1. Dyslipidaemia
LIPIDS= diverse heterogenousgroupof substanceswhichare insoluble inwaterbutsolubleinorganicsolvents.Include
triglycerides/cholesterol/phospholipids/waxes/steroids
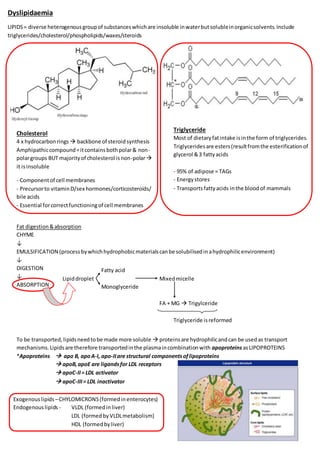
Cholesterol
4 x hydrocarbonrings backbone of steroidsynthesis
Amphipathiccompound=itcontainsbothpolar& non-
polargroups BUT majorityof cholesterol isnon-polar
it isinsoluble
- Componentof cell membranes
- Precursorto vitaminD/sex hormones/corticosteroids/
bile acids
- Essential forcorrectfunctioningof cell membranes
Triglyceride
Most of dietaryfatintake isinthe form of triglycerides.
Triglyceridesare esters(resultfromthe esterificationof
glycerol &3 fattyacids
- 95% of adipose = TAGs
- Energystores
- Transportsfattyacids inthe bloodof mammals
Fat digestion&absorption
CHYME
↓
EMULSIFICATION (processbywhichhydrophobicmaterialscanbe solubilisedinahydrophilicenvironment)
↓
DIGESTION
↓
ABSORPTION
To be transported,lipidsneedtobe made more soluble proteinsare hydrophilicandcan be usedas transport
mechanisms.Lipidsare therefore transportedinthe plasmaincombinationwith apoproteins asLIPOPROTEINS
*Apoproteins apo B, apoA-I, apo-IIare structural componentsoflipoproteins
apoB,apoE are ligandsfor LDL receptors
apoC-II= LDL activator
apoC-III= LDL inactivator
Fatty acid
Lipiddroplet Mixedmicelle
Monoglyceride
FA + MG Trigylceride
Triglyceride isreformed
Exogenouslipids –CHYLOMICRONS(formedinenterocytes)
Endogenouslipids - VLDL (formedinliver)
LDL (formedbyVLDLmetabolism)
HDL (formedbyliver)
2. Lipoproteins
EXOGENOUS I.E. DIETARY LIPID
ENDOGENOUS LIPID
Free fattyacids& free glycerol are takenupbymicelles &
absorbedbe enteroctres.
↓
Re-esterification
↓
Packagedintochylomicrons
↓
AbsorbedintoGIlymphaticdrainage,intothe thoracicduct&
intothe blood.
In the blood, chylomicrons acquire apoC and apoE from
HDL
↓
Hydrolysed by LPL into chylomicrons remnants which
are cleared in the liver
Carbs
Proteins Acetyl-CoA CHOLESTEROL
Alcohol
Sat. Fats
Endogenouspathway=VLDL synthesisinthe liver
Cholesterol&fattyacidspackagedintoVLDL withapoB-100
↓
HydrolysedbyLPLintoIDL
↓
Hydrolysedbyhepaticlipase LDL
↓
Thenonto LDL receptorsinliver& extra-hepatictissues
Lipoprotein lipase
- Removesmaterial fromchylomicronstherefore
leavingchylomicronremnants
- AllowsTAGto be usedbytissues
- Foundon surface of capillariesorhepatocytes act
on lipoproteinstravellinginbloodstream
- Fattyacids releasedneartissuestherefore there isa
highconcentrationthatdiffusesintotissues
oxidise forf.acids
storage
phospholipidsynthesis
Hepatic lipase
- Formof LPL on the surface of hepatocytes
- ConvertsIDL LDL containingCHOLESTEROL
- LDL receptors(LDLr) intissues
- LDL deliverscholesterol totissueswhichuse itfor
steroidhormones/vitD
- Alsotransportscholesteroltobloodvesselwall
atheroscleroticplaques
arterial narrowing
3. LDL isthe most atherogenic.
The onlyapoproteinassociatedwithitisapoB-
100 therefore mutationsinapoB-100or LDL
receptorswill resultindisease.
VLDL mixeswiththe plasma.
Chylomicronsare large andnotvery
dense settle ontopof plasma.
HDL metabolism
= “reverse cholesterol transport”
- promotesthe removal of fattydepositsinthe bloodvessel wall.
Picksup cholesterolfromthe peripheryandtakesitback to the
liver.
HDL hasanti-oxidantproperties&preventsthe oxidationof LDL.
*Anti-thrombogenic
*Inhibitsplateletaggregation
*Promotesplateletbreakdownby↑ prostacyclinsynthesis
Efflux of cholesterolfromcellsregulatedbyCERP(cholesterolefflux
regulatoryprotein) encodedby ACBA1gene.Thisisanactive
process& needsATP.
Cholesterol is either
taken up by VLDL via CETP
scavenged into liver or macrophages by SR-B1
(scavenger receptor B1)
Free cholesterol (bound to apoAI) esterified
by LCAT
Transfer of cholesterol Uptake of cholesterol
esters to VLDL by CERP esters by SR-B1
Macrophage scavengerreceptor
= alternative meansforcholesterol uptake
- Nospecific takesupa varietyof particles
- In the circulation,LDLcan become damaged
(oxidised) there receptorsrecognised
modifiedLDL
- Uptake isn’tregulatedtherefore
macrophagescan become full of lipid&turn
intofoamcells= formsthe basisof an
atheroscleroticplaque
4. Blood cholesterol is affected by the
amount and type of fat consumed Unsaturated fatty acids
Saturated/trans fatty acids
Decreased total and LDL cholesterol
Increased total LDL cholesterol in blood in blood
Fatty acidsaffectLDLr expression.UnsaturatedfattyacidsupregulteLDLrtherefore LDLis clearedmore effectivelyfromblood.
Lipidmeasurementin practice
- Total cholesterol
- HDL
- Triglycerides
- LDL
CARDIOVASCULARDISEASEISTHE LEADING CAUSE OF DEATH AMONG ADULTS WORLDWIDE
- Coronarydisease =7.2 million Risk prediction?
- Cancer= 6.3 million - Sex – oestrogenhasa protective effect
- Cerebrovasculardisease =4.6 million - Diabetic?
- Acute LRTI = 3.9 million - Smoker?(still consideredasasmokerif theyhave
- TB = 3 million smokedwithinthe last5years)
- COPD= 2.9 million
Primary
dyslipidaemia
(mustalwaysbe
excluded!)
Familial hypercholesterolaemia ↑ LDL Corneal arcus/
Tendon xanthomata/
Xanthelasma
Familial defective apoB-100 ↑ LDL Corneal arcus/
Tendon xanthomata/
Xanthelasma
Familial combined
hyerplipidaemia
↑ LDL/↑ VLDL/↓ HDL Corneal arcus/
Xanthelasma
Remnant particle disease ↑ IDL Palmar striae
Familial hypertriglyceridaemia ↑ VLDL/ ↑ chylomicrons Hepatomegaly/
Lipaemia retinalis
Lipoprotein lipase ↑ chylomicrons
Secondary
dyslipidaemia
Endocrine Diabetes mellitus
Thyroid disease
Pregnancy
Nutritional Obesity
Alcohol intake
Anorexia nervosa
Renal disease Nephrotic syndrome
CRF/CKD
Drugs β-blockers/thiazides/steroid hormones
Hepatic Cholestasis/gall stones/hepatocellulardysfunction
Immunoglobulin excess Paraproteinaemia
AIDS
LDL = Total cholesterol –HDL – (triglycerides/2.2)
BUT thisisonlyapplicable if TAG< 4.5mmol/L as mostcholesterol will be from
VLDL not LDL.
Predominantlipids:
CHYLOMICRONS= TRIGLYCERIDES
VLDL = TRIGLYCERIDES
LDL = CHOLESTEROL
5. Familial hypercholesterolaemia
Definition&diagnosis of FH
a) Adults:total cholesterol>7.5mmol/L
Children:total cholesterol>6.7mmol/L
A
PLUS
B or Cb)
TendonXanthomatainpatient/1st
/2nd
degree relatives
c) DNA-basedevidence of LDLreceptormutationor familial apoB-100
d) Fam Hx of MI before 50 yrs ingrandparent/aunt/uncle orbefore 60inparent/sibling/child THEN PLUS
D OR E
e) Fam Hx of raisedcholesterol >7.5mmol/Linadult1st
or 2nd
degree relative
XANETHELASMA CORNEAL ARCUS
- Autosomal dominantinheriteddisorderof
lipoproteinmetabolism veryhighplasmalevelsof
LDL cholesterolandincreasedriskof premature heart
disease
- Prevalence –1/500
- 110,000 people inthe UK, 10 millionworld-wide
- Male:Female ratio=1:1
- Untreated,50% of menwill sufferwithCHDbythe
age of 50. At least30% of womenwill sufferwithCHD
by the age of 60.
DYSFUNCTIONALLDLr preventLDL from
MUTATIONS INapoB-100 binding ↑LDL
RISKASSESSMENT – Total cholesterol &HDL
TREATMENT TARGETS – Total cholesterol &LDL
The risk calculationmaynotbe appropriate incertainindividuals&maybe higherthanestimatedincertain
people e.g.
* FamilyHx of premature CVD
* Metabolicsyndrome
* Premature menopause
* Ethnicminorities
*Diabetes ALWAYSEXCLUDE THE POSSIBILITY OF FAMILIAL HYPERCHOLESTEROLAEMIA IN
YOUNGERPATIENTS PRESENTING WITH TOTAL CHOLESTEROL >7.5mmol/L