

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Corneal neovascularization
Ähnlich wie Corneal neovascularization (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Corneal neovascularization
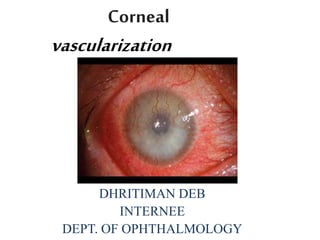
- 1. Corneal vascularization DHRITIMAN DEB INTERNEE DEPT. OF OPHTHALMOLOGY
- 2. definition • Corneal vascularization - in-growth of new blood vessels from the pericorneal plexus into avascular corneal tissue as a result of hypoxia i.e. oxygen deprivation. • Maintaining avascularity of the corneal stroma - An important aspect of corneal pathophysiology as it is required for corneal transparency and optimal vision.
- 4. Types • Superficial:- It involve the epithelium & anterior to Bowman’s layer with an arborizing pattern. • Deep:- It involve the stromal layer with radially oriented parallel channels.
- 5. Etiology:- • Contact lens • Infection like herpes simplex • Injury • Inflammation • Dystrophy • Degeneration or cancerous conditions
- 6. Pathogenesis: • Chemical theory There may be presence of vasostimulatory factor (VSF) or the breakdown (destruction) of previously existing vasoinhibitory factor (VIF). • Mechanical theory Blood vessels cannot invade normal cornea because of its compactness and loosening of the compactness of corneal tissue due to oedema was mandatory for neovascularization.
- 7. Symptoms:- • Decreased vision • Lacrimation • Redness • Photophobia • ‘Foreign body’ sensation • Pain • Visible ‘whiteness’ of the cornea
- 8. Signs:- • Loss of transparency & decrease in vision. • Circumcorneal congestion. • Loss of smoothness of the surface • Epithelial defect • Vascularization • Change in shape,thickness or curvature • Appearance of nodules or growth on the surface.
- 9. Treatment:- • Medical Options • Surgical Options
- 10. •Medical Options • If contact lens–related hypoxia is suspected, it is important to cease contact lens use while the NV is addressed. • Anti-inflammatory drugs. Topical administration of steroids and/or nonsteroidal anti-inflammatory drugs (NSAIDs) should be first-line treatment for corneal NV. These drugs are best administered within 24 hours following the initial corneal insult, before leukocyte infiltration and recruitment occurs.
- 11. • Anti-VEGF agents. Recent studies involving monoclonal anti-VEGF antibodies have shown promising results for the reduction of corneal NV. Topical and/or subconjunctival administration of bevacizumab or ranibizumab has demonstrated good short-term safety and efficacy. • MMP inhibitors. Under inflammatory conditions, suppression of enzymes that compromise corneal structural integrity may block corneal NV. The combination of orally administered doxycycline (a nonselective MMP inhibitor) plus topical corticosteroids has been shown to suppress neovascularization.
- 12. oSurgical Options:- • Laser ablation. Argon and Nd:YAG lasers may be used to occlude invading blood vessels by coagulating blood vessels and ablating tissue. Careful attention must be paid to avoid excessive irradiation and damage to adjacent tissues, as complications such as corneal hemorrhage and corneal thinning may develop. Failure due to vessel lumen reopening is common, and new shunt vessels may form.
- 13. • Photodynamic therapy. Irradiation of a previously injected photosensitive dye causes a reaction that produces reactive oxygen species in the vessel lumen, inducing apoptosis and necrosis of the endothelium and basement membrane. The highly specific tissue damage, combined with the resulting thrombogenic response, seals off the vessel. Although it is effective, photodynamic therapy has limited clinical acceptance due to high costs and potential complications related to laser irradiation and generation of reactive oxygen species.
- 14. • Diathermy and cautery. A fine needle may be inserted into feeder vessels at the limbus. Vessels are occluded either by application of a coagulating current through a unipolar diathermy unit or by thermal cautery using an electrolysis needle. Although initial studies found these techniques to be safe and effective
- 15. Thank you