![AHFS : NOT VERIFIED
Similarities and differences between acute MI & AHFS in
hospitalization in the US
Incidence 1 million per year 1 million per year
Mortality
Pre hospitalization
In hospital
After discharge [ 60-90 d]
High
3-4%
2%
?
3-4%
10%
Myocardial injury Yes Likely
Pathophysiological target Clearly defined
[coronary thrombosis]
Uncertain
Clinical benefits of
interventions in published
clinical trial
Beneficial Minimal / no benefit or
deleterious compared with
placebo
ACC / AHA recommendation LEVEL A NONE
2](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Acute Decompensated Heart Failure
Ähnlich wie Acute Decompensated Heart Failure (20)
Mehr von drucsamal
Mehr von drucsamal (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Acute Decompensated Heart Failure
- 1. Prof. U. C. SAMAL MD, FICC, FACC, FIACM, FIAE, FISE, FISC, FAPVS Ex- Prof. Cardiology & Ex-HOD Medicine Patna Medical College, Patna, Bihar Past President, Indian College of Cardiology Permanent & Chief Trustee, ICC-Heart Failure Foundation National Executive Member, Cardiological Society of India President, CSI Bihar Acute Decompensated Heart Failure : What Is New ? 1
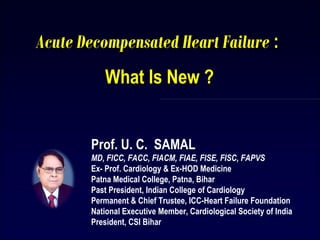
- 2. AHFS : NOT VERIFIED Similarities and differences between acute MI & AHFS in hospitalization in the US Incidence 1 million per year 1 million per year Mortality Pre hospitalization In hospital After discharge [ 60-90 d] High 3-4% 2% ? 3-4% 10% Myocardial injury Yes Likely Pathophysiological target Clearly defined [coronary thrombosis] Uncertain Clinical benefits of interventions in published clinical trial Beneficial Minimal / no benefit or deleterious compared with placebo ACC / AHA recommendation LEVEL A NONE 2
- 3. Acute Heart Failure Syndrome(s) • Acute heart failure (AHF) is defined as a rapid onset or change in the signs and symptoms of HF, resulting in the need for urgent therapy. • Symptoms are primarily the result of severe pulmonarycongestion due to elevated left ventricular (LV) filling pressures(with or without low cardiac output). • AHFS can occur in patientswith preserved or reduced ejection fraction (EF). • Concurrentcardiovascular conditions such as coronary heart disease (CHD),hypertension, valvular heart disease, atrial arrhythmias, and/or noncardiac conditions (including renal dysfunction, diabetes,anemia) are often present and may precipitate or contributeto the pathophysiology of this syndrome 3 ESC Guidelines
- 4. Mortality % Frontiers in Cardiovascular Medicine EHJ 2010:31;784-793 4 Mortality in AHFS
- 5. Proposed classification for patients who present with acute heart failure syndromes ACCF/AHA stage Explanation of stage Worsening chronic HF (75%) Stage C C: structural heart disease with prior or current symptoms of HF Advanced HF (5%) Stage D D: refractory HF requiring specialized interventions De novo HF (20%) Stage B most common, but also Stage A Also neither A nor B B: structural heart disease but without signs or symptoms of HF A: at high risk for HF but without structural heart disease or symptoms of HF 5 Frontiers in Cardiovascular Medicine EHJ 2010:31;784-793
- 6. • diuretics • ultrafiltration Vasodilators • nitroglycerin • nesiritide • nitroprusside INOTROPES • dobutamine • dopamine • levosimendan • nitroprusside Fluid retention or redistribution ? “dry out” “warm up & “dry out” Assessment of hemodynamic profile : therapeutic implications Adapted from Stevenson L W, Eur Heart j 6
- 7. HF Management: Principal changes from the 2008 guidelines o An expansion of the indication for mineralocorticoid receptor antagonists (MRAs) o A new indication for the sinus node inhibitor Ivabradine o An expanded indication for cardiac resynchronisation therapy (CRT) o New information on the role of coronary revascularisation in HF (PCI / CABG) o Recognition of the growing use of ventricular assist devices (LVAD) o The emergence of transcatheter valve interventions ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 7
- 8. Linking Short- term intervention with long-term benefit: What is needed? Better understanding of Acute Heart Failure pathophysiology MORTALITY • Myocardial injury [Tn release] • Renal dysfunction [CRS] • Liver dysfunction PREVENTION OF END- ORGAN DAMAGE Congestion Viable but dysfunctional myocardium Neurohormonal & inflammatory activation Mechanisms which can be targeted Metabolic factors Hemodynamic deterioration [↑LVFP,↓ CO, ↓ PERFUSION] Vascular resistance /stiffness ↑ ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012 Reviewed by Ponikowski
- 9. Neurohormones Norepinephrine Renin Angiotensin II Copeptin Endothelin Vascular system Homocysteine Adhesion molecules (ICAM, P-selectin) Endothelin Adiponectin C-type natriuretic peptide Inflammation C-reactive protein sST2 Tumor necrosis factor FAS (APO-1) GDF-15 Pentraxin 3 Adipokines Cytokines Procalcitonin Osteoprotegerin Myocardial stress Natriuretic peptides Mid-regional pro-adrenomedullin Neuregulin sST2 Myocardial injury Cardiac troponins High sensitivity cardiac troponins Myosin light-chain kinase 1 Heart-type fatty acid binding protein Pentraxin 3 Matrix and cellular remodeling Galectin-3 sST2 GDF-15 MMPs TIMPs Collagen propeptides Osteopontin Cardio-renal syndrome Creatinine Cystatin C NGAL ß-Trace protein Oxidative stress Oxidized LDL Myeloperoxidase Urinary biopyrrins Urinary and plasma isoprostanes Plasma malondialdehyde HF as a systemic illness & organ cross-talk 9 Nature Review Cardiology Vol.9 June 12 pg 349 And organ cross talk
- 10. Using Biomarkers across the ARC of Heart Failure Hospitalisation Therapy decisions Measure delta change Look for decline Obtain baseline Monitor therapy Present to ED Decisions on triage Determine prognosis In-hospital treatment Discharge Outpatient follow-up Therapy decisions Nov 1, 2013 - Dr Yancy interviews Drs Pang and Januzzi on the use of biomarkers ... Cardiac Intensive Care Unit, Massachusetts General Hospital, Boston,
- 11. BNP Status This pilot study demonstrates that home BNP testing is feasible and that trials using home monitoring for guiding therapy are justifiable in high-risk patients. Daily weight monitoring is complementary to BNP, but BNP changes correspond to larger changes in risk, both upward and downward. (Heart Failure [HF] Assessment with B-type Natriuretic Peptide [BNP] In the Home [HABIT]; NCT00946231)
- 12. Clinical RELEVANCE of promising novel biomarkers(AHFS) Biomarker Diagnosis Prognosis Therapy guidance Cardiac Production NT-proBNP and BNP ++++ ++++ ++ Solely Serum Sodium + +++ ++ No Serum Creatinine - +++ ++ No MR-proANP +++ ++++ Likely similar to NT- ProBNP/BNP Solely sST2 + ++++ ? Not Exclusively Hs troponin-I [EFFECT] + ++++ ? Solely MR-proADM - ++++ ? No Cystatin C - ++++ ? No NGAL - ++++ ? No GDF-15 - +++ ? Not Exclusively β- Trace protein - +++ ? No Gal-3 - +++ ? Not exclusively CRP - ++ ? No TNF-α - ++ ? No IL-6 - ++ ? No PTX3 - ++ ? Unknown MPO - ++ ? Not exclusively ET-1 - ++ ? Not exclusively Copeptin - ++ ? No PCT ++ ++ ++ No 12 Clinical Chemistry 58:1 127–138 (2012)
- 13. Pulmonary congestion evaluated by lung ultrasound predicts admission in pts with HF •97 HF outpts followed up during a period of 106 ± 12 days •21 hospitalizations for acute pulmonary edema •Multivariate analysis showed that pulmonary congestion assessed by lung ultrasound is strongest predictor of hospital admission Conclusion – in a HF outpt setting, B-lines assessment by lung ultrasound may help to identify pts who are most likely to decompensate
- 14. The four chest areas per side considered for complete eight zone lung ultrasound examination. These areas are used to evaluate for the presence of interstitial syndrome. Areas 1 and 2 denote the upper anterior and lower anterior chest areas, respectively. Areas 3 and 4 denote the upper lateral and basal lateral chest areas respectively. 14 Echo windows
- 15. Multiple reflections of ultrasound beams ultrasound beams ultrasound beams Comet-tails echographic image Normal echographic image horizontal lines Regular intervalReverberations Transducer Transducer Edematous Interlobular Septa Normal Interlobular Septa Ultrasound Comet-Tail Images: A Marker Of Pulmonary Edema A: Typical comet-tail artifacts: hyperechogenic, coherent vertical bundles with narrow basis spreading from the transducer to the further border of the screen. This artifact is composed of multiple microreflections of the ultrasound beam. A B B: Normal subject, with regular, parallel, roughly horizontal hyperechogenic lines due to the lung-wall interface. Chest. 2005;127(5):1690-1695. doi:10.1378/chest.127.5.1690 15
- 16. HF: Monitoring to predict/ prevent ADHF admissions • Devices: Externally applied Impedance Cardiography (PREDICT study 211 pts) • Internally placed devices measuring intra thoracic impedance(PARTNER 2HF: CRT device with Impedance monitoring): predicted subsequent admission for ADHF • PA / LA/ LVEDP monitoring devices Usefulness uncertain for mortality benefit 16
- 17. Heart Failure Risk Scores Circ HF 2013 End point: Death/ transplant/ Assist device • Heart Failure Survival Score(200pts): – IHD, QRS>120ms, LVEF, Resting HR, mean BP, O2 consumption, ser Na • Seattle Heart Failure model: (1100pts) – Age, LVEF, NYHA class, SBP, Diuretic dose, Na+, uric acid, ser. Chol., lymph. count - Sex, IHD, QRS >120ms, ICD, CRT, betablockers, ACEI, Statins, Allopurinol, • SHOCKED predictor: (900pts): Age>75, NYHA>II, AF, COPD, CKD, LVEF<20%, DM • PACE: (900 pts) PVD, Age >70, Creatinine >2, EF < 20%, • ADHERE registry( for acute mortality): SBP, Ser creatinine and BUN • Frankenstein: BNP , 6′WT
- 18. … We found that in a large, diverse contemporary HF population, risk assessment was strikingly similar across all LVEF categories. These data suggest that, although many HF therapies are uniquely applied to patients with reduced LVEF, individual prognostic factor performance does not seem to be significantly related to level of left ventricular systolic function. (Circ Heart Fail. 2013;6:635-646.)
- 19. AHF Treatment Goals Immediate [ED/ICU/CCU] •Treat symptoms and restore oxygenation •Improve hemodynamic and organ perfusion •Limit cardiac and renal damage •Prevent thromboembolism •Minimize length of ICU stay Intermediate [in –hospital] • stabilise pt and optimize treatment strategy •Initiate and up-titrate disease modifying pharmacologic therapy •Consider device therapy in appropriate pts • identify etiology and relevant comorbidities Pre-discharge and long term management •Plan follow up stratergy •Enroll in ds management programme, educate and initiate life style adjustments •Plan to up-titrate / optimise disease modifying pharmacologic therapy •Ensure assessed for appropriate device therapy •Prevent early readmission •Improve symptoms Http://www.Peerviewpress.Com/01/r286
- 20. 20 While pharmaceutical innovation has been highly successful in reducing mortality in chronic heart failure, this has not been matched by similar success in decompensated heart failure syndromes. Despite outstanding issues over definitions and end points, we argue in this paper that an unprecedented wealth of pharmacologic innovation may soon transform the management of these challenging patients. Agents that target contractility, such as cardiac myosin activators and novel adenosine triphosphate-dependent transmembrane sodium-potassium pump inhibitors, provide inotropic support without arrhythmogenic increases in cytosolic calcium or side effects of more traditional agents. Adenosine receptor blockade may improve glomerular filtration and diuresis by exerting a direct beneficial effect on glomerular blood flow while vasopressin antagonists promote free water excretion without compromising renal function and may simultaneously inhibit myocardial remodeling. Urodilatin, the renally synthesized isoform of atrial natriuretic peptide, may improve pulmonary congestion via vasodilation and enhanced diuresis. Finally, metabolic modulators such as perhexiline may optimize myocardial energy utilization by shifting adenosine triphosphate production from free fatty acids to glucose, a unique and conceptually appealing approach to the management of heart failure. These advances allow optimism not only for the advancement of our understanding and management of decompensated heart failure syndromes but for the translational research effort in heart failure biology in general.
- 21. 21 The main stay of AHF Therapy
- 22. Some new therapeutic agents for acute heart failure and their potential targets Agent For patients with these clinical features Diuretics, vasopressin antagonists, adenosine antagonists Patients with signs of fluid overload, high BNP Vasodilators Normal to high SBP, high BNP Inotropes Low SBP, signs of Hypoperfusion Renal preservation agents Renal dysfunction Myocardial protection agents CAD, or ongoing ischaemia 22
- 23. Short- and long-term novel therapies for AHF syndromes Short term Long term Both Levosimendan [LIDO, CASINO, SURVIVE] ? ? Nesiritide[ ASCEND-HF, ROSE-AHF] Relaxin [RELAX-AHF] Myosin Activators Omecamtiv Mecarbil [ATOMIC-AHF] RyR2 stabilizers/ rycals Cinaciguat (UIT) Adenosine regulating agents Stresscopin Istaroxime [HORIZON-HF] Ularitide [TRUE-AHF, SIRIUS II, URGENT] Urocrotins [UNICORN] Hypertonic Saline Ultrafiltration [RAPID-CHF, UNLOAD] IABP EECP [PEECH] CAFA IMT Direct renin Inhibitors (DRI) [ASTRONAUT] Macronutrients Micronutrients CRT/AICD Adenosine Antagonists [PROTECT, REACH UP rolofylline] Vasopressin Antagonists [EVEREST, TACTICS-HF] Digoxin [DIG] CD-NP Frontiers in Cardiovascular Medicine EHJ 2010:31;784-793 modified 2013 23
- 24. Newer Drugs/Devices and targeted Therapy Group A • Managing fluids • Preserving renal function Group B • Contractility • Diastole/ Vascular Resistance Group C • Vasomotion 24
- 25. Group A Managing fluids Preserving renal function 25
- 26. • Loop diuretics are an essential component of therapy for patients with acute decompensated heart failure, but there are few prospective data to guide their use. • In a prospective, double-blind, randomized trial, we assigned 308 patients with ADHF to receive furosemide administered intravenously by means of either a bolus every 12 hours or continuous infusion and at either a low dose (equivalent to the patient’s previous oral dose) or a high dose (2.5 times the previous oral dose). • DOSE Trial: Among patients with ADHF, there were no significant differences in patients’ global assessment of symptoms or in the change in renal function when diuretic therapy was administered by bolus as compared with continuous infusion or at a high dose as compared with a low dose. • Low dose dopamine increases GFR and RBF. DAD-HF investigated 60 pts randomized to low dose furosemide (continuous infusion 05 mg/hr) and 5 µg/kg/min per eight hours was found effective in terms of dyspnoea relief with improved renal function. High dose combination though was equally effective caused WRF . 20 mg/hr F + 5µg/kg/min Dopamine. Furosemide 26
- 27. • The study tests the hypothesis that in patients admitted with acutely decompensated heart failure (ADHF), achievement of adequate body hydration status with intensive medical therapy, modulated by combined bioelectrical vectorial impedance analysis (BIVA) and B-type natriuretic peptide (BNP) measurement, may contribute to optimize the timing of patient’s discharge and to improve clinical outcomes. • 300 ADHF pts underwent serial BIVA and BNP measurement. Therapy was titrated to reach a BNP value of 250 pg/ml, whenever possible. • Our study confirms the hypothesis that combined BNP/BIVA sequential measurements help to achieve adequate fluid balance status in patients with ADHF and can be used to drive a ‘‘tailored therapy,’’ allowing clinicians to identify high-risk patients and possibly to reduce the incidence of complications secondary to fluid management strategies. 27
- 28. Ultrafiltration 28 • UNLOAD(200pts): • superior to diuretics as it reduces volume at a rate more than 500 ml/hr which is Isotonic ultrafiltrate (both salt and water) • UF leads to a lower plasma renin, norepinephine and aldosterone levels as compared to diuretics. • CARESS study: High risk ADHF pts.: Similar outcome for weight reduction, but higher rise in ser creatinine, need for dialysis, and other adverse events…. UF a new therapy as primary beyond diuresis resistance in ADHF?? • AVOID HF: Ongoing trial (to be completed in 2016) J Am Coll Cardiol 2012:59:2145-53
- 29. Investigational drugs in ADHF Adenosine A1 receptor antagonist: Rolofylline • A1 receptor blockade results in afferent arteriolar vasodilation which leads to improved GFR and enhanced diuresis and natriuresis without activation of tubuloglomerular feedback. • Preserve GFR, improve diuresis, increase sodium excretion by kidney. • Phase 2 trial: better relief of dyspnoea and lesser renal dysfunction. • Phase 3 trial: PROTECT:2033 pts.: negative trial with none of the primary end points significant and safety was questioned due to neurological side effects: seizure and stroke. 29
- 30. • Small studies have indicated that adenosine A1 receptor antagonists enhance diuresis and may improve renal function in patients with chronic heart failure or AHF. • 2,033 AHF pts, volume overload, eCrCl 20 - 80 ml/min, and elevated BNP randomized (2:1) within 24 h of hospital presentation to rolofylline 30 mg/day or intravenous placebo for up to 3 days. • In this large, phase III clinical trial, the adenosine A1 receptor antagonist rolofylline did not prevent persistent worsening renal function in AHF patients with volume overload and renal dysfunction. Rolofylline 30 SCr↑ BUN↑
- 31. •Effects of rolofylline on endpoints in relation to baseline renal function. •The secondary morbidity/mortality endpoint, the risk of death or cardiovascular or renal rehospitalization through day 60, was lower in the rolofylline group compared with the placebo group only in patients with a baseline eCrCl 30 ml/min (hazard ratio: 0.64; 95% CI: 0.43 to 0.95), but not in the other subgroups Rolofylline 31
- 32. Group B Contractility Diastole/ Vascular Resistance 32
- 33. Levosimendan enhances contractility by increasing responsiveness of myofilaments to calcium. The cardiac myosin activator Omecamtiv mecarbil stimulates myosin adenosine triphosphatase (ATPase), thereby increasing force generation. Istaroxime inhibits activity of plasma membrane sodium-potassium ATPase and increases the activity of sarcoplasmic/endoplasmic reticulum calcium ATPase (SERCA). Mechanism of action of novel contractility-enhancing medications. Omecamtiv mecarbil (Modified from Tavares M, Rezlan E, Vostroknoutova I, et al. New pharmacologic therapies for acute heart failure. Crit Care Med 2008; 36[Suppl]:S112-S120.) 33 Istaroxime Levosimendan
- 34. Omecamtiv Mecarbil (OM) is a Novel Selective Cardiac Myosin Activator Malik Fl, et al. Science 2011; 331:1439-43 Teerlink JR, et al. Lancet 2011; 378:667-75; Cleland JGF, et al. Lancet 2011; 378:676-83 Mechanochemical Cycle of Myosin • • Increases duration of systole • Increases stroke volume • No Increase in myocyte calcium • No change in dp/dtmax • No increase in MVO2 ATOMIC-AHF Phase 2; 613 pts .X 48 hrs random IV dose 115; 230; 310 ng/ml. ATOMIC-AHF Phase 2; 613 pts .X 48 hrs random IV dose 115; 230; 310 ng/ml. COSMIC-HF chronic oral therapy; oral alone or IV to oral transition. COSMIC-HF chronic oral therapy; oral alone or IV to oral transition. Omecamtiv mecarbil increases the entry rate of myosin into the tightly- bound, force-producing state with actin “More hands pulling on the rope” 34
- 35. Study Design: Sequential Dosing Cohort Cohort 1 Cohort 2 Cohort 3 Omecamtiv Placebo 1:1 Randomization (n≈200) Omecamtiv Placebo 1:1 randomization (n≈200) Placebo Omecamtiv 1:1 randomization (n≈200) DMC DMC Cohort 1 Cohort 2 Cohort 3 15 mg/hr @ 0-4 hr 3 mg/hr @ 4-48 hr Target: 230 ng/mL Cmax: 75-500 ng/mL SET: ~8-55 msec 20 mg/hr @ 0-4 hr 4 mg/hr @ 4-48 hr Target: 310 ng/mL Cmax: 125-700 ng/mL SET: ~14-78 msec 7.5 mg/hr @ 0-4 hr 1.5 mg/hr @ 4-48 hr Target: 115 ng/mL Cmax: 30-250 ng/mL SET: ~3-28 msec Pharmacokinetic simulations Teerlink JR, et al. Lancet 2011; 378: 667–75; Cleland JGF, et al. Lancet 2011; 378: 676–83.
- 36. ATOMIC –AHF Omecamtiv Mecarbil Dyspnea Response Teerlink J R ESC 2013, Symposium 4503 Response rate ratio 1.02 1.02 1.41 95% CI [0.74 -1.42] [0.76 – 1.37] [1.02 -1.93] Response rate ratio : ratio of response rate to placebo with each cohort
- 37. Omecamtiv Mecarbil : time dependent changes in echocardiogram measures Http://www.Peerviewpress.Com/01/r286
- 38. • Efficacy – OM did not meet the 1° endpoint of dyspnoea relief – Appeared to improve dyspnoea in Cohort 3 – Trends towards reduction of worsening HF • Safety – Overall SAE profile and tolerability similar to placebo – Increase in troponin; no clear relationship to OM concentration – Numerical imbalance in MIs in Cohort 3 – No evidence of pro-arrhythmia • Pharmacology – PK similar to healthy volunteers and stable HF patients – Systolic ejection time significantly increased consistent with MOA – Small fall in heart rate & rise in systolic BP at higher doses ATOMIC- AHF Summary Though at present investigational the drug of the future in AHF Janccin B: New Heart failure inotrope could be ‘Holy Grail’. IMNG Medical Media September 5, 2013 John J. V. McMurray et al, on behalf of the ATOMIC-AHF Investigators and Patients
- 39. • Istaroxime is a novel intravenous agent with inotropic and lusitropic properties related to inhibition of Na/K adenosine triphosphatase (ATPase) and stimulation of sarcoplasmic reticulum calcium ATPase. • 120 AHF pts and reduced systolic function. Three sequential cohorts of 40 patients each were randomized 3:1 istaroxime:placebo to a continuous 6-h infusion. The first cohort received 0.5 g/kg/min, the second 1.0 g/kg/min, and the third 1.5 g/kg/min istaroxime or placebo. • In patients hospitalized with HF, istaroxime improved PCWP and possibly diastolic function. In contrast to available inotropes, istaroxime increased SBP and decreased HR. Istaroxime Mihai Gheorghiade et al JACC 2008:03;015 39 [HORIZON-HF Trial]
- 40. •Urocortins are a recently discovered group of peptide hormones of the corticotropin releasing factor family. They bind with a strong affinity to the CRH-R2 receptor, which is highly expressed in the myocardium and in the vascular endothelium. •Urocortins exhibit potent inotropic and lusitropic effects on rat and sheep hearts and activates a group of myocyte protective pathways collectively known as ‘reperfusion injury salvage kinase’. •In healthy humans show that brief intravenous infusions of urocortin 2 in healthy humans induce pronounced dose-related increases in cardiac output, heart rate, and left ventricular ejection fraction while decreasing systemic vascular resistance; similar effects were seen in HF patients. Urocortins 40
- 41. Stresscopin Human stresscopin is a corticotropin-releasing factor type 2 receptor selective agonist and a member of the CRF peptide family. Stimulation of CRFR2 improves cardiac output and LVEF. 62 pts with HF and LVEF ≤ 35% were instrumented with a pulmonary artery catheter and randomly assigned (ratio 3:1) to receive an intravenous infusion of stresscopin or placebo. The main study was an ascending dose study of three doses (5, 15, and 30 ng/kg/min) of study drug or placebo administered in sequential 1 h intervals (3 h total). Statistically significant increases in CI and reduction in SVR were observed with both the 15 ng/kg/min (2 h time point) and 30 ng/kg/min (3 h time point) doses of stresscopin without significant changes in HR or SBP. No statistically significant reductions in PCWP were seen with any dose tested in the primary analysis, although a trend towards reduction was seen. In HF patients with reduced LVEF and CI, ascending doses of stresscopin were associated with progressive increases in CI and reductions in SVR without significant effects on PCWP, HR, or SBP. 41
- 43. Vaso active drugs in ADHF Relaxin: Serelaxin • A recombinant human relaxin -2- a naturally occurring peptide that regulates maternal adaptations • RELAX AHF:1160 pt. of ADHF with preserved SBP >115 mmHg. • Serelaxin 30 ug/kg/day x48 hrs or Placebo • Significant improvement in dyspnoea scale • No impact on short term mortality/ HF readmission at 60 days, though 180 day mortality was significantly lower. • Hypotensive episodes higher but renal dysfunction less than placebo group • No limitation: dobutamine milrinone (increase intercellular calcium in myocytes leading to tachycardia and arrhythmias, levosimendon calcium sensitiser causes atrial and ventricular arrhythmias, and like milrinone may be limited by hypotension. • FDA grants Breakthrough Therapy designation to Novartis' serelaxin (RLX030) for acute heart failure. 43
- 44. Biology of Relaxin and Potential Beneficial Effects in HF Teichman SL, Unemori E, Teerlink JR, Cotter G, Metra M - Curr Heart Fail Rep (2010) Endogenous peptide associated with pregnancy, and acts through relaxin receptor: reduce inflammation, decrease fibrosis, attenuate ventricular remodeling, increase vasodilation, promote renal blood flow, increase vascular endothelial growth factor, and angiogenesis. ↓Inflammation↓Inflammation ↓Fibrosis↓Fibrosis ↑Vasodilation↑Vasodilation Renal effectsRenal effects AngiogenesisAngiogenesis Relaxin ReceptorRelaxin Receptor RelaxinRelaxin Pregnancy associated endogenous peptide Relaxin ReceptorRelaxin 44
- 45. Pre-RELAX-AHF : Rapid dyspnea improvement through 24 hours [Likert Scale] Teerlink J R Lancet 2009,373:1429-1439
- 46. RELAX-AHF : Cardiovascular and All Cause Mortality Teerlink J R Lancet 2013, 381:29-39
- 47. RELAX-AHF : Biomarker Changes Metra M Et Al J Am Coll Cardiol 2013, 61: 196 -206
- 48. RELAX-AHF • 1161 pts with AHF • 19% improvement in dyspnea • Decreases in worsening HF • Improvement of in-hospital signs and symptoms of HF • Decreased length of hospital stay • No significant difference in second primary efficacy endpoint of the proportion of pts with dyspnea relief • No significant effect on secondary endpoints of cardiovascular death or hospital readmission for HF or renal failure [RELAX –AF was not powered as a mortality trial] Teerlink J R Lancet 2013, 381:29-39
- 49. Seralaxin • Increased renal function • Improved vascular compliance • Improved cardiac output Beneficial effects on dyspnea and post-discharge clinical outcomes
- 50. • Cinaciguat (BAY 58-2667) is a soluble guanylate cyclase (sGC, second messenger that internalizes the message carried by intercellular messengers such as peptide hormones and NO) activator that is being developed as a first-in-class treatment for acute decompensated heart failure (ADHF). It acts independently of the sGC ligand nitric oxide. • Cardioprotective effects in animal models, and pilot clinical studies found that it was well tolerated, unloaded the heart and increased cardiac output. • This placebo-controlled, randomized, double-blind, multicenter, international phase IIb study investigated the safety and efficacy of intravenous cinaciguat (per-protocol) as add-on to standard therapy in 139 patients with ADHF (NYHA functional class III and IV; pulmonary capillary wedge pressure [PCWP] ≥ 18 mmHg). • Cinaciguat rapidly and significantly reduced PCWP and PVR and increased cardiac output in patients with ADHF, without impairing cardiac or renal function. Hypotension occurred in some patients; further dose titration studies are therefore required to establish the optimal dosing strategy for this promising new therapy. Cinaciguat JACC Mar 9,2010 Vol:55 issue 10A 50
- 51. These molecules have been engineered to combine the beneficial aspects of different natriuretic peptides into a single molecule while minimizing potentially negative actions. CD-NP is a combination of C-type natriuretic peptide (CNP) and Dendroapsis NP (DNP). Although lacking natriuretic effects, CNP is a more selective venodilator than BNP, thus reducing the risk of significant hypotension. On the other side, DNP possesses significant natriuretic activity, at the expense of possible hypotensive effects. The chimeric peptide CD-NP combines the favourable natriuretic effects of DNP with the venodilatory profile of CNP, reducing the risk for harmful side effects. Preliminary studies in AHFS patients are ongoing. Chimeric natriuretic peptides 51
- 52. Adenosine regulating agents •This new class of drugs, whose prototype is represented by acadesine, has been developed to mimic the protective effects of adenosine during ischaemia. •Acadesine exerts its pharmacological actions by increasing adenosine bioavailability and by activating 50adenosine monophosphate (AMP) signalling cascade via its metabolite 5-aminoimidazole-4-carboxamide riboside (ZMP). •The first mechanism leads to multiple anti-ischaemic effects (maintenance of endothelial function and vasodilation, inhibition of platelet aggregation and neutrophil activation), whereas the latter ameliorates glucose uptake and free fatty acid oxidation thus increasing ATP synthesis. Importantly, acadesine exerts its actions only in areas undergoing net ATP catabolism (such as ischaemic tissues) thereby avoiding potentially harmful peripheral vasodilator effects. Acadesine 52
- 53. • Nesiritide is approved in the United States for early relief of dyspnea in patients with acute heart failure. Previous meta-analyses have raised questions regarding renal toxicity and the mortality associated with this agent. • We randomly assigned 7141 patients [ASCEND-HF trial] • Co-primary end points were the change in dyspnea at 6 and 24 hours, and the composite end point of rehospitalization for heart failure or death within 30 days. • Nesiritide was not associated with an increase or a decrease in the rate of death and rehospitalization and had a small, nonsignificant effect on dyspnea when used in combination with other therapies. • It was not associated with a worsening of renal function, but it was associated with an increase in rates of hypotension. On the basis of these results, nesiritide cannot be recommended for routine use in the broad population of patients with acute heart failure. Nesiritide 53
- 54. Ularitide • Synthetic form of Urodilantin: human natriuretic peptide produced in kidney: induces natriuresis and diuresis. Also potent vasodilator( increases intracellular cyclic GMP) and increased renal blood flow) : Two double blind studies have shown favorable outcome in ADHF by symptom improvement and hemodynamics. • Phase 3 trial(TRUE-AHF >2110 pts) - ongoing study. 54
- 55. Summary• AHFS is a complex condition with heterogenous pathophysiology and varied etiology with unpredictable and often stormy course. • Present management rests on therapeutic optimisation of congestion, perfusion & protection against kidney injury & finally myocardial preservation and enhancement. Needless to point out, too much reliance on inotropics and pressor amines could be ominous. • Simplistic biometrics like HR, B.P. and eGFR are inexpensive and dependable. Measures of clinical assesment while BNP and other monitoring devices may be superior but often unaffordable and expensive and make HF management imposible. • The safe path on part of ED Physician is to follow updated guideline pathways till future breakthrough and safe newer drugs are available. • All stabilised discharged pts must have GDMT/ Devices/ revascularisation as could be indicated. Multi disciplinary care approach is inevitable at all stage. • Serelaxin, Omecamtiv Mecarbil , Istaroxime & Ularitide appear to be new drugs of the near future. • … Future trials conducted in aHFs must abandon the ‘one-sizefits- all’ approach in favor of an approach that takes into account the varied and distinct pathophysiologies of aHFs. 55
- 56. 56
- 59. (1) Symptom relief. (2) Measures of congestion relief (i.e. improvement in clinical signs). (3) Index hospitalization data (e.g. length of stay). (4) Prevention of end-organ damage (heart and kidney). (5) Post-discharge: death and rehospitalization data. Federal Drug Administration (FDA) Study Group as a general guide for choosing the components of the endpoints to be included when testing different types of drugs in different patient subgroups, although not all of them would be necessary in a single trial Position Statement European Journal of Heart Failure (2011) 59
Hinweis der Redaktion
- In HF patients with reduced LVEF and CI, ascending doses of JNJ-39588146 were associated with progressive increases in CI and reductions in SVR without significant effects on PCWP, HR, or SBP
- Furosemide is conventional volume reducing drug. There are some newer observation depicted by DOSE trial: High Vs Low / Bolus Vs continuous infusion. Further DAD- HF tells us High vs Low dose furosemide with low dose of dopamine equal effect in diuresis and dysponea relief but high dose furosemide causes WRF.
- In optimization of monitoring volume reduction a targeted approach with bio-electrical vectorial impedence anaysis with BNP measurement give us precise message as against regular clinical observation of fluid status, perhaps this will provide clinicians a drive for “ Tailor Therapy”
- Ultrafiltration though used in state of diuretic resistance and refractory Heart Failure, UNLOAD experience there is optimising , this may be first line application. With newer versions of equipment and easy peripheral venovenus connection this is apt to be used as OPD procedure with cardiac small need for anticoagualants.
- Rolofylline was identify as a drug which improves GFR enhance diuresis and natriuress without activation of TGF i.e. with afferent glomerular arteriolar vasodilation. In phase 3 trials drugs was questioned in 2033 patients failing to address none of the primary end points and loss of safety with neurological side effects like seizure and stroke it turned out to be a Negative trial.
- Obviously it shows secondary morbility and mortality endpoint as the risk of death and rehospitalisation due to cardiac or renal not favourable expect at sub-group the pts. With eGFR 30ml/min.
- This is a unified model to demonstrate the myo contractility enhancing mechanism of three principal drugs : Levosimendan judiciously used in Europe and Asia though not approved by FDA, USA. Two others are in pipeline:- Omecamtiv mecarbil amd Istaroxime. Omecamtiv mecarbil exerts a novel chemical mechanism to generate force and enhance contraction while istaroxime leads to SERCA activation leading into myocardial enhancement and contraction. None of the above drugs increase intracellular calcium nor oxygen demand by the myocyte i.e constractingly unique to conventional Inotropics agents which lead to ischemia arrhythemia and hypotension eminently the dobutamine milrinone
- So, dyspnoea response only significant in cohort 3 while though better not more significant in cohort 1 or 2.
- Echocardiographic evidence of improvement of myocardial performance in terms of systolic ejection time (SET) which is the characteristic therapeutic effect of OM. There is appreciated beneficial, in terms of systolic value change LVESV AND LVEDV.
- Finally in terms of relief of dysponea a reduction of worsening HF and myocardial enhancement without significant adverse effects OM is the future drugs of the HF as McMurray says this is a cloud with silver lining believably the star of the future in AHF care and as per IMNG Medical Media Observation an inotrope , no less a Holy Grail.
- Istaroxime as shown in the confluent diagram a having convincing mode of action. This is a unique drug which causes reduction of PCWP and possibly diastolic function in the contrast of available inotrope it shown a trend of increased SVB and decrease of HR which are the clinical marker of Heart Failure benefit. By ATPase inhibition and SERCA ATPase stimualation it exerts inotropic and lusitropic.
- Urocortins is a peptide harmone of CRH Family which is highly express in myocardial and vascular endothelial with I.V. Infusion in a healthy human it enhances Cardiac Output HR and LVEF while decrease in SVR. It pronounced Inotropic and lusitropic effects in the experimental animals and found interestingly activates a group of myocyte protective pathways known as the reperfusion injury salvagekines
- This is similar to Urocortin . This drug is studied by PaC monitoring with the graded dose by IV infusion in pts. Of reduced ejection fraction and Cardiac Index it causes progressive increased in CO & CI. With reduction in SVR. There is no effect on PCWP, HR or SBP. This study is small but very encouraging.
- This is considered to be a promisingly physiological therapy against the ADHF. Relaxin is pregnancy associated harmone which protect pregnant women against volume expansion with advancing pregnancy. Serelaxin is a recombinant, relaxin analog developed by Novartis. This is the only drug which has been given breakthrough status by FDA in AHF therapy.
- This is anti inflammatory anti fibrotic and renoprotective and enhances the vasomotion by angiogenese. This picture depicts the intricate pathways culminating in unique renoprotective action which is the considered to independent predictor of prognosis and outcome AHFS. Though it contributes a severally volume homeostatis.
- Proportion of the pts. At the dose of 30 mg/ day shows the benefit in dyspones relief in Likert scale which confirm to the conviction a similar administration of the single dose in ADHS in ED department would be very beneficial would suffice.
- In comparison to placebo benefits is seen in terms of myocardial injury / troponin – Myocardial stretch NT-proBNP- Acute Kidney injury Cystatin C . The graph is expressed in terms of comparative applicacy to bring it to down basal level.
- To read it out.
- Soluble guanylate cylase in smooth muscle cells is converted to CGMP with causes vasodilation. At high doses, a substantial decreases in SBP was noted, not associated with adverse effects on renal function, rehospitalisation or mortality.
- AHFS
- AHFS