8447779800, Low rate Call girls in Uttam Nagar Delhi NCR
Pathways Between Pulpal and Periodontal Infections
1. J Clin Periodontol 2002: 29: 663–671 Copyright C Blackwell Munksgaard 2002
Printed in Denmark . All rights reserved
0303-6979
M. Zehnder1
, S. I. Gold2
and
Pathologic interactions in pulpal G. Hasselgren1
1
Columbia University, School of Dental and
Oral Surgery, Division of Endodontics, New
York, NY, 2
Columbia University, School ofand periodontal tissues Dental and Oral Surgery, Division of
Periodontics, New York, NY, USA
Zehnder M, Gold SI, Hasselgren G. Pathologic interactions in pulpal and
periodontal tissues. J Clin Periodontol 2002; 29: 663–671. C Blackwell Munksgaard,
2002.
Abstract
Both endodontic and periodontal disease are caused by a mixed anaerobic infec-
tion. The pathways for the spread of bacteria between pulpal and periodontal
tissues have been discussed with controversy. This article is an attempt to provide
a rational approach to the perio-endo/endo-perio question based on a review of Key words: combined lesion; endo-perio,
infection; pathways; PDL; perio-endo; pulp;the relevant literature. In the light of evidence, clinical concepts for the diagnosis
reviewand treatment of lesions involving both periodontal and pulpal tissues are dis-
cussed. Accepted for publication 31 July 2001
A lesion involving both periodontal and
pulpal tissues can be of primary endo-
dontic, primary periodontal or stem
from separate origins (meaning that
both the endodontic lesion and the
marginal periodontal lesion have de-
veloped independently). Different
authors have created varying nomencla-
tures for these pathologies, based on
either aetiological or clinical criteria, or
a combination of these (Oliet & Pollock
1968, Simon et al. 1972, Guldener
1985). The clinical aspects of perio-
endo lesions have been discussed in
depth (Hiatt 1977, Harrington 1979,
Gargiulo 1984, Meng 1999). However,
scientific support for the current under-
standing of the matter is sparse. Much
of what is in the literature consists of
anecdotal reports. There is general
agreement today that the vast majority
of pulpal and periodontal lesions are a
result of bacterial infection. Under
which conditions and especially in
which direction spread of the disease
occurs in the pulpo-periodontal con-
tinuum remains a matter of controversy.
This article attempts to provide a ra-
tional approach to the perio-endo ques-
tion based on a review of the relevant
literature. Special attention is given to
the natural and man-made gates con-
necting the involved tissues and the
communication of microorganisms and
their products within these pathways.
Clinical considerations are discussed
for each type of lesion, using the classi-
fication of Simon et al. (1972), separat-
ing lesions involving both periodontal
and pulpal tissues into the following
groups:
O primary endodontic lesions with sec-
ondary periodontal involvement,
O primary periodontal lesions with sec-
ondary endodontic involvement, and
O true combined lesions.
Microbiology of endodontic and
periodontal lesions
In a letter to the Royal Society of Lon-
don in 1683, Antoni van Leeuvenhoek,
the father of microbiology, described
the ‘animalcules’ contained in dental
plaque and tartar and produced the
first drawing of bacteria (Dobell 1958).
The presence of bacteria in necrotic hu-
man pulp tissue was first described by
Miller (1894). It was not until the
groundbreaking experiments in animal
models by Gupta et al. (1957) and
Kakehashi et al. (1965) that micro-
organisms were established as the main
cause of periodontal and pulpal disease.
The concepts obtained from the pre-
viously cited animal studies were later
confirmed in man (Löe et al. 1965,
Sundqvist 1976). Periodontal disease is
now thought by most researchers to be
caused by a mixed anaerobic infection,
modulated by a complex interplay with
local and host factors (for review, see
Loesche 1999, Page 1999). Similarly, en-
dodontic infection of necrotic pulp
tissue is of an anerobic nature (Sundqv-
ist 1976). An exception to this rule
seems to be the microaerophilic A. acti-
nomycetemcomitans, which has been as-
sociated with aggressive periodontitis
(Newman & Socransky 1977). Most of
the species that have been found in in-
fected root canals can also be present
in the periodontal pocket (Moore 1987,
Sundqvist 1994). However, Porphyro-
monas endodontalis seems to be very
rare in oral infections other than those
of endodontic origin (VanWinkelhoff et
al. 1988). Overall, the root canal flora
does not appear to be as complex as the
periodontal flora of adjacent pockets
(Kurihara et al. 1995). However, it is an
inherent problem in bacterial sampling
of periodontal pockets that strains from
more shallow levels of the site are har-
2. 664 Zehnder et al.
vested along with the strains at the
front of the lesion. In patients with lo-
calized aggressive periodontitis, more
than 50% of the flora from the deepest
portion of the pocket consists of Gram-
negative rods (Newman & Socransky
1977). When classifying microbiota by
morphological criteria with interference
microscopy, no significant difference
was found between infected root canals
and adjacent periodontal pockets (Ko-
bayashi et al. 1990). Using anaerobic
culturing techniques, the overall flora
also appears similar in deepened
pockets and adjacent necrotic pulps
(Kipioti et al. 1984). Similar conditions
favoring anaerobic growth appear to be
present in both deepened periodontal
pockets and infected pulpal tissues. In
addition, it should not be forgotten that
the source of both infections is the
same, namely, the more than 400 bac-
terial species that are present in the
flora of the oral cavity.
As in any opportunistic infection, in
both pulpal and periodontal disease it
is quite difficult to evaluate which
microbiota actually cause the problem
and which bacteria are found simply
because the environment favors their
selection. Exacerbations of periapical
lesions appear to be linked to the pres-
ence of black-pigmented, Gram-nega-
tive anaerobic rods in the root canal
system (Sundqvist 1976, Yoshida et al.
1987, Haapasalo 1989, Sundqvist et al.
1989, Gomes et al. 1994). At least in the
case of Prevotella oralis, these bacteria
appear to depend on other strains to
develop their full pathogenic potential
in the root canal system, and were
found to be unable to survive if mono-
inoculated in root canals of monkeys
(Fabricius et al. 1982). The idea of posi-
tive microbial interaction in endodontic
infections was underlined further by
Sundqvist (1992), who demonstrated
that certain bacteria are more likely to
be found together in the root canal
flora. In a study on 13261 plaque
samples, Bacteroides forsythus, Porphy-
romonas gingivalis and Treponema
denticola, if found together, were highly
correlated with pocket depth and
bleeding on probing (Socransky et al.
1998). This complex was also found in
two of 28 infected root canals (Siqueira
et al. 2000). However, the sample size in
the latter study was much too small for
any definite conclusions. It has been
noted that the endodontic flora can ap-
pear in clusters of mixed bacterial con-
tent similar to the arrangement seen in
subgingival plaque (Nair 1987). Such
matrix-enclosed communities of bac-
teria evolved to permit survival of the
whole community, and are called bi-
ofilms (Costerton et al. 1994).
In conclusion, the similarities be-
tween the endodontic and periodontal
microflora suggest that cross-infection
between the root canal and the peri-
odontal pocket can occur. This idea is
supported by the presence of anatomi-
cal pathways between the pulp and the
periodontal ligament (Kerekes & Olsen
1990).
Pathways connecting endodontic
and periodontal tissues
There are two forms of possible path-
ways for bacteria and their products
connecting the two tissues: anatomical
and non-physiological.
Anatomical pathways
The major connections between peri-
odontal and pulpal tissues are the api-
cal foramina. In addition to these main
avenues of communication, there are a
multitude of branches connecting the
main root canal system with the peri-
odontal ligament. These root canal
ramifications were first described some
100years ago (Preiswerk 1901, Fischer
1907), and have since been subdivided
into furcated, collateral, lateral, second-
ary, accessory, intercanal and reticular
canals (DeDeus 1975), as well as fur-
cation canals (Vertucci & Williams
1974). For simplicity’s sake, this paper
will use the term ‘accessory canal’ for
any ramification that connects the root
canal system to the periodontal liga-
ment. It has been speculated that these
channels are created by the interference
of persistent blood vessels during the
downward growth of the sheath of
Hertwig (Barrett 1925). This hypothesis
is underlined by the finding that acces-
sory canals usually contain blood ves-
sels (Russell & Kramer 1956). Acces-
sory canals are most frequent in the
apical third of the root (DeDeus 1975),
with ramifications at the very tip of the
root having the highest incidence (Hess
1917). In the latter study, maxillary
third molars had the highest incidence
of accessory canals, followed by maxil-
lary lateral and central incisors (Hess
1917). Several authors have described
the existence of accessory canals lead-
ing from the pulp chamber and/or the
main canals into the furcation area of
multirooted teeth (Barrett 1925, Seltzer
et al. 1963b, Lowman et al. 1973, Ko-
enigs et al. 1974, Burch & Hulen 1974,
Vertucci & Williams 1974, Gutmann
1978, Perlich et al. 1981, Vertucci & An-
thony 1986). A variety of techniques
have been employed for these studies,
which may explain the divergent results.
While scanning electron microscopy
studies reveal a high incidence of open-
ings on the periodontal surface of mo-
lar furcations (Vertucci & Anthony
1986), fewer such openings can be
found on the floor of the pulp chamber
(Perlich et al. 1981). This phenomenon
is explained by the finding that the ma-
jority of these ‘canals’ are present only
in the cementum layer that covers the
furcation; they do not reach the dentin
and contain connective tissue rather
than blood vessels (Schroeder & Scherle
1987). Patent canals leading from the
pulp chamber into the furcation only
occur in about 10% of all molars (Vert-
ucci & Williams 1974). However, patent
canals connecting the main root canal
system to the periodontal ligament in
the whole furcation area of molars are
found in 30–60% of investigated molars
(Lowman et al. 1973, Gutmann 1978),
predisposing this area to be a zone of
intense communication between pulpal
and periodontal tissues.
In addition to the apical foramina
and accessory canals, there is a third
possible route for bacteria and their
products, the dentinal tubules. Dentinal
tubules are formed or, better, left out
during tooth development by odonto-
blasts, which trail their processes as
they grow centripetally while secreting
the dentin matrix. The extent of these
processes in the dentinal tubules of fully
formed dentin is a matter of dispute;
however, it is most likely that the
odontoblastic process does not reach
further than 0.5mm into the dentin
(Garberoglio & Brännström 1976).
Dentinal tubules are filled with a fluid
(Spreter von Kreudenstein & Stüben
1955) similar in composition to extra-
cellular fluid (Coffey et al. 1970). In a
mature tooth, each individual dentinal
tubule can be regarded as an inverted
cone with the smallest dimension at the
periphery and the largest dimension at
the pulp. The opening of each of these
small tunnels facing the periodontal
ligament is sealed with cementum. At
3.5mm distance from the pulp, the
mean tubule diameter was found to be
0.8mm, compared to 2.5mm at the pul-
pal wall (Garberoglio & Brännström
3. Pulpal and periodontal tissue pathways 665
1976). The number of dentinal tubules
per mm2
decreases from the pulp to the
periphery (Garberoglio & Brännström
1976). Furthermore, the total density of
tubules is significantly lower in the api-
cal root region than in the midroot and
cervical areas (Carrigan et al. 1984).
The odontoblastic process, collagenous
fibers and the sheet-like lamina limitans
in the tubule are tissue structures that
further diminish the functional tubule
radius to 5–40% of the anatomical ra-
dius (Michelich et al. 1978).
Non-physiological pathways
Iatrogenic root canal perforations are
serious complications during dental
treatment and have a rather poor prog-
nosis (Petersson et al. 1985). Perfor-
ations may be produced by powered ro-
tary instruments during the attempt to
gain access to the pulp, or during prep-
aration for a post. Improper manipula-
tion of endodontic instruments can also
lead to a perforation of the root.
The second group of artificial path-
ways between periodontal and pulpal
tissues are vertical root fractures. Verti-
cal root fractures are caused by trauma
and have been reported to occur in both
vital and non-vital teeth (Chan et al.
1999). In vital teeth, vertical fractures
can be continuations of coronal frac-
tures in the ‘cracked tooth syndrome’
(Cameron 1964) or can occur solely on
root surfaces (Chan et al. 1999). In en-
dodontically treated teeth, the incidence
of vertical root fractures is higher in
teeth that were filled with lateral con-
densation technique as compared to
teeth filled with single cone technique
(Morfis 1990). Teeth restored with in-
tracanal posts are more susceptible to
fracture than root-filled teeth without
posts, and the extension of posts be-
yond the coronal half of root canals has
a significant negative effect on the inci-
dence of root fractures as compared to
shorter posts (Morfis 1990).
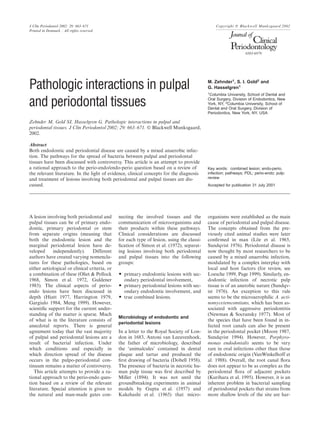
Spread of the disease and clinical
considerations
The transfer of bacterial flora between
periodontal and pulpal tissues is sum-
marized in a schematic diagram in Fig.
1. In the following, a more detailed dis-
cussion will be given, according to the
classification of lesions involving both
periodontal and pulpal tissues by Si-
mon et al. (1972). Some clinical con-
siderations are discussed for each type
of lesion, based on the evidence of its
bacterial aetiology.
Primary endodontic lesions with
secondary periodontal involvement
The root canal system primarily be-
comes infected as a result of dental
caries (Reeves & Stanley 1966), trau-
matic injuries (Sundqvist 1976) and co-
ronal microleakage (Madison & Wilcox
1988). The influence of infected pulp
tissue on a healthy periodontium has
been directly correlated with the total
microbial content in the root canal sys-
tem (Byström et al. 1987), and with the
length and time the periapical tissues
are exposed to the infecting micro-
organisms (Korzen et al. 1974). As in
periodontal disease, certain host factors
or a lack thereof may also play a roˆle in
the development of periapical pathosis.
For instance, when exposed to the same
endodontic pathogens, rats with strep-
tozotocin-induced diabetes develop sig-
nificantly larger periapical lesions than
healthy control animals (Kohsaka et al.
1996). In general, individuals with de-
fects in the non-specific immune system
have increased susceptibility to bac-
terial infections, including periodontitis
(Van Dyke & Hoop 1990). Although
not yet investigated, it might be antici-
pated that patients suffering from dis-
eases affecting the non-specific immune
response are also more susceptible to
the progression of pulpal infection and
to increased periapical destruction (Sta-
shenko et al. 1998).
Fig.1. Schematic diagram illustrating possible pathways as well as the direction within these
pathways (small arrowheads) for spread of infection between pulpal and periodontal tissues.
If a pulp is only inflamed, but not yet
necrotic, it should essentially be re-
garded as non-infected and no major
breakdown of the periapical tissues
should be expected. It has been estab-
lished histologically that bacteria do
not invade vital pulp tissue (Langeland
1987). However, minor periapical radio-
lucencies can occur in spite of the fact
that vital pulp functions prevail (Lange-
land 1987). Moreover, it is a common
clinical observation that in multirooted
teeth, vital tissue can be found in canals
adjacent to ones containing completely
necrotic pulp tissue. Breakdown prod-
ucts from necrotic uninfected pulps do
not seem to be sufficient to cause peri-
apical pathosis (Bergenholtz 1974,
Sundqvist 1976, Möller et al. 1981). In
addition, there does not seem to be
much breakdown from dead, uninfected
tissue. In contrast, breakdown products
from the cell walls of Gram-negative
bacteria found in infected root canals
(Dahle´n & Bergenholtz 1980) can cause
inflammatory alterations in the peri-
apical area (Dwyer & Torabinejad
1981). Hence, infected necrotic pulps
will always lead to periapical tissue re-
actions if not treated (Sundqvist 1976,
Möller et al. 1981). The location of this
inflammation is most often at the apex
of the tooth. However, periodontal
tissue breakdown due to endodontic in-
fection not infrequently occurs around
the opening of an accessory canal on
lateral root surfaces or in the furcation
region of multirooted teeth. Such
lesions can mimic marginal periodontal
4. 666 Zehnder et al.
pathology, and have been termed ‘retro-
grade periodontitis’ (Simring & Gold-
berg 1964).
Similarly, teeth with iatrogenic root
perforations cause inflammatory reac-
tions in the periodontal ligament. After
an observation period of 1year, a severe
inflammation was noted in the peri-
odontal ligament surrounding the site
of experimental root perforation in 37
of 51 dog teeth (Petersson et al. 1985).
In the same study, epithelial down-
growth towards the perforation was
noted, creating a marginal periodontal
defect. This phenomenon seems to be
more likely with the perforation site
close to the epithelial attachment, and
may explain the poorer prognosis of
perforations in the furcation area of
molars (Strömberg et al. 1972a).
A substantial effect of infected pulp
tissue on the healthy periodontium via
dentinal tubules is very unlikely. Due to
its physiological features, discussed
above, dentin and the overlying ce-
mentum form a natural barrier against
bacterial penetration. In fact, it was
found that healthy dentin alone signifi-
cantly restricts the diffusion of Porphyr-
omonas gingivalis proteins in vitro (Pis-
siotis & Spångberg 1992). However, in
heavily infected root canals, bacteria
are found from a few micrometers into
the dentin to approximately halfway to
the cementodentinal junction, and de-
generative alterations can be observed
in the cementum (Armitage et al. 1983).
The host tissue response to bacterial
spread from an infected root canal can
initially take two forms: an acute abscess
or a chronic inflammatory reaction.
Which direction the infectious process
takes is in large measure dependent on
the virulence and the amount of bacteria
present in the root canal. In acute forms
of periapical lesions, bacteria can be
found in periapical tissues (Nair 1987).
Acute periapical lesions or exacer-
bations of chronic lesions may drain
through sinus tracts, sometimes reaching
the gingival sulcus. Following the initial
expansion, which involves destruction of
the periodontal ligament and the ad-
jacent alveolar bone, a balanced host–
parasite relationship is usually estab-
lished (Yu & Stashenko 1987). The in-
flammatory process may then remain
unchanged for years. Periapical lesions
unaffected by marginal periodontal dis-
ease are periapical cysts in 15%, granu-
lomas in 50% and periapical abscesses in
35% of the cases (Nair et al. 1996).
Chronic, non-symptomatic periapical
lesions are usually free of bacteria, but
are maintained by endodontic infection
(Nair 1987).
Clinical considerations
If a tooth with an unusual periodontal
breakdown does not have a root filling,
the first step for proper perio-endo di-
agnosis will be a vitality test. It is well-
known that pulp tests cannot provide
an accurate assessment of the histologi-
cal status of the pulp (Greth 1933, Selt-
zer et al. 1963a). However, it has been
shown that the probability of a non-
sensitive reaction representing a ne-
crotic pulp is 89% with the cold test and
88% with the electric pulp test
(Petersson et al. 1999). As mentioned
above, a necrotic pulp in association
with a deep periodontal defect should
always be suspected to harbor bacteria
and should therefore be treated endo-
dontically. If the rest of the dentition is
periodontally healthy and a vertical
root fracture has been ruled out, heal-
ing of the attachment apparatus can be
expected after endodontic treatment
without any periodontal treatment
(Fig.2). Some clinical folklore still
exists as to the belief that fistulas of en-
dodontic origin can cause a periodontal
problem. However, it has been demon-
strated that, after proper root canal
treatment, fistulas originating from an
endodontic lesion heal even if they have
been present for a long time (Strömberg
et al. 1972b).
In this context, it should be noted
that cleaning and shaping of the root
canal in combination with irrigation
Fig.2. Male, age 45, presenting with severe
bone loss around the distal root and in the
furcation area of the mandibular left second
molar. Pus was draining through the sulcus.
The rest of the dentition was in fair to good
periodontal condition. The tooth was non-
responsive to cold test (Endo IceA
, Hygenic,
Akron, OH, USA). Endodontic treatment
was administered in two visits, with an in-
tervisit calcium hydroxide medication. No
periodontal treatment was rendered. At the
6-month recall visit, repair of the bony lesion
could be observed (Courtesy of Dr Joshua
Most, New York, NY, USA).
with sodium hypochlorite alone can not
render the root canal system free of cul-
tivable bacteria, but an additional in-
terappointment medication with a cal-
cium hydroxide dressing can
(Byström & Sundqvist 1983, Byström et
al. 1985).
In root-filled, non-vital teeth with
periapical lesions, it should be kept in
mind that the periapical radiolucency
does not necessarily indicate an infec-
tion of the root canal system. It has
been shown that periapical lesions in
endodontically treated teeth take up to
4years to heal (Strindberg 1956). The
importance of following up each lesion
can therefore not be overemphasized.
The prognosis of root canal perfor-
ations can be augmented by a stringent
aseptic technique and immediate clo-
sure of the via falsa with a material that
provides maximal bacterial sealing abil-
ity and minimal tissue irritation (Seltzer
et al. 1970).
Primary periodontal lesions with
secondary endodontic involvement
The formation of bacterial plaque on
exposed root surfaces following peri-
odontal disease theoretically has the
chance to induce pathological changes
in the healthy pulp tissue along the very
same pathways, as an endodontic infec-
tion can affect the periodontium in the
opposite direction. Only a few studies
have dealt with the matter of bacterial
transfer from the infected periodontium
towards the uninfected pulp and pulpal
reactions to periodontal disease. Find-
ings have been very contradictory.
Some researchers have reported sub-
stantial pathological change and fre-
quent necrosis in the pulp tissue due to
periodontal disease, especially when ac-
cessory canals are present (Bauchwitz
1932, Seltzer et al. 1963b, Rubach &
Mitchell 1965). Other investigators have
stated that pulps in periodontally
affected teeth remain within normal
limits regardless of the severity of the
periodontal pathosis (Mazur & Massler
1964, Czarnecki & Schilder 1979). In a
well-designed histological study on 60
caries-free teeth with various degrees of
periodontitis, Langeland et al. (1974)
convincingly demonstrated that patho-
logic changes do occur in the pulp when
periodontal disease is present; however,
the pulp does not succumb as long as
the apical foramen is not involved. It
therefore seems evident that peri-
odontal disease rarely jeopardizes the
5. Pulpal and periodontal tissue pathways 667
vital functions of the pulp unless the
disease process has reached a terminal
stage and involves the main pulpal
blood supply.
Some controversy remains as to
whether the removal of cementum dur-
ing scaling and root planing has an
untoward effect on the pulp by opening
the dentinal tubules to bacterial pene-
tration. In 21 human teeth affected by
terminal periodontal attachment loss,
invading bacteria were found in the
outer third of the dentinal tubules in
eight of 15 teeth that had received root
planing and in three of six untreated
teeth (Adriaens et al. 1987). Unfortu-
nately, no attention was given to the
state of the pulp in that study. In mon-
keys, teeth subjected to scaling and sub-
sequent plaque accumulation in com-
parison with teeth with periodontitis
alone exhibit no obvious aggravation or
increased incidence of pathologic pulp
reactions (Bergenholtz & Lindhe 1978).
As long as the pulp maintains its vital
functions, an outward flow of dentinal
fluid may be expected upon removal of
the cementum barrier (Vongsavan &
Matthews 1991). This fluid flow may
have a protective, flushing action, which
may reduce the inward diffusion of nox-
ious bacterial products in exposed den-
tin (Pashley & Matthews 1993). Indeed,
in a well-controlled in vivo study using
human third molars bound for extrac-
tion, it was found that bacteria invade
dentinal tubules of devitalized teeth
much more readily than the tubules of
vital control teeth (Nagaoka et al.
1996). On a more long-term basis, the
pulp tissue will protect itself against
noxious agents by formation of repara-
tive dentin (Seltzer & Bender 1959). It
therefore seems unlikely that, in vital
teeth, careful scaling has a negative ef-
fect on the pulp tissue. It furthermore
does not seem very plausible that peri-
odontal disease can be maintained by a
bacterial ‘depot’ contained in infected
dentinal tubules after scaling and root
planing, as has been suggested (Adria-
ens et al. 1987).
Clinical considerations
If a tooth presenting with a breakdown
of the attachment apparatus all the way
to the apex reacts positively to cold or
electric pulp test, endodontic treatment
is not necessary and should be avoided.
The probability of a sensitive reaction
representing a vital pulp is 90% with the
cold test and 84% with the electric pulp
test (Petersson et al. 1999). Vital teeth
with apparent periapical lesions that
stem from primary periodontal break-
down are not uncommon (Figs3 and 4).
In these cases, periodontal treatment
alone should be administered (Gold &
Moskow 1987), but complete healing of
the attachment apparatus is unlikely.
Teeth that did become necrotic as a se-
quela of periodontal disease are very
rare, and are usually bound for extrac-
tion (Zehnder 2001).
Fig.3. Male, age 57, long-standing peri-
odontal disease in multiple sites. Advised
root resection and endodontic treatment on
maxillary right first molar. Patient declined
recommended treatment but agreed to surgi-
cal debridement. The patient was on periodic
periodontal (non-surgical) maintenance
treatment throughout the observation
period. At the 18-year recall visit, the tooth
was still in place and the gain of clinical
attachment was 6mm in the furcation area.
The tooth is vital (positive response to cold
test).
Fig.4. Female, age 50, long-standing recur-
rent periodontal infection. The periodontal
disease on the mandibular left central incisor
was treated surgically. Routine periodontal
maintenance was carried out in 3–4-month
intervals. Three years postoperatively, the
gain of clinical attachment was 5mm on the
distal aspect of this tooth. The tooth has re-
mained vital throughout the observation
period.
True combined lesions
These lesions occur when an endodont-
ically induced periapical lesion exists at
a tooth that is also affected by marginal
periodontitis. The two lesions can either
merge or exist separately. Merged
lesions form by ongoing marginal
attachment loss or by exacerbations of
apical periodontitis. Teeth with vertical
root fractures also belong in this cat-
egory, and have been found to have ra-
diolucencies involving the periodontal
ligament in 75% of the cases (Meister et
al. 1980). If apical foramina and acces-
sory canals are referred to as avenues
of communication for bacteria between
pulpal and periodontal tissues, vertical
root fractures should be called bacterial
highways. As a result of bacterial
growth in a fracture space, the adjacent
periodontal ligament and (in vital
cases) pulp tissue will become the seat
of an inflammatory lesion, causing
breakdown of connective tissue fibers
and alveolar bone.
Combined endo-perio lesions that
exist separately on the same tooth
(meaning that they are not physically
merged) have recently gained a lot of
attention. The roˆle of an endodontic in-
fection as a local modifying risk factor
of periodontal disease has been studied
in retrospective clinical studies on peri-
odontitis-prone patients. Single-rooted
teeth with an endodontic infection
evident as a periapical radiolucency are
significantly correlated to deeper peri-
odontal pockets (Jansson et al. 1993a),
more radiographic attachment loss
(Jansson et al. 1993b, Jansson et al.
1995) and less probing depth reduction
over time (Ehnevid et al. 1993a, Ehnev-
id et al. 1993b) compared to teeth with-
out endodontic infection. Furthermore,
endodontic infection is associated with
additional attachment loss in the fur-
cation area of molars (Jansson & Ehne-
vid 1998). Dentinal tubules devoid of
the covering cementum layer have been
suggested as possible pathways for bac-
teria in endodontically infected teeth,
leading to further periodontal break-
down (Ehnevid et al. 1995). Indeed, in
intentionally replanted, infected mon-
key teeth, denuded dentin surfaces are
associated with epithelial downgrowth
(Hammarström et al. 1986), and ex-
posed dentin surfaces show significantly
larger areas of resorption in infected
roots compared to non-infected roots.
On the other hand, cementum surfaces
exhibit an almost identical distribution
6. 668 Zehnder et al.
of tissue reactions, regardless of
whether a root canal infection is present
or not (Ehnevid et al. 1995). However,
the latter study employed a model that
involved trauma to the periodontal liga-
ment, and the results obtained can
therefore not be directly transferred to
the situation of a combined peri-
odontal-endodontic lesion. Interest-
ingly, in a well-controlled study on ex-
perimentally induced periapical in-
flammation in monkey teeth, colonies
of bacteria could be observed along the
entire length of the dentinal tubules ad-
jacent to inflamed periodontal tissue,
whereas bacteria penetrated to no more
than about one third of the tubular
length towards the cemento-dentinal
junction adjacent to a healthy peri-
odontal ligament (Valderhaug 1974).
Hence, healthy periodontal tissue, simi-
lar to healthy pulp tissue, appears to
have more defense mechanisms to resist
bacterial penetration than a diseased
tissue. Whether an intact cementum
layer is an important part of this de-
fense system remains elusive.
Clinical considerations
Root-filled teeth with unusual marginal
bone loss should be carefully inspected
for vertical root fractures and root per-
forations. Here, the comparison of ac-
tual radiographs with previous pictures
of the same area are very helpful. A
sudden and severe breakdown of bony
attachment is indicative of a vertical
root fracture. It has also been found
that vertically fractured, endodontically
treated teeth are associated with a typi-
cal, V-shaped osseous defect on the buc-
cal plate (Lustig et al. 2000). An ex-
ploratory surgical procedure is often
necessary to obtain the correct diag-
nosis. If a vertical root fracture is diag-
nosed, extraction or amputation of the
affected root remains the only good
treatment option.
Even if a fracture has been ruled out,
the treatment of teeth with combined
lesions remains challenging. It is often
hard or impossible to assess where the
defect caused by the marginal peri-
odontal disease starts and the endodon-
tic lesion ends. Yet the root canal sys-
tem, unlike the periodontal tissues, can
be freed from bacteria and then sealed.
In addition, overzealous deep scaling
and root planing may create the risk of
interfering with reattachment. Hence,
the treatment should always start with
the root canal treatment, followed by an
observation period of at least 3months.
Concluding remarks
In conclusion, it can be stated that in
the vast majority of the lesions involv-
ing the pulpo-periodontal complex, the
bacterial aetiology dictates the clinical
course of the disease and therefore the
treatment plan. Therefore, the classifi-
cation by Simon et al. (1972) has stood
the test of time and is very useful in
reaching sound clinical decisions. The
guidelines for treatment planning given
in this text are general. Other factors,
such as patient cooperation, restor-
ability and economics will influence
treatment decisions. However, the pri-
mary goal of all treatment efforts must
be to rid the patient of the infection.
In this article, cystic and neoplastic
processes, which are not related to bac-
terial invasion of either periodontal or
endodontic tissues, yet appear in these
tissues, have not been discussed, be-
cause the authors feel that they are rare
and not perio-endo lesions in the true
sense of the expression. Furthermore,
lesions that are in part caused by exter-
nal traumatic injuries to the dentition,
such as external inflammatory resorp-
tion, have also not been included.
Many of the articles cited here are
quite old; the majority of the references
were published before 1990. There are
two reasons for this: 1) some outstand-
ing studies, especially anatomical obser-
vations, are as valid today as when they
were first published; and 2) there is a
clear lack of recent documentation re-
lated to the present topic. The need for
new data can not be overemphasized.
Hopefully, some of the unanswered
questions raised in this article will pro-
vide ideas for new research projects.
Zusammenfassung
Pathologische Interaktionen bei pulpalen und
parodontalen Geweben
Sowohl die endodontalen als auch parodon-
talen Erkrankungen sind durch eine gemisch-
te anaerobe Infektion verursacht. Die patho-
genetischen Muster für die Ausbreitung der
Bakterien zwischen pulpalen und parodonta-
len Geweben sind kontrovers diskutiert wor-
den. Dieser Artikel ist ein Versuch für einen
rationalen Ansatz zu den paro-endo bzw.
endo-paro Fragen, basierend auf einer Über-
sicht der relevanten Literatur. Im Blick der
Evidence werden die klinischen Konzepte für
die Diagnose und Therapie der Läsionen, die
sowohl parodontale als auch pulpale Gewebe
einbeziehen, diskutiert.
Re´sume´
Interactions pathologiques entre les tissus pul-
paires et parodontaux.
Les maladies endodontiques et parodontales
sont toutes deux causes par une infection
mixte anae´robique. Les voies de disse´mina-
tion des bacte´ries entre les tissus pulpaires et
parodontaux ont e´te´ discute´e avec controver-
se. Cet article est une tentative d’apporter
une approche rationnelle a` la question paro-
endo/endo-paro a` partir d’une revue critique
de la litte´rature approprie´e. A la lumie`re des
preuves, des concepts cliniques pour le dia-
gnostic et le traitement des le´sions impli-
quant a` la fois les tissus parodontaux et pul-
paires sont discute´s.
References
Adriaens, P. A., Edwards, C. A., De Boever,
J. A. & Loesche, W. J. (1987) Ultrastruc-
tural observations on bacterial invasion in
cementum and radicular dentin of peri-
odontally diseased human teeth. Journal of
Periodontology 59, 493–503.
Armitage, G. C., Ryder, M. I. & Wilcox, S.
E. (1983) Cemental changes in teeth with
heavily infected root canals. Journal of En-
dodontics 9, 127–130.
Barrett, M. T. (1925) The internal anatomy
of the teeth with special reference to the
pulp with its branches. Dental Cosmos 67,
581–592.
Bauchwitz, M. (1932) Veränderungen der
Zahnpulpa und des Paradentium bei Par-
adentose. Zahnärztliche Rundschau 11,
430–438, 1228–1233, 1271–1275.
Bergenholtz, G. (1974) Micro-organisms
from necrotic pulp of traumatized teeth.
Odontologisk Revy 25, 347–358.
Bergenholtz, G. & Lindhe, J. (1978) Effect of
experimentally induced marginal peri-
odontitis and periodontal scaling on the
dental pulp. Journal of Clinical Periodon-
tology 5, 59–73.
Burch, J. G. & Hulen, S. (1974) A study of
the presence of accessory foramina and
the topography of molar furcations. Oral
Surgery, Oral Medicine and Oral Pathol-
ogy 38, 451–455.
Byström, A., Claesson, R. & Sundqvist, G.
(1985) The antibacterial effect of cam-
phorated paramonochlorophenol, cam-
phorated phenol and calcium hydroxide in
the treatment of infected root canals. En-
dodontics and Dental Traumatology 1,
170–175.
Byström, A., Happonen, R. P., Sjögren, U. &
Sundqvist, G. (1987) Healing of periapical
lesions of pulpless teeth after endodontic
treatment with controlled asepsis. Endo-
dontics and Dental Traumatology 3, 58–63.
Byström, A. & Sundqvist, G. (1983) Bacteri-
ologic evaluation of the effect of 0.5 per-
cent sodium hypochlorite in endodontic
therapy. Oral Surgery, Oral Medicine and
Oral Pathology 55, 307–312.
7. Pulpal and periodontal tissue pathways 669
Cameron, C. E. (1964) Cracked-tooth syn-
drome. Journal of the American Dental As-
sociation 68, 405–411.
Carrigan, P. J., Morse, D. R., Furst, M. L. &
Sinai, I. H. (1984) A scanning electron
microscopic evaluation of human dentinal
tubules according to age and location.
Journal of Endodontics 10, 359–363.
Chan, C.-P., Lin, C.-P., Tseng, S.-C. & Jeng,
J.-H. (1999) Vertical root fracture in endo-
dontically versus nonendodontically
treated teeth. A survey of 315 cases in Chi-
nese patients. Oral Surgery, Oral Medi-
cine, Oral Pathology, Oral Radiology and
Endodontics 87, 504–507.
Coffey, C. T., Ingram, M. J. & Bjorndall, A.
M. (1970) Analysis of human dentinal
fluid. Oral Surgery, Oral Medicine and
Oral Pathology 30, 835–837.
Costerton, J. W., Lewandowski, Z., DeBeer,
D., Caldwell, D., Korber, D. & James, G.
(1994) Biofilms, the customized mi-
croniche. Journal of Bacteriology 176,
2137–2142.
Czarnecki, R. T. & Schilder, H. (1979) A his-
tological evaluation of the human pulp in
teeth with varying degrees of periodontal
disease. Journal of Endodontics 5, 242–253.
Dahle´n, G. & Bergenholtz, G. (1980) Endo-
toxic activity in teeth with necrotic pulps.
Journal of Dental Research 59, 1033–1040.
DeDeus, Q. D. (1975) Frequency, location,
and direction of the lateral, secondary, and
accessory canals. Journal of Endodontics 1,
361–366.
Dobell, C. (1958). Anthony Van Leeuven-
hoeck and his ‘little animals’. New York:
Russell.
Dwyer, T. G. & Torabinejad, M. (1981)
Radiographic and histologic evaluation of
the effect of endotoxin on the periapical
tissues of the cat. Journal of Endodontics
7, 31–35.
Ehnevid, H., Jansson, L., Lindskog, S. &
Blomlöf, L. (1993a) Periodontal healing in
teeth with periapical lesions. A clinical
retrospective study. Journal of Clinical
Periodontology 20, 254–258.
Ehnevid, H., Jansson, L. E., Lindskog, S.
F. & Blomlöf, L. B. (1993b) Periodontal
healing in relation to radiographic attach-
ment and endodontic infection. Journal of
Periodontology 64, 1199–1204.
Ehnevid, H., Jansson, L., Lindskog, S., Wein-
traub, A. & Blomlöf, L. (1995) Endodon-
tic pathogens: propagation of infection
through patent dentinal tubules in trauma-
tized monkey teeth. Endodontics and Den-
tal Traumatology 11, 229–234.
Fabricius, L., Dahle´n, G., Holm, S. E. &
Möller, Å. J. R. (1982) Influence of combi-
nations of oral bacteria on periapical
tissues in monkeys. Scandinavian Journal
of Dental Research 90, 200–206.
Fischer, G. (1907) Über die feinere Anatomie
der Wurzelkanäle menschlicher Zähne.
Vorläufige Mitteilung. Deutsche Mon-
atsschrift für Zahnheilkunde 25, 544–552.
Garberoglio, R. & Brännström, M. (1976)
Scanning electron microscopic investiga-
tion of human dentinal tubules. Archives
of Oral Biology 21, 355–362.
Gargiulo, A. V. Jr (1984) Endodontic-peri-
odontic interrelationships. Diagnosis and
treatment. Dental Clinics of North America
28, 767–781.
Gold, S. I. & Moskow, B. S. (1987) Peri-
odontal repair of periapical lesions: the
borderland between pulpal and peri-
odontal disease. Journal of Clinical Period-
ontology 14, 251–256.
Gomes, B. P. F. A., Drucker, D. B. & Lilley,
J. D. (1994) Association of specific bac-
teria with some endodontic signs and
symptoms. International Endodontic
Journal 27, 291–298.
Greth, H. (1933). Diagnostik der Pulpaerk-
rankungen. Berlin: Hermann Meusser.
Guldener, P. H. A. (1985) The relationship
between periodontal and pulpal disease.
International Endodontic Journal 18, 41–
54.
Gupta, O. P., Auskaps, A. M. & Shaw, J. H.
(1957) Periodontal disease in the rice rat.
IV. The effects of antibiotics on the inci-
dence of periodontal lesions. Oral Surgery,
Oral Medicine and Oral Pathology 10,
1169–1175.
Gutmann, J. L. (1978) Prevalence, location,
and patency of accessory canals in the fur-
cation region of permanent molars.
Journal of Periodontology 49, 21–26.
Haapasalo, M. (1989) Bacteroides spp. in
dental root canal infections. Endodontics
and Dental Traumatology 5, 1–10.
Hammarström, L. E., Blomlöf, L. B., Feig-
lin, B. & Lindskog, S. F. (1986) Effect of
calcium hydroxide treatment on peri-
odontal repair and root resorption. Endo-
dontics and Dental Traumatology 2, 184–
189.
Harrington, G. W. (1979) The perio-endo
question: Differential diagnosis. Dental
Clinics of North America 23, 673–690.
Hess, W. (1917) Zur Anatomie der Wurzelk-
anäle des menschlichen Gebisses mit
Berücksichtigung der feinen Verzweigung-
en am Foramen apicale. Schweizerische Vi-
erteljahresschrift für Zahnheilkunde 1, 1–
53.
Hiatt, W. H. (1977) Pulpal periodontal dis-
ease. Journal of Periodontology 48, 598–
609.
Jansson, L. E. & Ehnevid, H. (1998) The in-
fluence of endodontic infection on peri-
odontal status in mandibular molars.
Journal of Periodontology 69, 1392–1396.
Jansson, L., Ehnevid, H., Blomlöf, L., Wein-
traub, A. & Lindskog, S. (1995) Endodon-
tic pathogens in periodontal disease aug-
mentation. Journal of Clinical Periodonto-
logy 22, 598–602.
Jansson, L., Ehnevid, H., Lindskog, S. &
Blomlöf, L. (1993a) Relationship between
periapical and periodontal status. A clin-
ical retrospective study. Journal of Clinical
Periodontology 20, 117–123.
Jansson, L. E., Ehnevid, H., Lindskog, S.
F. & Blomlöf, L. B. (1993b) Radiographic
attachment in periodontitis-prone teeth
with endodontic infection. Journal of Peri-
odontology 64, 947–953.
Kakehashi, S., Stanley, H. R. & Fitzgerald,
R. J. (1965) The effects of surgical ex-
posures of dental pulps in germ-free and
conventional laboratory rats. Oral
Surgery, Oral Medicine and Oral Pathol-
ogy 20, 340–349.
Kerekes, K. & Olsen, I. (1990) Similarities in
the microfloras of root canals and deep
periodontal pockets. Endodontics and Den-
tal Traumatology 6, 1–5.
Kipioti, A., Nakou, M., Legakis, N. &
Mitsis, F. (1984) Microbiological findings
of infected root canals and adjacent peri-
odontal pockets in teeth with advanced
periodontitis. Oral Surgery, Oral Medicine
and Oral Pathology 58, 213–220.
Kobayashi, T., Hayashi, A., Yoshikawa, R.,
Okuda, K. & Hara, K. (1990) The mi-
crobial flora from root canals and peri-
odontal pockets of non-vital teeth associ-
ated with advanced periodontitis. Interna-
tional Endodontic Journal 23, 100–106.
Koenigs, J. F., Brilliant, J. D. & Foreman, D.
W. Jr (1974) Preliminary scanning electron
microscope investigations of accessory for-
amina in the furcation areas of human mo-
lar teeth. Oral Surgery, Oral Medicine and
Oral Pathology 38, 773–782.
Kohsaka, T., Kumazawa, M., Yamasaki,
M. & Nakamura, H. (1996) Periapical
lesions in rats with streptozotocin-induced
diabetes. Journal of Endodontics 22, 418–
421.
Korzen, B. H., Krakow, A. A. & Green, D.
B. (1974) Pulpal and periapical tissue re-
sponses in conventional and monoinfected
gnotobiotic rats. Oral Surgery, Oral Medi-
cine and Oral Pathology 37, 783–802.
Kurihara, H., Kobayashi, Y., Francisco, I.
A., Isoshima, O., Nagai, A. & Murayama,
Y. (1995) A microbiological and immuno-
logical study of endodontic-periodontic
lesions. Journal of Endodontics 21, 617–
621.
Langeland, K. (1987) Tissue response to den-
tal caries. Endodontics and Dental
Traumatology 3, 149–171.
Langeland, K., Rodrigues, H. & Dowden, W.
(1974) Periodontal disease, bacteria, and
pulpal histopathology. Oral Surgery, Oral
Medicine and Oral Pathology 37, 257–270.
Löe, H., Theilade, E. & Jensen, S. B. (1965)
Experimental gingivitis in man. Journal of
Periodontology 36, 177–187.
Loesche, W. J. (1999) The antimicrobial
treatment of periodontal disease: Chang-
ing the treatment paradigm. Critical Re-
views in Oral Biology and Medicine 10,
245–275.
Lowman, J. V., Burke, R. S. & Pelleu, G. B.
(1973) Patent accessory canals: Incidence
in molar furcation region. Oral Surgery,
Oral Medicine and Oral Pathology 36,
580–584.
Lustig, J. P., Tamse, A. & Fuss, Z. (2000) Pat-
tern of bone resorption in vertically frac-
tured, endodontically treated teeth. Oral
Surgery, Oral Medicine, Oral Pathology,
8. 670 Zehnder et al.
Oral Radiology and Endodontics 90, 224–
227.
Madison, S. & Wilcox, L. R. (1988) An
evaluation of coronal microleakage in en-
dodontically treated teeth. Part III. In vivo
study. Journal of Endodontics 14, 455–458.
Mazur, B. & Massler, M. (1964) Influence of
periodontal disease on the dental pulp.
Oral Surgery, Oral Medicine and Oral
Pathology 17, 592–603.
Meister, F. Jr, Lommel, T. J. & Gerstein, H.
(1980) Diagnosis and possible causes of
vertical root fractures. Oral Surgery, Oral
Medicine and Oral Pathology 49, 243–253.
Meng, H. X. (1999) Periodontic-endodontic
lesions. Annals of Periodontology 4, 84–89.
Michelich, V., Pashley, D. H. & Whitford, G.
M. (1978) Dentin permeability: a compari-
son of functional versus anatomical tubu-
lar radii. Journal of Dental Research 57,
1019–1024.
Miller, W. D. (1894) An introduction to the
study of the bacterio-pathology of the
dental pulp. Dental Cosmos 36, 505–528.
Möller, Å. J. R., Fabricius, L., Dahle´n, G.,
Öhman, A. E. & Heyden, G. (1981) Influ-
ence on periapical tissues of indigenous
oral bacteria and necrotic pulp tissue in
monkeys. Scandinavian Journal of Dental
Research 89, 475–484.
Moore, W. E. C. (1987) Microbiology of peri-
odontal disease. Journal of Periodontal Re-
search 22, 335–341.
Morfis, A. S. (1990) Vertical root fractures.
Oral Surgery, Oral Medicine and Oral
Pathology 69, 631–635.
Nagaoka, S., Miyazaki, Y., Liu, H.-J., Iwam-
oto, Y., Kitano, M. & Kawagoe, M. (1996)
Bacterial invasion into dentinal tubules of
human vital and nonvital teeth. Journal of
Endodontics 21, 70–73.
Nair, P. N. R. (1987) Light and electron
microscopic studies of root canal flora and
periapical lesions. Journal of Endodontics
13, 29–39.
Nair, P. N. R., Pajarola, G. & Schroeder, H.
E. (1996) Types and incidence of human
periapical lesions obtained with extracted
teeth. Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology and Endodont-
ics 81, 93–102.
Newman, M. G. & Socransky, S. S. (1977)
Predominant cultivable microbiota in peri-
odontosis. Journal of Periodontal Research
12, 120–128.
Oliet, S. & Pollock, S. (1968) Classification
and treatment of endo-perio involved
teeth. Bulletin of the Philadelphia Dental
Society 34, 12–16.
Page, R. C. (1999) Milestones in periodontal
research and the remaining critical issues.
Journal of Periodontal Research 34, 331–
339.
Pashley, D. H. & Matthews, W. G. (1993) The
effects of outward forced convective flow
on inward diffusion in human dentine in
vitro. Archives of Oral Biology 38, 577–
582.
Perlich, M. A., Reader, A. & Foreman, D.
W. (1981) A scanning electron microscopic
investigation of accessory foramens on the
pulpal floor of human molars. Journal of
Endodontics 7, 402–406.
Petersson, K., Hasselgren, G. & Tronstad, L.
(1985) Endodontic treatment of experi-
mental root perforations in dog teeth. En-
dodontics and Dental Traumatology 1, 22–
28.
Petersson, K., Söderström, C., Kiani-Ana-
raki, M. & Le´vy, G. (1999) Evaluation of
the ability of thermal and electrical tests
to register pulp vitality. Endodontics and
Dental Traumatology 15, 127–131.
Pissiotis, E. & Spångberg, L. (1992) Dentin
as inhibitor of bacterial toxicity on pulpal
cells in vitro. Journal of Endodontics 18,
166–171.
Preiswerk, G. (1901) Die Pulpaamputation,
eine klinische, pathohistologische und
bakteriologische Studie. Österreichisch-
Ungarische Vierteljahresschrift für
Zahnheilkunde 17, 145–220.
Reeves, R. & Stanley, H. R. (1966) The re-
lationship of bacterial penetration and
pulpal pathosis in carious teeth. Oral
Surgery, Oral Medicine and Oral Pathol-
ogy 22, 59–65.
Rubach, W. C. & Mitchell, D. F. (1965) Peri-
odontal disease, accessory canals and pulp
pathosis. Journal of Periodontology 36, 34–
38.
Russell, L. H. & Kramer, I. R. H. (1956) Ob-
servations on the vascular architecture of
the dental pulp. Journal of Dental Re-
search 35, 957.
Schroeder, H. E. & Scherle, W. F. (1987) Wa-
rum die Furkation menschlicher Zähne so
unvorhersehbar bizarr gestaltet ist.
Schweizerische Monatsschrift für Zahnme-
dizin 97, 1495–1508.
Seltzer, S. & Bender, I. B. (1959) Inflam-
mation in the odontoblastic layer of the
dental pulp. Journal of the American Den-
tal Association 59, 720–724.
Seltzer, S., Bender, I. B. & Ziontz, M. (1963a)
The dynamics of pulp inflammation: cor-
relations between diagnostic data and ac-
tual histologic findings in the pulp. Oral
Surgery, Oral Medicine and Oral Pathol-
ogy 16, 846–871.
Seltzer, S., Bender, I. B. & Ziontz, M.
(1963b) The interrelationship of pulp and
periodontal disease. Oral Surgery, Oral
Medicine and Oral Pathology 16, 1474–
1490.
Simon, J. H. S., Glick, D. H. & Frank, A.
L. (1972) The relationship of endodontic-
periodontic lesions. Journal of Periodonto-
logy 43, 202–208.
Simring, M. & Goldberg, M. (1964) The pul-
pal pocket approach: Retrograde peri-
odontitis. Journal of Periodontology 35,
22–48.
Siqueira, J. F. Jr, Roˆc¸as, I. N., Souto, R., de-
Uzeda, M. & Colombo, A. P. (2000)
Checkerboard DNA-DNA hybridization
analysis of endodontic infections. Oral
Surgery, Oral Medicine, Oral Pathology,
Oral Radiology and Endodontics 89, 744–
748.
Socransky, S. S., Haffajee, A. D., Cugini, M.
A., Smith, C. & Kent, R. L. Jr (1998) Mi-
crobial complexes in subgingival plaque.
Journal of Clinical Periodontology 25, 134–
144.
Spreter von Kreudenstein, T. & Stüben, J.
(1955) Dentinstoffwechselstudien. III.
Mitteilung: Die thermische Methode zum
Nachweis des Dentinliquors. Deutsche
Zahnärztliche Zeitschrift 10, 1178–1182.
Seltzer, S., Sinai, I. & August, D. (1970) Peri-
odontal effects of root perforations before
and during endodontic procedures.
Journal of Dental Research 49, 332–339.
Stashenko, P., Teles, R. & D’Souza, R. (1998)
Periapical inflammatory responses and
their modulation. Critical Reviews in Oral
Biology and Medicine 9, 498–521.
Strindberg, L. Z. (1956) The dependence of
the results of pulp therapy on certain fac-
tors. An analytic study based on radio-
graphic and clinical follow-up examina-
tions. Acta Odontologica Scandinavica 14
(Suppl. 21), 1–175.
Strömberg, R., Hasselgren, G. & Bergstedt,
H. (1972a) Endodontic treatment of trau-
matic root perforations in man. A clinical
and roentgenological follow-up study.
Swedish Dental Journal 65, 457–465.
Strömberg, R., Hasselgren, G. & Bergstedt,
H. (1972b) Endodontic treatment of re-
sorptive periapical osteitis with fistula. A
clinical and roentgenological follow-up
study. Swedish Dental Journal 65, 467–474.
Sundqvist, G. (1976) Bacteriologic studies of
necrotic dental pulps. University Odonto-
logical Dissertation .7 Umeå: University
of Umeå.
Sundqvist, G. (1992) Associations between
microbial species in dental root canal in-
fections. Oral Microbiology and Immu-
nology 7, 257–262.
Sundqvist, G. (1994) Taxonomy, ecology, and
pathogenicity of the root canal flora. Oral
Surgery, Oral Medicine and Oral Pathol-
ogy 78, 522–530.
Sundqvist, G., Johansson, E. & Sjögren, U.
(1989) Prevalence of black-pigmented
bacteroides species in root canal infec-
tions. Journal of Endodontics 15, 13–19.
Valderhaug, J. (1974) A histologic study of
experimentally induced periapical in-
flammation in primary teeth in monkeys.
International Journal of Oral Surgery 3,
111–123.
Van Dyke, T. E. & Hoop, G. A. (1990) Neu-
trophil function and oral disease. Critical
Reviews in Oral Biology and Medicine 1,
117–133.
VanWinkelhoff, A. J., VanSteenbergen, T. J.
M. & DeGraaf, J. (1988) The role of
black-pigmented Bacteroides in human
oral infections. Journal of Clinical Period-
ontology 15, 145–155.
Vertucci, F. J. & Anthony, R. L. (1986) A
scanning electron microscopic investiga-
tion of accessory foramina in the furcation
and pulp chamber floor of molar teeth.
Oral Surgery, Oral Medicine and Oral
Pathology 62, 319–326.
9. Pulpal and periodontal tissue pathways 671
Vertucci, F. J. & Williams, R. G. (1974) Fur-
cation canals in the human mandibular
first molar. Oral Surgery, Oral Medicine
and Oral Pathology 38, 308–314.
Vongsavan, N. & Matthews, B. (1991) The
permeability of cat dentine in vivo and in
vitro. Archives of Oral Biology 36, 641–
646.
Yoshida, M., Fukushima, H., Yamamoto,
K., Ogawa, K., Toda, T. & Sagawa, H.
(1987) Correlation between clinical symp-
toms and microorganisms isolated from
root canals of teeth with periapical pa-
thosis. Journal of Endodontics 13, 24–28.
Yu, S. M. & Stashenko, P. (1987) Identifi-
cation of inflammatory cells in developing
rat periapical lesions. Journal of Endodont-
ics 13, 535–540.
Zehnder, M. (2001) Endodontic infection
caused by localized aggressive peri-
odontitis: A case report and bacteriologic
evaluation. Oral Surgery, Oral Medicine,
Oral Pathology, Oral Radiology and Endo-
dontics 92, 440–445.
Address:
Matthias Zehnder
Division of Endodontics
Columbia University School of Dental and
Oral Surgery
630W 168th Street
New York, NY 10032
USA
Tel: π1 212 305 0698
Fax: π1 212 305 8493
e-mail: mz121/columbia.edu