of the following is the best next step in this patients management? A. Increase oxygen concentration and continue albuterol/ipratropium treatment. B. Start noninvasive positive-pressure ventilation. C. Start continuous positive-airway pressure ventilation. D. Start intravenous antibiotic therapy. Pulmonary Medicine and Critical Care:Question 78 A 47-year-old man is evaluated in the emergency department because of fatigue and headaches, which are more frequent in the morning. He also notes nocturia and night sweats. On physical examination, his body mass index is 42. His heart and lungs are normal. Laboratory studies yield normal results except hemoglobin of 16.8 g/dL. Trace edema of the lower extremities is noted. Chest radiograph shows that his heart is of normal size and that his lung fields are clear. Which of the following is most likely to show the cause of the fatigue and headaches? A. Echocardiogram B. Spirometry C. Beck Depression Inventory D. CT scan of the brain E. Overnight polysomnography Pulmonary Medicine and Critical Care:Question 79 A 28-year-old man with a diffuse petechial rash is hospitalized in the intensive care unit with a clinical diagnosis of meningococcemia and septic shock. He was intubated in the emergency department for airway protection. Results of a lumbar puncture are compatible with bacterial meningitis. Intravenous penicillin is initiated. Chest radiograph shows no abnormality. On physical examination, his temperature is 39 C (102.2 F) and pulse rate is 120/min. An arterial line is inserted, and mean arterial pressure is 68 mm Hg with administration of intravenous norepinephrine. He is sedated and mechanically ventilated. Pulse oximetry is 100% with fractional inspired oxygen (FiO 2 set at .5, and positive end-expiratory pressure of 5 cm H20. Since his arrival in the emergency department 6 hours ago he has received 3 L normal saline. His urine output has decreased and is currently .25 mL/kg per hour over last 2 hours. Leukocyte count is 22,000/μL and platelet count is 40,000/μL (platelet count was 60,00/μL at the time of the lumbar puncture). Which of the following therapeutic decisions is most appropriate at this time? A. Transfuse platelets. B. Increase norepinephrine to achieve a mean arterial pressure of 75 mm Hg or higher. C. Switch from norepinephrine to dopamine. D. Administer a 1000-mL bolus normal saline. E. Administer furosemide. Pulmonary Medicine and Critical Care:Question 80 A 55-year-old man is evaluated in the emergency department because of a 5-day history of increased dyspnea and cough productive of yellow-green mucus. Nine months ago, he required prolonged mechanical ventilation for an exacerbation of chronic obstructive pulmonary disease. His medical history includes hypertension. On recent pulmonary function testing, the forced expiratory volume in 1 sec (FEV1) was 38% of predicted. His temperature is 38.1 C (100.5 F), pulse rate is 135/min and irregular, respiration rate is 25/min, and blood pressure is 90/65 mm Hg. He is mildly lethargic but arousable and oriented. He has a weak cough with pooling of
- 32. 32 secretions in the oral cavity and hypopharynx. Electrocardiogram demonstrates multifocal atrial tachycardia. Chest examination reveals accessory muscle use, coarse rhonchi, and decreased breath sounds at the right base. Leukocyte count is 1 7,000/μL. Chest radiograph shows right lower lobe consolidation. With the patient breathing 4 L oxygen, arterial blood gases show a FO2 of 50 mm Hg, a PCO2 of 65 mm Hg, and a pH of 7.25. Therapy with methylprednisolone sodium succinate, 125mg intravenously every 6 h, is intiated, along with nebulized albuterol and ipratropium bromide every 4 h, and azithromycin, 500 mg administered intravenously daily. Which of the following is the most appropriate additional management? A. Intubate and begin mechanical ventilation. B. Initiate mucloytic therapy, chest physiotherapy, and oral-tracheal suctioning. C. Administer a helium-oxygen mixture of 70%:30%, delivered by face mask. D. Initiate bilevel noninvasive positive-pressure ventilation by face mask E. Administer 40% oxygen by Venturi mask Pulmonary Medicine and Critical Care:Question 81 A 70-year-old man is ready to be discharged in October from the hospital after treatment of an exacerbation of his chronic obstructive pulmonary disease. His only other medical problems include stable angina and hypertension. He has normal renal function and is well nourished. He quit smoking 2 years ago. He received pneumonia vaccine 2 years ago and influenza vaccine 1 year ago. Which of the following is true of his vaccination status? A. He should receive pneumonia vaccine and influenza vaccine. B. He should receive pneumonia vaccine. C. He should receive influenza vaccine. D. He should receive neither pneumonia vaccine nor influenza vaccine. Pulmonary Medicine and Critical Care:Question 82 A 25-year-old man is evaluated approximately 12 hours after a suicide attempt in which he ingested 30 pills of an extra-strength acetaminophen product (500 mg/pill), 10 ibuprofen tablets (200 mg), and 7 pills of alprazolam (dosage unknown). He is sleepy but arousable and oriented. He has nausea and vomiting. His temperature is 37 C (98.6 F), pulse rate is 90/min, respiration rate is 16/min, and blood pressure is 120/76 mm Hg. In addition to obtaining an acetaminophen level, which of the following is the most important initial intervention? A. Administer oral N-acetylcysteine. B. Administer oral activated charcoal. C. Administer intravenous naloxone. D. Administer intravenous flumazenil. Pulmonary Medicine and Critical Care:Question 83 A 53-year-old woman with myasthenia gravis is hospitalized because of a 3-day history of progressive dyspnea. She ran out of her medications 5 days ago. On admission she is breathing shallowly and having difficulty speaking. She has mild weakness of the extremities. Her lungs and heart are normal. A chest radiograph is normal. Bedside testing shows a vital capacity of 1.5 L (34% of predicted) and a maximum negative inspiratory pressure of 60 cm H2O. Prednisone and pyridostigmine therapy is initiated. Over the next 24 hours, the weakness in the extremities is unchanged. The patient is noted to be having difficulty managing secretions and aspirates them on one occasion. What is the best next step in this patient’s management?
- 33. 33 A. Administer noninvasive ventilation through a nasal mask. B. Order chest physical therapy with postural drainage. C. Initiate orotracheal intubation. D. Order that she take nothing by mouth and administer medications intravenously. Pulmonary Medicine and Critical Care:Question 84 A thin, 19-year-old woman is evaluated because of chronic cough productive of green sputum. She reports a long-standing history of loose bowel movements and intermittent abdominal bloating. Physical examination is notable for bilateral nasal polyps, crackles in the upper lung zones bilaterally, and early digital clubbing. Which of the following is the best initial test to evaluate this patient for cystic fibrosis? A. Gene mutation test (buccal swab or blood test) B. Quantitative pilocarpine iontophoresis sweat chloride test C. 72-hour fecal fat test D. Measurement of nasal potential difference E. Sputum culture Pulmonary Medicine and Critical Care:Question 85 A 34-year-old man is evaluated because of recurrent sleepiness in the late afternoon, especially at work. His excessive sleepiness dates back to his high school years and seems unrelated to activity or schedule. He has no history of snoring or witnessed apneas, but he does awaken frequently at night, especially in the early morning. He reports that he has recurrent jaw weakness after laughing at a joke or becoming angry. Particularly troubling to the patient are recurrent nightmares occurring shortly after he falls asleep. On physical examination, the patient is 178 cm (70 in) tall and weighs 70.3 kg (155 Ib). His blood pressure is 120/75 mm Hg. His lungs are clear on auscultation; heart sounds are regular and there are no gallops or murmurs. Neurologic examination reveals no abnormalities. An overnight polysomnogram reveals no evidence of obstructive sleep apnea. On a multiple sleep latency nap test, mean sleep latency is 3.5 mm, and two sleep-onset periods of rapid eye movement are observed. Which of the following is the most likely diagnosis? A. Temporal lobe epilepsy B. Panic disorder C. Narcolepsy D. Amphetamine abuse E. Parasomnia Pulmonary Medicine and Critical Care:Question 86 A 48-year-old previously healthy man has a CT scan of the thorax with intravenous contrast. After administration of the contrast material the patient feels tightness in the throat and diffuse itching. He also feels light-headed. On physical examination, he is diaphoretic and anxious. His pulse rate is 125/min, his respiration rate is 28/min, and his blood pressure is 70/50 mm Hg. There is mild wheezing on auscultation. A rash is noted on the patient’s chest and upper extremities. Which one of the following is the most important immediate treatment? A. Dobutamine B. Dopamine C. Corticosteroids D. Epinephrine
- 34. 34 Pulmonary Medicine and Critical Care:Question 87 A 65-year-old hospitalized man, develops a rapidly progressing bilateral bronchopneumonia requiring mechanical ventilation. His fractional inspired oxygen level (nO2) is 0.6, and positive end-expiratory pressure is 12 cm H2O. He was agitated before being intubated and is now being treated with sedative agents. During the past 12 hours, he has also developed a moderate increase in creatinine concentration with normal urine output. His hemodynamic status has remained stable. Prothrombin time and partial thromboplastin time are mildly elevated. Platelet count is mildly depressed, and his leukocyte count is elevated. His blood pressure is normal. In addition to the proper antibiotics, which of the following is likely to benefit this patient? A. Antithrombin III B. A single large dose of methylprednisolone C. Low-dose (stress dose) corticosteroids D. Drotrecogin alfa (activated) E. Low-dose dopamine (2 μg/kg of body weight/mm) Pulmonary Medicine and Critical Care:Question 88 A 23-year-old woman is evaluated in the emergency department because of right- sided hemiplegia and depressed mental status. Her temperature is 39.2 C (102.5 F). Laboratory studies show a platelet count of 22,000/μL, serum creatinine of 2.5 mg/dL, serum lactate dehydrogenase of 458 U/L, hemoglobin of 8.3 g/dL, normal coagulation parameters, and schistocytes on her peripheral blood smear. She is intubated and mechanical ventilation is begun. Plasmapheresis is initiated for thrombotic thrombocytopenic purpura. Her condition improves, and after 8 days she c an follow simple commands and is extubated. Three hours later she seizes and becomes hypoxemic and is reintubated. Chest radiograph shows diffuse infiltrates consistent with neurogenic pulmonary edema or acute respiratory distress syndrome. She is severely agitated and lorazepam, 4 mg/hr, is begun. Ten days later, the thrombotic thrombocytopenic purpura is in remission and her respiratory status has improved, but she cannot be weaned because she remains unresponsive 2 days after stopping the lorazepam. A CT scan of the brain is unremarkable. Electroencephalogram shows “diffuse slowing.” Which of the following is the best next step in this patient’s management? A. Lumbar puncture B. Resume plasmapheresis C. Perform a tracheostomy and place a percutaneous gastrostomy tube D. Monitor the patient off sedatives and wait for her mental status to improve E. Measure serum levels of propylene glycol Pulmonary Medicine and Critical Care:Question 89 A 60-year-old man, a farmer, is evaluated because of severe, progressive shortness of breath and cough, such that he is no longer able to work. He has no history of cardiac or pulmonary disease but states that approximately 6 weeks ago he experienced self-limited chest tightness, wheezing, and cough that began a few hours after he checked the silage level in his silo. He “took it easy” for a couple of days and then felt well enough to return to work. He was well until 2 weeks ago when his presenting symptoms began. On physical examination, he has tachypnea and early inspiratory crackles. Chest radiograph shows only hyperinflation. Spirometry is notable for severe obstruction, with forced expiratory volume in 1 sec (FEV1) 35% of predicted, forced vital capacity
- 35. 35 (FVC) 90% of predicted, and FEV1/FVC 45% of predicted. What is the most likely cause of this patient’s symptoms? A. Hypersensitivity pneumonitis B. Bronchiolitis obliterans C. Occupational asthma D. Reactive airways dysfunction syndrome E. Acute respiratory distress syndrome Pulmonary Medicine and Critical Care:Question 90 A 66-year-old woman of normal body weight is evaluated in the emergency department because of weakness. She has diabetes mellitus and hypertension and 1 week ago underwent cholecystectomy. On physical examination, she weighs 55 kg (121.3 Ib). Her temperature is 38.1 C (100.5 F), pulse rate is 128/min, respiration rate is 28/min, and blood pressure is 80/60 mm Hg. Her abdomen is tender and bowel sounds are present. She has no chest pain but says she is dyspneic. Pulse oximetry is 88%, with the patient breathing room air. Supplemental oxygen is initiated. Electrocardiogram reveals T -wave inversion laterally. Hemoglobin is 13.5 g/dL. The patient remains hypotensive after 1 L of normal saline is infused, with worsening oxygenation. Which of the following diagnostic studies is most appropriate at this time? A. CT scan of the abdomen and chest B. Ventilation/perfusion lung scan C. Transthoracic echocardiography D. Transesophageal echocardiography Pulmonary Medicine and Critical Care:Question 91 A 64-year-old man who was diagnosed with amyotrophic lateral sclerosis 2 years ago is evaluated because of weakness in the legs that prevents him from standing and walking. He also reports that dyspnea forces him to sleep on his side. He has had no problems swallowing. On physical examination, he has significant wasting of the thenar and hypothenar eminences and weakness of the hands. His cranial nerve function is intact. His vital capacity is 40% of predicted and negative inspiratory pressure is -45 cm H20. Peak cough expiratory flow is 400 L/min. Which of the following interventions has been shown to prolong life in patients like this one? A. Prophylactic use of antibiotics to prevent pneumonia B. Daily home chest percussion therapy and postural drainage C. Nocturnal noninvasive ventilation through a face mask D. Daily mucolytic therapy Pulmonary Medicine and Critical Care:Question 92 A 68-year-old Lithuanian man with limited command of English presents for an initial outpatient visit. A letter from a doctor in another city indicates that the man has advanced idiopathic pulmonary fibrosis confirmed by surgical lung biopsy. Lung disease has progressed over 2 years despite an extended trial of prednisone and cyclophosphamide. Three months ago, pulmonary function studies showed a forced vital capacity (FVC) 59% of predicted. A sample of arterial blood obtained at that time showed a PCO2 of 49 mm Hg and a PO2 of 51 mm Hg, with the patient breathing room air. The office nurse reports that the man arrived in a wheelchair and has obvious peripheral edema. The patients daughter privately asks the physician to take on the