Understanding rickets types,diagnosis,prevention & treatment dr.sandeep c agrawal agrasen hospital gondia india
•
79 likes•4,715 views

CALCIUM,VITAMIN D,OSTEOPOROSIS,DIET, METABOLIC BONE DISEASE,HYPERPARATHYROIDISM,RENALOSTEODYSTROPHY,RICKETS,BONEMETABOLISM,Vitamin D Resistant Rickets Type 1 & 2,Fanconi anemia,Renal tubular acidosis,Familial Hypophosphatemia Rickets,Renal Rickets,Hepatic Rickets,Malabsorption Rickets,Hypophosphatasia,Malabsorption Rickets,Metaphyseal Dysplasia,Serum Calcium,Serum Phosphorus,Serum Vitamin D,Serum 1,25 dihydroxry cholecalcirol,Urine pH,Urine Calcium,Urine Creatinine,Understanding Rickets-Types,Diagnosis,Prevention & Treatment Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Understanding rickets types,diagnosis,prevention & treatment dr.sandeep c agrawal agrasen hospital gondia india
Similar to Understanding rickets types,diagnosis,prevention & treatment dr.sandeep c agrawal agrasen hospital gondia india (20)
More from AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA
More from AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA (13)
Recently uploaded
Recently uploaded (20)
Understanding rickets types,diagnosis,prevention & treatment dr.sandeep c agrawal agrasen hospital gondia india
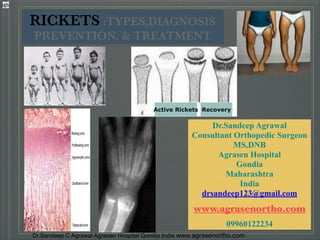
- 1. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Dr.Sandeep Agrawal Consultant Orthopedic Surgeon MS,DNB Agrasen Hospital Gondia Maharashtra India drsandeep123@gmail.com ! www.agrasenortho.com ! 09960122234 RICKETS :TYPES,DIAGNOSIS PREVENTION, & TREATMENT Active Rickets Recovery
- 2. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Rickets (Rachitis) Metabolic disease of growing bone that is unique to children (especially of first 2 years) and adolescents. .Caused by failure of osteoid to calcify in growing bones.
- 3. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 4. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Growth plate in normal bone shows: Zone of resting cartilage (one layer of cells). ! Zone of proliferating cartilage: Regular columns of cells originating from resting layer).
- 5. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Growth plate : Zone of degeneration : (cells become swollen with glycogen, glycolytic enzymes and alkaline phosphatase. Calcium is deposited in the matrix. It is sharply demarcated in X ray film). ! Zone of ossification : ! (Blood vessels invade the developing bone with ossification and remodeling resulting in mature bone).
- 6. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com In rickets Zone of proliferation: increases & becomes very vascular causing enlargement of metaphyseal area and invades adjacent zone of degeneration. ! Zone of degeneration: Fails to mineralise & newly formed tissue called osteoid is excessively deposited and being soft it gives way with pressure causing bulging and deformity of metaphyseal area of long bones ! (this is responsible for flaring of the ends of long bones and rachitic rosary).
- 7. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Types of Rickets 1.Nutritional Rickets or 2.Vitamin D-deficiency Rickets 3.Vitamin D-dependent Rickets Type I Type II 4.Vitamin D-resistant Rickets (“looks like Rickets”) 5.Secondary Rickets
- 8. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com 8 Rickets
- 9. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com PATHOGENESIS Causes of vitamin D deficiency 1. Disorders associated with Vitamin D synthesis Deficiency in cutaneously synthesized vitamin D Lack of dietary intake ! 2. Disorders associated with Vitamin D absorbtion ! 3. Chronic diseases of Liver or Kidney ! 4. Congenital anomalies of metabolism of Vitamin D, Ca, P.
- 10. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Deficiency in cutaneously synthesized vitamin D ! Cancer ???
- 11. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Congenital anomalies of metabolism of Vitamin D, Ca and P 1.Vit D-dependent rickets type 1 ! (pseudovitamin D-deficiency rickets) - defect in gene coding of renal 1-alpha-hydroxylase. ! ! 2.Vit D-dependent rickets type 2 ! (hereditary 1-alfa, 25-dihydroxyvitamin D-resistent rickets) - mutation exists in the vitamin D receptors (VDR). ! 3.Vit D-resistent rickets (Familial hypophosphatemic rickets) - ! mutations of the phosphate-regulating gene on the X chromosome
- 12. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com RENAL LOSSES X-linked hypophosphatemic rickets[*] Autosomal dominant hypophosphatemic rickets[*] Hereditary hypophosphatemic rickets with hypercalciuria! Overproduction of phosphatonin! Tumor-induced rickets[*] McCune-Albright syndrome[*] Epidermal nevus syndrome[*] Neurofibromatosis[*] Fanconi syndrome Dent disease DISTAL RENAL TUBULAR ACIDOSIS
- 13. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com PHOSPHOROUS DEFICIENCY INADEQUATE INTAKE: -rare ,severe anorexia -long-term use of aluminum- containing antacids ! ! PHOSPHATONIN: decreases renal tubular reabsorption of phosphate and therefore decreases serum phosphorus.
- 14. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com CLINICAL MANIFESTATIONS I. Specific to the bone tissue in rickets: ! A.osteomalacia B.Hyperplasia of osteoid tissue C.Hypoplasia of osseous tissue ! ! II. Not specific to the bone tissue in rickets
- 15. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Symptoms Specific to bone tissue Symptoms of osteomalacia : ! 1.Craniotabes ! 2.Softening of ribs ! 3.Kyphosis ! 4.Bowing in the legs ! 5.Softening of the big fontanel's edges
- 16. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Symptoms Specific to bone tissue Hyperplasia of osteoid tissue: ! 1.Increase of frontal and occipital tubers (frontal bossing, “caput quadratum”) ! ! 2.Costohondral prominence ("rachitic rosary”) ! 3.Chest deformities: (Harrison’s groove and pigeon breast)
- 17. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Symptoms Specific to bone tissue Hypoplasia of osseous tissue: ! Delayed fontanel closure ! Delayed teething ! Enamel hypoplasia ! Costal or Lower extremity fractures (particularly greenstick fractures) ! Lag of growth of tubular bones in length (in severe cases)
- 18. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Symptoms NOT Specific to bone tissue in rickets: Occipital alopecia ! Muscular hypotonia ! Constipation ! Hypocalcemic convulsions ! Anemia ! Increased risk for respiratory infections ! Growth retardation and low height−for−age (rachitic dwarfism)
- 19. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com BREAST-FED INFANTS: Low Vitamin D Content of Breast Milk, so infant rely on Cutaneous Synthesis or Vitamin Supplements.
- 20. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com In acute course of rickets symptoms of osteomalacia prevail In subacute – symptoms of hyperplasia of osteoid tissue. ! Initial period is starting from 2-3 month of life, lasts from 2-3 weeks to 2-3 months. In breast-fed infants whose mothers have osteomalacia, rickets may develop before 2 months. ! Florid rickets appears toward the end of the 1st and during the 2nd year of life. ! Later in childhood, manifest vitamin D deficient rickets is rare.
- 21. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com In rickets In the shaft: bone is resorbed and new osteoid is formed around the shaft from the periosteum ! During healing of rickets: a new line of calcified bone (line of provisional calcification) appears at the end of zone of degeneration out standing from rarefied osteoid then the area between it and the diaphysis gradually fills with normal density bone.
- 22. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 23. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com 1.Craniotabes: Occurs due to thinning of the inner table of occipital bone under the pressure of intracranial contents with failure of mineralization. ! It can be elicited by gentle pressure by both thumbs of the occipital bone, which produces a dent with crackling sensation (ping pong ball like). ! This can be elicited from 3 to 12 months of life.
- 24. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Clinical manifestation Early rickets 2. Rosary: Enlargement of costochondral junction of ribs giving the appearance of beads due to excessive osteoid formation. ! 3. Radiological finding of active rickets ! 4. Rise of serum alkaline phosphatase enzyme.
- 25. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Advanced rickets Head: Bossing of skull: excessive proliferation of cartilage at occipital and parietal eminences makes the skull looks like a box. ! Enlargement of head circumference. ! Delayed closure of anterior fontanels, which remains widely open ! Delayed eruption of primary dentition with possible enamel hypoplasia
- 26. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Thorax: Rosary beads. ! Longitudinal sulcus: appears lateral to the rosaries due to compression of rib cage by atmospheric pressure at weakest point. ! Harrison's sulcus: A transverse sulcus along the lower border of the costal margin due to inward traction of the ribs at sites of diaphragmatic insertion. Advanced rickets
- 27. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Rickets Characteristic feature: ! Widening of wrist, knee and ankle due to physeal over growth
- 28. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Thorax: ! Forward protrusion of sternum and adjacent costal cartilage. ! Everted costal margin below Harrison's sulcus. ! The overall shape of the chest wall is called “pigeon chest”, which is nearly triangular in cross section. Advanced rickets
- 29. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Abdomen: Liver and spleen become palpable as deformed chest and weak abdominal muscles ! Abdomen appears protruded. ! Pelvis: Pelvic inlet is narrowed by forward protrusion of sacral promontory, while pelvic outlet is narrowed by forward projection of the coccyx. ! This might be very hazardous in females during labor in the future. Advanced rickets
- 30. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Spinal column: ! Correctable kyphosis in the dorsal region and lordosis in the lumbar region due to muscle weakness and laxity of ligaments. Advanced rickets Scoliosis
- 31. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 32. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Complications Respiratory: infections or atelectasis due to chest deformities. ! GIT: diarrhea or constipation. ! Bony deformities or fractures. ! Anemia: due to chronic infection or deficiencies. ! Tetany: due to hypocalcaemia in late cases after exhaustion of parathyroids.
- 33. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Rickets leads to cupping and to a brush−like appearance of the epiphyseal ends on radiograms. ! Radiographs of the knee of a 3.6-year-old girl with hypophosphatemia depict severe fraying of the metaphysis. N Active Rickets recovery
- 34. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Rickets in wrist - uncalcified lower ends of bones are porous, ragged, and saucer-shaped (A) Rickets in 3 month old infant (B) Healing after 28 days of treatment (C) After 41 days of treatment A B C
- 35. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Radiologic Changes Active rickets: They occur early, are pathognomonic and diagnostic, and help in follow up. Distal ends of long bones appear flared, frayed and cupped. ! Distance between the distal end of radius and metacarpal bones appears wider than normal (by the area filled with osteoid). ! Diaphysis appears rarefied and may show double contour or deformity.
- 36. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Radiologic Changes Healing rickets: Occurs 2-3 weeks after successful treatment. Appearance of the line of provisional calcification at the end of metaphysis, then the osteoid in between this line and diaphysis gradually ossifies.
- 37. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Radiologic Changes Healed rickets: Bone density returns to normal with slight cupping remains as a stigma of previous rickets.
- 38. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 39. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com RADIOLOGICAL FINDINGS
- 40. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com RADIOLOGICAL FINDINGS ◆ Rosary beads of rickets ! ! ! ! ! ! ! ◆ curved back
- 41. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Biochemical parameters: Serum alkaline phosphatase is elevated due to over activity of osteoblasts during the formation of excessive osteoid (normal 5-15 Bodansky units /dl). ! Serum inorganic phosphorus is decreased (normal 4.5-6.5 mg/dl). ! Serum calcium is maintained within normal values (9-11 mg/dl) due to compensatory hyperactivity of parathyroid gland. ! Vitamin D and its metabolites are decreased.
- 42. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com 42 Rickets
- 43. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 44. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com 1. Low dosage and long−term vitamin D therapy (gradual method) 1000− 10 000 IU/day (125-250 mcg) for 2−3 months Vitamin D can be given according to the infant’s age as follows: 1000 IU/day for infants < 1 month of age, 1000-5000 IU/ day for children 1-12 mon. 5000-10 000 IU/day for children > 12 mon. If hypocalcemia is seen the initial dose of vit D must be doubled. Afterwards, it is recommended to give maintenance therapy of 400 IU/ day.
- 45. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Because this method requires daily treatment, success depends on compliance. Levels of Ca and P are normalized in 6−10 days by this therapy, while it takes 1−2 months for PTH to reach normal levels. Depending on the severity of the disease, it may take 3 months for the normal serum ALP levels to be restored and the radiological findings of rickets to disappear. ! In this treatment model, lack of compliance is an important cause of lack of response
- 46. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com STOSS THERAPY 300,000–600,000 IU of Vitamin D Are Administered Orally or Intramuscularly As 2–4 Doses Over 1 Day. ! Stoss Therapy Is Ideal in Situations Where Adherence to Therapy Is Questionable.
- 47. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 48. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com 2. Stoss therapy (single-day therapy) For patients who are suspected to have poor compliance, a high dose of vitamin D can be given orally or intramuscularly as a single dose of 100 000−600 000 IU after the first month of life. ! This dose is usually divided into 4 or 6 oral doses. ! An intramuscular injection is also available.
- 49. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Stoss therapy (single-day therapy) Administration of 150 000−300 000 units of vitamin D and 600 000 units (15,000 mcg) in severe rickets is an effective and safe method of treatment. ! Vitamin D (cholecalciferol) is well stored in the body and is gradually released over many weeks. ! This treatment evokes a rapid clinical response, resulting in biochemical recovery in a few days and radiological recovery in 10−15 days.
- 50. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 51. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Single-day therapy avoids problems with compliance and may be helpful in differentiating nutritional rickets from familial hypophosphatemia rickets (FHR). ! In nutritional rickets, the phosphorus level rises in 96 hours and radiographic healing is visible in 6-7 days. ! Neither happens with FHR.
- 52. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Vit D deficiency rickets – 1 alpha vit D3 or vit D2(arachitol) 6,00,000 IU every two to three weeks IM 2 to 3 doses. (STOSS REGIMEN) ! VDDR 1 –! 1,25 vit D 0.25 to 1.0 mcg/day orally. ! VDDR 2 –! 1,25 vit D or 1 alpha Vit D 6 mcg/kg/day (total of 30 to 60 mcg orally) with calcium supplements.
- 53. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com RENAL OSTEODYSTROPHY Low phospharous diet [low phosphate formulas to infants]. Phosphate binders to enhance fecal excretion – calcium carbonate & calcium acetate, newer non- calcium based binders – sevelamer [Aluminum based binders should be avoided]. ! Vit. D therapy : If 25 (OH) D levels are low treat with ergocalciferol. If 25 (OH) D levels are normal but PTH is high, treat with calcitriol or 1,25 (OH) D 0.01-0.05 mg/kg/24hr
- 54. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 55. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Familial hypophosphatemic Low stature in the family Dental deformities Orthopaedic abnormalities ! Consanguineous marriage indicated for hereditary hypophosphatemic rickets
- 56. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Pharmacologic Therapy of Vit D ̶ resistant rickets Familial hypophosphatemic rickets Usual vitamin D preparations are not useful for treatment in this disorder, because they lack significant 1-alpha-hydroxylase activity. ! Original treatment protocols advocated vitamin D at levels of 25,000-50,000 U/d (at the lower limit of toxic dosage). ! Amiloride and hydrochlorothiazide are administered to enhance calcium reabsorption and to reduce the risk of nephrocalcinosis.
- 57. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 58. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com FAMILIAL HYPOPHOSPHATEMIC RICKETS Replacement of Phosphate every 4 to 6 hourly ! 1 alpha Vit D
- 59. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 60. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Sulkovich’s test ! Assessment of result: ! “+” – normal level ! “++, ++++” – hypercalcaemia and hypercalciuria
- 61. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Tertiary level investigations Estimation of vitamin D metabolites to differentiate VDDR type 1 from type 2 ! Receptor vitamin D interaction : – in vitro study to assess VDDR type 2 ! Bone mineral content ! Bone densitometry
- 62. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com DIFFERENTIAL DIAGNOSIS Vitamin D ̶ deficient rickets Vitamin D ̶ dependent rickets (types I and II) Vitamin D-resistent Rickets (“looks like Rickets”): Hereditary X-linked hypophosphatemic rickets with hypocalciuria Familial hypophosphatrmic Phosphat-diabetes Achondrodroplasia Fanconi syndrome(types I and II) Pseudohypoparathyroidism Renal tubular acidosis Cystinosis Tyrosinemia Secondary Rickets (renal, gastrointestinal, tumor-associated, medications, malabsortion syndromes)
- 63. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Prognosis Usually good with improvement after exposure to sun light in the morning or afternoon or after administration of Vitamin D. ! Deformities improve with normal growth but very slowly. ! Sometimes, severe skeletal deformities require orthopedic correction.
- 64. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 65. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 66. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 67. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com nonspecific specific ! specific PREVENTION Antenatal Postnatal nonspecific
- 68. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Prevention ⦿ Exposure to ultraviolet rays in sunshine (10 to 20 minutes/day). ! ⦿ Daily requirements of vitamin D are 400-800 i.u /day. ! ⦿ For low birth weight infants, and patients of malnutrition or hypothyroidism during receiving their specific treatment, 1000-1500 i.u /day are needed for the accelerated rate of growth.
- 69. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com Also with a perspective to prevent early rickets, it is recommended that vitamin D at a dose of 2000 IU/day should be administered during the last trimester of pregnancy to mothers with poor exposure to sunlight due to various reasons and who are at high risk of Vitamin D deficiency.
- 70. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com The Endocrine Society recommends (2011) : The Endocrine Society, along with the Canadian Society of Endocrinology and Metabolism and the National Osteoporosis Foundation, published a clinical practice guideline in 2011 titled "Evaluation, Treatment and Prevention of Vitamin D Deficiency." ! 400 IU (10 mcg) for children aged 0-1 year 600 IU/day (15 mcg) for children aged 1-18 years 1500-2000 IU for all men and women older than 18 years, including lactating and pregnant women whose infants are not ingesting vitamin D.
- 71. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 72. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com
- 73. Dr.Sandeep C Agrawal Agrasen Hospital Gondia India www.agrasenortho.com This presentation is for doctors and students in general. . Graphics,Images and jpeg files are taken from Google and yahoo Image to heighten the specific points in this presentation. • If there is any objection/or copyright violation, please inform drsandeep123@gmail.com for prompt deletion. • It is intended for use only by the doctors of orthopaedic surgery. . Views expressed in this presentation are personal. • .For any confusion please contact the sole author for clarification. • Every body is allowed to copy or download and use the material best suited to him. There is no financial involvement. • For any correction or suggestion please contact drsandeep123@gmail.com or www.agrasenortho.com