Cementum
•
351 likes•71,215 views

This document provides an overview of cementum, including: - Its physical characteristics, composition, classification, and formation process (cementogenesis). - The cells involved in cementum formation and maintenance, including cementoblasts and cementocytes. - Its locations and junctions with other tissues like enamel and dentin. - The functions of cementum in anchoring teeth, adaptation, and repair. - Some developmental anomalies and abnormalities that can affect cementum.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cementum
Similar to Cementum (20)
Recently uploaded
Recently uploaded (20)
Cementum
- 1. Dr anirudh singh chauhan PG Ist year department of periodontology
- 2. CONTENTS •Introduction •Physical characteristics •Composition •Classification of cementum •Cementogenesis •Mineralization •Cementum associated cells •Cementoenamel junction •Cementodentinal junction •Functions of cementum •Developmental anomalies of cementum •Abnormalities of cementum •Conclusion
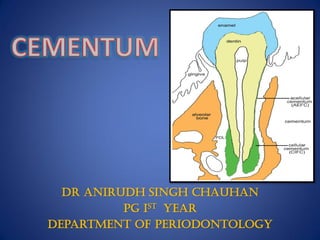
- 3. INTRODUCTION • Calcified, Avascular mesenchymal tissue that forms the outer covering of the anatomic root. Carranza 11th edition. • First demonstrated in 1835 by FRANKE & RASCHKOV, two pupils of purkinje. • Begins at the cervical portion of the tooth at the cementoenamel junction and continues to the apex. • Two main types- - Acellular ( primary) - Cellular ( secondary) • Both consist of interfibrillar matrix and collagen fibrils.
- 4. PHYSICAL CHARACTERISTICS • Hardness < Dentin. • Light yellow in color and lacks luster. • Lighter in color than dentin, however it may not be distinguished on basis of color alone. • Permeability of cellular cementum is greater than that of acellular cementum. With age, the permeability of cementum decreases. • Thinnest at CEMENTOENAMEL JUNCTION (20-50 um) • Thickest towards the APEX (150-200 um)
- 5. COMPOSITION • Dry weight basis: – 45-50% inorganic substances which consists of calcium and phosphate in the form of hydroxyapetite crystals. – 50-55% organic material and water. • Organic matrix of cementum consists of : – Type I collagen ( 90%) – Type III collagen ( 5% ) – Non collagenous proteins. • By volume: 45% inorganic 35% organic 20% water
- 6. • Two main sources of collagen fibers 1. Sharpeys fibers ( Extrinsic) are the embedded portion of the principal fibers of periodontal ligament and formed by fibroblasts. 2. Fibers that belong to the cementum matrix ( intrinsic) and produced by cementoblast. • Due to its lower crystallinity of mineral component : – has the highest Flouride content – Readily decalcifies in the presence of acidic conditions.
- 7. Non collagenous • Non- collagenous proteins- play important role in matrix deposition, initiation and control of mineralization and matrix remodelling. Include: Bone sialoprotein, osteopontin,tenascin, fibronectin, osteocalcin . • Proteoglycans- Chondroitin sulphate,hyaluronate, heparan sulfate, biglycan and osteoadherin.
- 8. Growth factors- TGFß, bone morphogenetic proteins (BMP’s),Platelet derived growth factors, Osteoprotegerin (OPG). Cementum derived growth factor seen exclusively in cementum. is an insulin like molecule. Enhance proliferation of gingival fibroblasts and periodontal ligament cells.
- 9. CLASSIFICATION • ACELLULAR CEMENTUM • CELLULAR CEMENTUM
- 10. ACELLULAR CEMENTUM • Term acellular is UNFORTUNATE because as a living tissue Cells are an integral part. • However some layers do not incorporate cells while other layers do not contain such cells in their lacunae. • First to be formed. • Sharpeys fibers make most of the structure.
- 11. • Forms during root formation before tooth reaches occlusal plane. • Covers approx. cervical 1/3rd (coronal portion)of the root. • Does not contain any cells. • More calcified. • Formation is slow • Arrangement of collagen fibers are more organized
- 12. CELLULAR CEMENTUM • Forms after the eruption of tooth once it reaches occlusal plane. • Its formation is also in response to the functional demands. • Sharpeys fibers occupy a smaller portion. • Contains cementocytes in lacunae that communicate with each other by canaliculi.
- 13. • Covers apical 2/3rd of the root • Contains cementocytes • Its deposition is more rapid • Collagen fibers are irregularly arranged.
- 14. SHROEDER & PAGE CLASSIFICATION 1986 • Classified CEMENTUM on the basis of : – LOCATION – MORPHOLOGY – HISTOLOGICAL APPEARANCE
- 15. 1. Acellular Afibrillar Cementum (AAC) 2. Acellular Exrinsic Fiber Cementum (AEFC) 3. Cellular Intrinsic Fiber Cementum (CIFC) 4. Cellular Mixed Stratified Cementum (CMSC) 5. Intermediate Cementum
- 17. Acellular Afibrillar Cementum (AAC) • FIBERS -ABSENT • CELLS- ABSENT • FORMED BY-CEMENTOBLASTS • LOCATION- CORONAL CEMENTUM • THICKNESS- 1-15μm
- 18. Acellular Extrinsic Fiber Cementum (AEFC) • FIBERS- DENSELY PACKED BUNDLES OF SHARPEY’S FIBRES • CELLS-ABSENT • FORMED BY –FIBROBLASTS & CEMENTOBLASTS • LOCATION -CERVICAL THIRD OF ROOT • THICKNESS - 30-230μm
- 19. Cellular Intrinsic Fiber Cementum (CIFC) • FIBERS - INTRINSIC FIBRES • CELLS - PRESENT • FORMED BY - CEMENTOBLASTS • LOCATION - RESORPTION LACUNAE
- 20. Cellular Mixed Stratified Cementum (CMSC) • FIBERS- EXTRINSIC SHARPEY’S & INTRINSIC FIBRES • CELLS - PRESENT • FORMED BY - FIBROBLASTS & CEMENTOBLASTS • LOCATION - APICAL 1/3 rd OF ROOT & FURCATION • THICKNESS - 100 -1000μm
- 21. INTERMEDIATE CEMENTUM • CELLS - CELLULAR REMNANTS OF HERTWIGS SHEATH • LOCATION – CEMENTODENTINAL JUNCTION • THICKNESS - 10μm
- 22. CEMENTOGENESIS (Berkovitz) Formation of cementum is known as cementogenesis Cementum formation takes place along the entire root. At the advancing root edge, HERTWIG’S EPITHELIAL ROOT SHEATH (HERS), which is derived from the extension of inner and outer enamel epithelium releases enamel proteins. HERS possibly sends inductive message to the ectomesenchymal cells of pulp.
- 23. These ectomesenchymal cells of pulp now differentiate into odontoblasts and produce a layer of predentin along the inner aspect of HERS. Once dentin formation is underway, breaks occur in HERS. Therefore the inner layer of dental follicle comes in contact with predentin. Cells of the dental follicle now differentiate into CEMENTOBLASTS which are the main cells responsible for cementum formation.
- 24. Cementoblasts synthesize organic matrix which is uncalcified and called as cementoid tissue or precementum Uncalcified cemental matrix – cementoid
- 26. PTHrP: parathyroid hormone–related protein; BMP: bone morphogenetic protein CSF: colony-stimulating factor; EGF: epidermal growth factor BSP: bone sialoprotein; OC: osteocalcin; OPN: osteopontin.
- 27. Regeneration versus development: events and cells. While similar events occur during development and regeneration of tissues, there are clear differences in cell types involved and in some of the factors promoting cell types involved and in some of the factors promoting cell
- 28. MINERALIZATION • Mineralization begins in the depth of precementum. • Fine hydroxyapatite crystals are deposited, first between and then within the collagen fibrils by a process that is identical to the mineralization of bone tissue. • Zander & Hurzeler examined the thickness of cementum on extracted human teeth from individuals of varying ages & concluded that the mean,linear rate of cementum deposition on single-rooted teeth is about 3 pm per year, (but varying greatly with tooth type, root surface area, and type of cementum being formed).
- 29. • A similar rate has been found for acellular extrinsic fiber cementum in premolars and in nonfunctioning, impacted teeth • The width of the precementum layer is about 3-5 um. • Process of establishing the appropriate condition for crystallization & growth of the individual crystals in cementum normally are extremely slow and extend over a period of several months
- 30. The development of cementum has been subdivided into: Pre-functional stage Functional stage Prefunctional portion of the cementum is formed during root development & is extremely long lasting process. The functional development of cementum, commences when the tooth is about to reach the occlusal level & is associated with the attachment of root to the surrounding bone & continues throughout life. It is mainly during this stage that adaptive & reparative processes are carried out by the biological responsiveness of cementum.
- 32. CEMENTOBLAST S Derived from dental follicle. Transformation of mesenchymal cells of dental follicle. Cemento-progenitor cells synthesize collagen and protein polysaccharide. These cells have numerous mitochondria, a well formed Golgi- apparatus and large amounts of granular endoplasmic reticulum.
- 33. Histological observation of areas of root resorption has shown that cementoblasts can arise wherever viable dentin is exposed to the soft tissue of the periodontal ligament. Induction of cementoblasts from periodontal ligament cells can apparently take place throughout life, as evidenced by physiological areas of cemental repair. Cellular turnover among cementoblasts is slow compared with that in the osteoblasts that line the alveolus. Furthermore, it appears that cementoblasts are capable of altering their rate of cementum deposition.
- 34. CEMENTOCYTES Cementocytes in lacunae and the channels in which their processes extend are called the canaliculi. The central cell mass may appear rounded or oval & diameter ranges from 8-15 um. The cytoplasm is palely basophilic and the nucleus is centrally located.
- 35. Cementocytes communicate with each other through a system of anastomosing canaliculi radiating from their body
- 36. CEMENTO ENAMEL JUNCTION The junction between the cementum and enamel at the cervical region of the tooth is termed Cemento-Enamel junction
- 37. In about 60% cases cementum overlaps the cervical end of enamel. In approx. 30% of all teeth cementum meets the cervical end of enamel. In 10% cases enamel and cementum do not meet which can cause accentuated sensitivity because of exposed dentin. In about 1.6% of cases enamel overlaps cementum. four TYPES OF RELATIONSHIP EXIsTS
- 38. Journal of Indian Society of Periodontology - Vol 18, Issue 5, Sep-Oct 2014
- 39. VARIOUS METHODS OF CEJ LOCATION • Methods for location of CEJ include following two kinds: – Conventional – Modified A. In conventional methods we have: • Visual • Tactile • By straight explorer • By periodontal probe; examiner feels for the cervical line with the tip of the probe • Radiographic • Intraoral periapical (IOPA) radiograph • Bite wings • RVG
- 40. B. In modified methods we have: • Computer linked electronic constant pressure probes – Florida probe – Inter probe/Perio probe – Birek probe/Toronto automated probe – Jeff coat probe/Foster miller probe. Journal of Indian Society of Periodontology - Vol 18, Issue 5, Sep-Oct 2014
- 41. THE CEMENTO-DENTINAL JUNCTION (CDJ) The terminal apical area of cementum where it joins the internal root dentin is called cementodentinal junction or CDJ The nature of CDJ is of particular importance, being of interest biologically because it forms an interface (a fit) between two very different mineralized tissues. It is also of clinical importance because of the processes involved in maintaining tooth function while repairing a diseased root surface. Width of CDJ is 2 to 3um and remains relatively stable
- 42. FUNCTIONS • ANCHORAGE • ADAPTATION • REPAIR and RESORPTION
- 43. ANCHORAGE • To furnish a medium for the attachment of collagen fibers that bind the tooth to alveolar bone. • Connective tissue attachment to the tooth impossible without cementum. • EXAMPLE- in hypophosphatasia, loosening and premature loss of anterior deciduous teeth occurs. The exfoliated teeth are characterized by an almost total absence of cementum
- 44. ADAPTATION • Continuous deposition of cementum is of functional importance. – Cementum is not resorbed under normal conditions. – As the most superficial layer of cementum ages, a new layer is deposited that keeps the attachment apparatus intact.
- 45. REPAIR • Serves as a major reparative tissue for root surfaces. • Damage to roots such as fractures and resorptions can be repaired by the deposition of new cementum.
- 46. RESORPTION OF CEMENTUM • Cementum although is less susceptible to resorption than bone. • Resorption is carried out by multinuclear odontoclasts & may continue into the root dentine. • Acc. To a study approx 70% of all resorption areas were confined to the cementum without involving the dentin.
- 47. • Local Factors For Resorption – Trauma from occlusion. – orthodontic movement – pressure from malaligned erupting teeth, – cysts, and tumors; – Teeth without functional antagonists; – embedded teeth; – replanted and transplanted teeth; – Periapical and periodontal disease.
- 48. Cemental resorption associated with excessive occlusal forces. A, Low-power histologic section of mandibular anterior teeth. B, High-power micrograph of apex of left central incisor shortened by resorption of cementum and dentin. Note partial repair of the eroded areas (arrows) and cementicle at upper right
- 49. • SYSTEMIC FACTORS – calcium deficiency, – hypothyroidism, – hereditary fibrous osteodystrophy, – Paget's disease. • IDIOPATHIC
- 50. • Cementum resorption appears microscopically as baylike concavities in the root surface. • Multinucleated giant cells and large mononuclear macrophages are generally found adjacent to cementum undergoing active resorption. • Cementum repair can occur in devitalized as well as in vital teeth. • Resorption occurs most commonly in apical third then middle third followed by gingival third.
- 52. CEMENTICLES • Are small, globular masses of cementum found in approx 35% of human roots. • May not be always attached to the cementum surface but may be located free in Pdl. • These may result from microtrauma, when extra stress on sharpeys fibers causes a tear in the cementum. • Are more commonly found in apical & middle third of root and in root furcation areas
- 53. • May develop from calcified epithelial rests; around small • spicules of cementum or alveolar bone traumatically displaced • into the periodontal ligament; from calcified • Sharpey's fibers; and from calcified, thrombosed vessels • within the periodontal ligament
- 54. ENAMEL PEARLS If some HERS cells remain attached to forming root surface, they can produce focal deposits of enamel like structures called ENAMEL PEARLS.
- 55. Clinical significance They are plaque retentive structures. Promote periodontal disease. They look similar to calculus, but cannot be scaled off. Only grinding will help in elimination.
- 56. ABNORMALITIES OF CEMENTUM Cemental Hyperplasia or Hypercementosis – Refers to abnormal thickening of cementum. It is largely an age related phenomenon It can be – Localized to one tooth Generalized- affect the entire dentition.
- 57. • If the overgrowth improves the functional qualities of the cementum, it is termed as cementum hypertrophy. • If the overgrowth occurs in nonfunctional teeth or if it is not correlated with increased function, it is termed cemental hyperplasia.
- 58. Appearance: Occurs as a generalised thickening of cementum, with nodular enlargement of the apical third of the root It also appears in the form of spike like excrescenses (cemental spikes) created by either the coalescence of cementicles that adhere to the root or the calcification of the periodontal fibres at the site of insertion into the cementum Hypercementosis
- 59. It is usually associated with situations like – teeth without antagonist teeth with pulpal and periapical infections Hypercementosis of entire dentition may be seen in patients with Paget's disease. Other systemic disturbances include acromegaly, calcinosis, thyroid goiter, arthritis etc.
- 60. Treatment: Hypercementosis itself does not need treatment. It could pose a problem if an affected tooth requires extraction. In multirooted tooth, sectioning of tooth may be required before extraction.
- 61. Cemental aplasia or hypoplasia: Absence or paucity of cellular cementum. Hypophosphatasia Hypophosphatasia is due to an inborn error of metabolism.The basic disorder is a deficiency of enzyme alkaline phosphatase in serum or tissues. This is characterised by loosening and premature exfoliation of deciduous teeth,mainly anteriors. Exfoliated teeth microscopically show complete absence of cementum or isolated areas of abnormally formed cementum.
- 62. Cemental Tear : The detachment of a fragment of cementum is described as a cemental tear. Cemental tears have been reported in the periodontal literature associated with localized, rapid periodontal breakdown. Cemental Tear
- 63. ANKYLOSIS Fusion of cementum and alveolar bone and obliteration of the periodontal ligament is called ankylosis. Results in resorption of root and its replacement by bone tissue. This condition is uncommon. Occurs in teeth with cemental resorption. It represents a form of abnormal repair.
- 64. Ankylosis can also occur after: Chronic periapical infection Tooth reimplantation Occlusal trauma Around embedded teeth. More common in primary dentition
- 65. Clinically: 1. Lack of physiologic mobility which is diagnostic sign of ankylotic resorption. 2. As the periodontal ligament is replaced with bone in ankylosis, proprioception is lost because pressure receptors in periodontal ligament are deleted or not function correctly. 3. Teeth have special metallic percussion sound. 4. If the process continues teeth will be in infraocclusion.
- 66. Radiographically: Resorption lacunae are filled with bone. Periodontal ligament space is missing. Treatment: No predictable treatment can be suggested. Treatment modalities range from a conservative approach,such as resotorative intervention to surgical extraction of affected tooth.
- 67. EXPOSURE OF CEMENTUM TO ORAL ENVIRONMENT • Exposed in cases of gingival recession leading to pocket formation. • Permeable to be penetrated by organic substances, inorganic ions and bacteria.
- 68. Leading to fragmentation & breakdown of cementum & resulting in areas of necrotic cementum seperated from tooth by masses of bacteria Bacterial penetration found as deep as cemento dentinal junction Collagenous remnants of sharpeys fibers undergo degeneration Creating environment for bacterial penetration 87% viable bacteria found in roots of periodontally non carious teeth As pocket deepens Collagen fibers destroyed Cementum exposed to oral environment
- 69. CONCLUSION Cementum forms a functional unit which is designed to maintain tooth support, integrity, and protection. Minor, non-pathological resorption defects on the root surface are generally reversible and heal by reparative cementum formation. Irreversible damage may occur when the cementum is exposed to the environment of a pocket or oral cavity.
- 70. REFERENCES Carranza’s clinical periodontology (10th & 11th edition) Jan Lindhe – Text Book Of Clinical Periodontology (4th edition) Orban’s –Text Book Of Oral Histology And Embryology 11th & 13th edition Tencates – Text Book Of Oral Histology (10th edition) • A Color Atlas & Text Of Oral Anatomy & Embryology – 2nd Edition B.K.B Berkovitz
- 71. PERIO 2000 - Dental cementum: the dynamic tissue covering of the root. Dieterd . Bosshard &t Knuta . Selvig Journal of Indian Society of Periodontology - Vol 18, Issue 5, Sep-Oct 2014 PERIO 2000 - Molecular and cell biology of cementum Nazan E. Saygin, William V. Giannobile&martha J. Somerman