assessment of the male genitalia
•
18 likes•51,396 views

assessment of the male genitalia including diseases

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to assessment of the male genitalia
Similar to assessment of the male genitalia (10)
More from Carmela Domocmat
More from Carmela Domocmat (20)
Recently uploaded
Recently uploaded (20)
assessment of the male genitalia
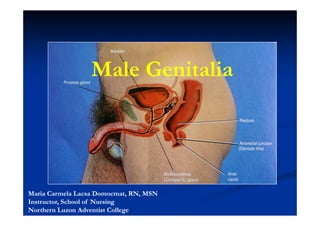
- 1. Male Genitalia Maria Carmela Lacsa Domocmat, RN, MSN Instructor, School of Nursing Northern Luzon Adventist College
- 2. Male Genitalia Anatomy and Physiology Techniques of Examination Related Abnormalities
- 3. Male Genitalia Anatomy and Physiology Maria Carmela L. Domocmat, RN, MSN
- 4. Male Genitalia The Penis Maria Carmela L. Domocmat, RN, MSN
- 5. Maria Carmela L. Domocmat, RN, MSN
- 6. Internal Structure Maria Carmela L. Domocmat, RN, MSN
- 7. Testicles Maria Carmela L. Domocmat, RN, MSN
- 8. Maria Carmela L. Domocmat, RN, MSN
- 9. Uncircumcised Circumcised Penis Penis Maria Carmela L. Domocmat, RN, MSN
- 10. Inguinal ring Maria Carmela L. Domocmat, RN, MSN
- 11. Assessment General Pubic Region Penis, Urethra Scrotum, Testes Inguinal Region
- 12. General Pubic Region Sexual Maturity Rating Hair Distribution
- 13. Sexual Maturity Rating Using the Tanner Stages, assess the developmental stage of the pubic hair, penis, and scrotum. Normal Findings • Males usually begin puberty between the ages of 9 ½ and 13 ½ . • Average male proceeds through puberty in about 3 years, with possible range of 2 to 5 years. Maria Carmela L. Domocmat, RN, MSN
- 14. Tanner’s Sexual Maturity Rating The five stages of male genital development. Stage 1 shows the undeveloped genitals of childhood. In Stage 2, pubic hair growth begins and the testicles begin to enlarge. By Stage 3, the penis grows longer and wider. The testicles continue to enlarge. Maria Carmela L. Domocmat, RN, MSN
- 15. Tanner’s Sexual Maturity Rating The five stages of male genital development. In Stage 4, the penis and testicles continue to enlarge while the head of the penis becomes more developed. In Stage 5, the genitals have become their adult size, and pubic hair covers the region. Maria Carmela L. Domocmat, RN, MSN
- 16. Tanner’s Sexual Maturity Rating Maria Carmela L. Domocmat, RN, MSN
- 17. Hair Distribution Normal Findings: • Diamond shape (triangular form) • Abundant in the pubic region. • May continue in a narrowing midline pattern to the umbilicus, around the scrotum to the anal orifice. Maria Carmela L. Domocmat, RN, MSN
- 18. Hair Distribution Normal Findings (cont’d) • Sparsely distributed on the scrotum and inner thigh and absent on penis. • More coarse than scalp hair. • No nits or lice. Maria Carmela L. Domocmat, RN, MSN
- 19. Geriatric Variation Thinner Sometimes gray Maria Carmela L. Domocmat, RN, MSN
- 20. Abnormal Findings Pediculosis Pubis Herpes Simplex
- 21. Crab lice, Pthirus pubis with reddish-brown crab feces. reddish- Maria Carmela L. Domocmat, RN, MSN
- 22. HSV Vesicles Maria Carmela L. Domocmat, RN, MSN
- 23. The Penis Inspection Palpation
- 24. Inspection •Examine the glans of the penis. If the patient is uncircumcised, ask him to retract the foreskin so that the underlying area can be inspected. Maria Carmela L. Domocmat, RN, MSN
- 25. • Inspect the anterior surface of the penis first. Ask the client to lift the penis to check the posterior surface. • Note the shape of the penis. Maria Carmela L. Domocmat, RN, MSN
- 26. Normal Findings Penis: • Cylindrical in shape. • Skin – free from lesions and inflammation. • Shaft skin – appears loose and wrinkled without erection. Maria Carmela L. Domocmat, RN, MSN
- 27. Normal Findings Penis: (cont’d) • Pink to light brown in Whites and light brown to dark brown in Blacks. • Surface vascularity may be apparent. Dorsal vein is sometimes visible. Maria Carmela L. Domocmat, RN, MSN
- 28. Normal Findings Glans penis – smooth, pink, bulbous • Varies in size and shape. • May appear round or broad. • Without lesions, swelling, and inflammation Maria Carmela L. Domocmat, RN, MSN
- 29. Foreskin or prepuce • Retracts easily to expose glans and returns to original position with ease. • No discharge. Maria Carmela L. Domocmat, RN, MSN
- 30. a. Uncircumcised: • Prepuce fold wrinkled, loosely attached to the underlying glans • Darker in color than glans • Should retract easily • Smegma (white, cottage- cottage- cheese- cheese-like substance) may be seen over the glans Maria Carmela L. Domocmat, RN, MSN
- 31. b. Circumcised: • Prepuce often absent, or small flaps remain at corona. • No smegma. • (Note: circumcised penises have varying lengths of foreskin remaining; some have multiple folds and others have few or none.) Maria Carmela L. Domocmat, RN, MSN
- 32. Let’s Watch: Inspecting the Penis
- 33. Palpation • Between the thumb and the first two fingers, palpate the entire length of the penis. • Note any pulsations, tenderness, masses, or plaques. Maria Carmela L. Domocmat, RN, MSN
- 34. Normal Findings • Pulsations may be present on the dorsal sides of the penis. • Non-tender. Non- • No masses or firm plaques are palpated. Maria Carmela L. Domocmat, RN, MSN
- 35. Make sure that you return the foreskin (if uncircumcised) to its normal place at the end of the exam. If not returned, it can cause paraphimosis - severe venous and arterial obstruction, leading to necrosis of the glans of the penis. Maria Carmela L. Domocmat, RN, MSN
- 36. Geriatric Variation Decrease in size of penis Maria Carmela L. Domocmat, RN, MSN
- 37. Abnormal Findings Chordee Priapism Phimosis Paraphimosis
- 38. Abnormal Curvature Congenital: Chordee Acquired: caused by Peyronie’s Disease Maria Carmela L. Domocmat, RN, MSN
- 39. Congenital Chordee Maria Carmela L. Domocmat, RN, MSN
- 40. Congenital Chordee Maria Carmela L. Domocmat, RN, MSN
- 41. Acquired curvature caused by Peyronie’s disease Maria Carmela L. Domocmat, RN, MSN
- 42. Priapism Maria Carmela L. Domocmat, RN, MSN
- 43. Phimosis Paraphimosis Maria Carmela L. Domocmat, RN, MSN
- 44. Abnormal Findings Penile Trauma: Human Bite Trauma- Trauma-induced Fistula Glanular Amputation Penile Strangulation Blast Injury
- 45. Human Bite Trauma- Trauma-induced fistula Urethro-cutaneous fistula developed as a result of circumcision injury Maria Carmela L. Domocmat, RN, MSN
- 46. Glanular Penile Amputation Strangulation Complete loss of the glans In this child, a penile resulting from electrocautery strangulation injury was injury during a circumcision caused by a rubber band. Maria Carmela L. Domocmat, RN, MSN
- 47. Blast Injury results in no salvageable testicular tissue Gunshot Wound through the right thigh and penis Maria Carmela L. Domocmat, RN, MSN
- 48. Penile Diseases
- 49. Diseases Tinea Cruris Urethritis Syphilitic Chancre Chancroid Condyloma acuminatum or genital warts Herpes Candidiasis Donovanosis or granuloma inguinale Lypmphogranuloma Venereum Penile Tumor and Cancer Maria Carmela L. Domocmat, RN, MSN
- 50. Tinea Cruris or Jock itch Maria Carmela L. Domocmat, RN, MSN
- 51. Balanitis Balanitis gangraenosa Marked inflammation of the head of the penis This patient was diagnosed with balanitis and foreskin, in this case caused by fungal gangraenosa, which was first thought to be a dermatitis syphilis infection infection. Maria Carmela L. Domocmat, RN, MSN .
- 52. Syphilitic Ulcer Syphilitic Chancre Maria Carmela L. Domocmat, RN, MSN
- 53. Condyloma Penile acuminatum Condyloma or Genital Warts Growth at edge of glans due to HPV infection Maria Carmela L. Domocmat, RN, MSN
- 54. Secondary Syphilis: includes multiple lesions located on the penis and scrotum. Secondary syphilis is the most contagious of all the stages, and is The secondary characterized by maculopapular rash a systemic usually causes no spread of the itching, and can Treponema appear as the pallidum chancre, or bacterium. chancres found during the primary stage of syphilis are healing, or several weeks after the chancres have healed. Maria Carmela L. Domocmat, RN, MSN
- 55. Chancroid . The differential diagnosis proved to be chancroid, caused by Haemophilus ducreyi, and not syphilis. Maria Carmela L. Domocmat, RN, MSN
- 56. Genital Herpes Candidiasis Maculopapular herpetic rash on the penile shaft and corona of the glans penis. Maria Carmela L. Domocmat, RN, MSN
- 57. Donovanosis, or Lymphogranulom granuloma a venereum inguinale A “genital ulcerative disease” caused by the intracellular Gram- negative bacterium Calymmatobacterium granulomatisL. Domocmat, RN, MSN Maria Carmela
- 58. Penile tumor Penile Cancer differentially diagnosed as giant condyloma of Buschke The erythematous patch on the glans penis and Löwenstein (GCBL) was diagnosed as Bowen's disease, or squamous cell carcinoma in situ. Maria Carmela L. Domocmat, RN, MSN
- 59. Urethra
- 60. Inspection • Note the location of the urethral meatus. • Observe for discharge. • Obtain a culture of any discharge. Maria Carmela L. Domocmat, RN, MSN
- 61. Normal Findings • Central • At the distal tip of the glans • Opening is glistening, smooth and pink • Slit-like Slit- • No discharge present • Nontender Maria Carmela L. Domocmat, RN, MSN
- 62. Compression of the glans to open the urethral meatus • Hold the glans between the thumb and the forefinger and gently squeeze to expose the meatus. Maria Carmela L. Domocmat, RN, MSN
- 63. • If a discharge is seen, a culture should be taken • If the client complains of penile discharge but none is present, ask the client to milk the penis from the shaft to the glans. This maneuver may express a discharge that can be cultured. Maria Carmela L. Domocmat, RN, MSN
- 64. Abnormal Findings Hypospadias Epispadias Urethritis
- 65. Hypospadias The termination of the urethra is on the ventral surface of the penis Categorized as glandular (involving the glans penis), penile, or perineoscrotal Maria Carmela L. Domocmat, RN, MSN
- 66. Maria Carmela L. Domocmat, RN, MSN
- 67. Epispadias The opening of the urethra is on the dorsal surface of the penis Maria Carmela L. Domocmat, RN, MSN
- 68. Chemical Urethritis Nonspecific Urethritis This 44-year-old man developed several itchy red scaly patches on the glans and distal penile shaft and a clear urethral discharge shortly after the application of a spray before sex used to delay ejaculation. Screening studies for sexually transmitted diseases were negative and contact dermatitis and chemical urethritis were diagnosed. Maria Carmela L. Domocmat, RN, MSN
- 70. Inspection • Displace the penis to one side in order to inspect the scrotal skin. • Lift up the scrotum to inspect the posterior side. • Observe for lesions, inflammation, swelling, and nodules. • Note the size and shape. Maria Carmela L. Domocmat, RN, MSN
- 71. • The client should stand with legs slightly spread apart. • Have the client perform the Valsalva maneuver. • Observe for any mass of dilated testicular veins in the spermatic cord above and behind the testes. Maria Carmela L. Domocmat, RN, MSN
- 72. Normal appearance of the scrotum in an adult male Maria Carmela L. Domocmat, RN, MSN
- 73. Normal Findings • Skin of the scrotum is normally loose. • Surface may be coarse • Size varies, may appear pendulous Maria Carmela L. Domocmat, RN, MSN
- 74. Normal Findings (cont’d) • Skin color: often more deeply pigmented than body skin. Often reddened in red-haired red- individuals. • Sac is divided in half by septum. Maria Carmela L. Domocmat, RN, MSN
- 75. Normal Findings (cont’d) • Left scrotal sac may be longer than right • Contracts in cold temperature; relaxes in warm temperature. • Deeply pigmented • Hairless or with infrequent hair Maria Carmela L. Domocmat, RN, MSN
- 76. Normal Findings (cont’d) • Rugose surface • Nontender • Thin loose skin over muscular layer • No Pitting. Maria Carmela L. Domocmat, RN, MSN
- 77. Normal Findings (cont’d) • If scrotal mass or enlargement is detected, the scrotum should be auscultated and transilluminated Maria Carmela L. Domocmat, RN, MSN
- 78. Normal Findings (cont’d) Geriatric Variation : scrotal sac may appear elongated or more pendulous • Elderly clients sometimes have a problem of sitting on the scrotum resulting in trauma or excoriation of the surface Maria Carmela L. Domocmat, RN, MSN
- 80. Abnormalities Scrotum and its Structures Sebaceous Cyst Varicocele Cryptorchidism Elephantiasis Prepenile Scrotum Carcinoma Orchitis Testicular Torsion Scrotal Edema Testicular Lump Hydrocele Epididymitis Spermatocele Maria Carmela L. Domocmat, RN, MSN
- 81. Sebaceous Cyst Orchitis on Scrotum Maria Carmela L. Domocmat, RN, MSN
- 82. Cryptorchidism Prepenile scrotum (PPS) also known as Penoscrotal Transposition Maria Carmela L. Domocmat, RN, MSN
- 83. Scrotal Edema Maria Carmela L. Domocmat, RN, MSN
- 84. Hydrocele Maria Carmela L. Domocmat, RN, MSN
- 85. Elephantiasis of the Scrotum Maria Carmela L. Domocmat, RN, MSN
- 86. Carcinoma of the Scrotum Maria Carmela L. Domocmat, RN, MSN
- 88. Testicular Palpation • Between the thumb and the first two fingers, gently palpate the left testicle • Note the size, shape, consistency, presence of masses. Maria Carmela L. Domocmat, RN, MSN
- 89. Testicular Exam • Palpate the epididymis Note the consistency and presence of tenderness or masses. Maria Carmela L. Domocmat, RN, MSN
- 90. Testicular Exam (cont’d) • Between the thumb and the first two fingers, palpate the spermatic cord from the epididymis to the external ring Note the consistency and presence of tenderness or masses. Maria Carmela L. Domocmat, RN, MSN
- 91. Normal Findings Testicle: • Present in each sac • Left testis may normally lower than the right • Approximately: 4 x 3 x 2 cm (1 ½ x 1 x ¾ inches). Maria Carmela L. Domocmat, RN, MSN
- 92. Normal Findings Testicle: (cont’d) • Mildly sensitive to gentle/ moderate compression but not tender • Equal in size • Firm but not hard Maria Carmela L. Domocmat, RN, MSN
- 93. Normal Findings Testicle: (cont’d) • Smooth, rubbery, ovoid in shape, and free from nodules • Movable • Geriatric Variation : testes may feel slightly softer and smaller. Maria Carmela L. Domocmat, RN, MSN
- 94. Let’s Watch: Palpating the Testes and Related Structures
- 95. Abnormal Finding Testicular Lump
- 96. Testicular Lump Maria Carmela L. Domocmat, RN, MSN
- 97. Normal Findings Epididymis: • Comma shaped and distinguishable from the testicle. • Nontender, resilient Maria Carmela L. Domocmat, RN, MSN
- 98. Normal Findings Epididymis: (cont’d) • Usually located on posterolateral surface of each testis • Discretely palpable, smooth Maria Carmela L. Domocmat, RN, MSN
- 99. Normal Findings Epididymis: (cont’d) • Insensitive to pressure • Lies towards the top and back of each testis Maria Carmela L. Domocmat, RN, MSN
- 100. Abnormal Finding Epididymitis
- 101. Epididymitis Maria Carmela L. Domocmat, RN, MSN
- 102. Normal Findings Spermatic cord: cord: • Smooth and round • Located above each testicle • Composed of vas deferens testicular artery/vein, ilio- ilio-inguinal nerve. Maria Carmela L. Domocmat, RN, MSN
- 103. Normal Findings Spermatic cord: cord: • Lies along the posterior aspect of the bundle • Feels firm and wire- wire-like Maria Carmela L. Domocmat, RN, MSN
- 104. Normal Findings Spermatic cord: cord: • Nontender, movable • Discretely palpable from epididymis to external inguinal ring Maria Carmela L. Domocmat, RN, MSN
- 105. Normal Findings Spermatic cord:(cont’d) cord: • Smooth and cordlike, without nodules or swelling • You will normally be unable to specifically identify the remaining structures. Maria Carmela L. Domocmat, RN, MSN
- 106. Abnormal Findings Spermatocele Varicocele
- 107. Spermatocele Maria Carmela L. Domocmat, RN, MSN
- 108. Varicocele Maria Carmela L. Domocmat, RN, MSN
- 109. Maria Carmela L. Domocmat, RN, MSN
- 110. Assess for Cremasteric Reflex
- 111. Assess for Cremasteric reflex • Cremasteric reflex – the temporary migration of the testis •the cremaster muscle surrounding the testes contracts in response to such stimuli as cold air, cold water, or touching the inner thigh. This contraction raises the contents of the scrotum toward the inguinal canal) Maria Carmela L. Domocmat, RN, MSN
- 112. Assess for Cremasteric reflex cont’d Stroke the inner thigh with the handle of a reflex hammer Maria Carmela L. Domocmat, RN, MSN
- 113. Normal Finding • Testicle and scrotum rise on the stroked side Maria Carmela L. Domocmat, RN, MSN
- 114. Abnormal Finding Testicular torsion
- 115. Testicular torsion Maria Carmela L. Domocmat, RN, MSN
- 116. Advanced Techniques
- 117. Auscultation * Performed when a scrotal mass is found on inspection or palpation. • Place the client in a supine position. • Stand at the client’s right side at the genital area. • Place the stethoscope over the scrotal mass. • Listen for the presence of bowel sounds. Maria Carmela L. Domocmat, RN, MSN
- 118. Normal Finding • No bowel sounds are present in the scrotum. Maria Carmela L. Domocmat, RN, MSN
- 119. Abnormal Findings Hernia
- 120. Transillumination
- 121. Transillumination * Performed when a scrotal mass is found on inspection or palpation. • Tell the patient what you are going to do and inform that it is not be painful. • Darken the room. Maria Carmela L. Domocmat, RN, MSN
- 122. Transillumination (cont’d) • Light the unaffected side behind the scrotum and direct it forward. • Light the side of the scrotal enlargement or mass. Note whether there is a transmission of a red glow. Maria Carmela L. Domocmat, RN, MSN
- 123. Normal Finding Normal testicle does not illuminate (i.e., there is no glow) Maria Carmela L. Domocmat, RN, MSN
- 124. Abnormal Findings (+) transillumination: transillumination: Serous Fluid such as in Hydrocele and Spermatocele (-) transillumination: transillumination: Vascular structures such as in Varicocele, Varicocele, Hernia, Epididymitis and Tumor
- 125. Varicocele Hydrocele Maria Carmela L. Domocmat, RN, MSN
- 126. Inguinal Region
- 127. Inspection • If the client is at supine, ask the client to stand. • Stand or sit facing the client. • Observe for swelling or bulges. • Ask the client to bear down. • Observe for swelling or bulges. Maria Carmela L. Domocmat, RN, MSN
- 128. Normal Findings • Inguinal area is free from any swelling or bulges. Maria Carmela L. Domocmat, RN, MSN
- 129. Palpation of Lymph Nodes • With the index and middle fingers of the right hand, palpate the skin overlying the inguinal and femoral areas for lymph nodes. Maria Carmela L. Domocmat, RN, MSN
- 130. Palpation of Lymph Nodes Note the size, consistency, tenderness, and mobility. Maria Carmela L. Domocmat, RN, MSN
- 131. Normal Findings • Movable • Small, size of pea or baked bean • Nontender • Typically less than 1 cm in diameter (Note: Do not confuse Poupart’s ligament with enlarged lymph nodes) Maria Carmela L. Domocmat, RN, MSN
- 132. Palpation for Indirect Inguinal Hernia • Ask the patient to bear down while you palpate the inguinal area. • Place the right index finger in the client’s right scrotal sac above the right testicle and invaginate the scrotal skin. • Follow the spermatic cord until you reach a triangular, slitlike opening (the external inguinal ring). Maria Carmela L. Domocmat, RN, MSN
- 133. Examination for an Hernia Maria Carmela L. Domocmat, RN, MSN
- 134. Palpation for Indirect Inguinal Hernia • If the inguinal area is large enough, continue to advance the finger along the inguinal canal and ask the client to turn his head and cough. Note any masses felt against the finger. • Repeat on the left side using the left hand to perform the palpation. Maria Carmela L. Domocmat, RN, MSN
- 135. Normal Findings • Finger follows spermatic cord upward to triangular slitlike opening. (Which may or may not admit finger). Maria Carmela L. Domocmat, RN, MSN
- 136. Normal Findings As the client strains, no bulging will be felt against fingertips; a tightening around the finger is normal. Maria Carmela L. Domocmat, RN, MSN
- 137. Palpation for Femoral Hernia •Palpate the femoral canal. •Ask the client to bear down. Maria Carmela L. Domocmat, RN, MSN
- 138. Normal Findings • No bulging or swelling • Abdominal muscle tightens and scrotum lowers as client bears down. Maria Carmela L. Domocmat, RN, MSN
- 139. Let’s Watch: Palpating for Hernia
- 140. Abnormal Finding Hernia
- 141. Large Right Indirect Inguinal Hernia Maria Carmela L. Domocmat, RN, MSN
- 142. Left Inguinal Hernia Maria Carmela L. Domocmat, RN, MSN
- 143. Direct Inguinal Femoral Hernia Hernia Maria Carmela L. Domocmat, RN, MSN
- 144. Giant Scrotal Hernia Maria Carmela L. Domocmat, RN, MSN