Presentation2, radiological imaging of diaphagmatic hernia.
•Download as PPTX, PDF•
24 likes•7,811 views

Health&Medicine.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation2, radiological imaging of diaphagmatic hernia.
Similar to Presentation2, radiological imaging of diaphagmatic hernia. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation2, radiological imaging of diaphagmatic hernia.
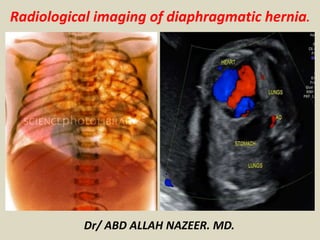
- 1. Radiological imaging of diaphragmatic hernia. Dr/ ABD ALLAH NAZEER. MD.
- 2. Types of diaphragmatic hernias.
- 3. Congenital diaphragmatic herniation (CDH) accounts for a small proportion of all diaphragmatic hernia. However, it is one of the most common non-cardiac fetal intrathoracic anomalies. Epidemiology Congenital diaphragmatic hernias are seen in 1 of every 2000-4000 live births. 84% are left-sided, 13% are right-sided and 2% bilateral. Clinical presentation Most congenital diaphragmatic hernias are detected either soon after birth or on antenatal ultrasound. Mortality is predominantly due to development of pulmonary hypoplasia, which is thought to be due to mass effect on the developing lung. Such neonates are hypoxic and have persistent fetal circulation due to pulmonary hypoplasia and pulmonary hypertension. Pathology Diaphragmatic development is usually complete by ~9th week of gestation. Congenital diaphragmatic hernias result from failure of fusion of one of the pleuroperitoneal canals at about 8 weeks gestation. They may contain stomach, intestines, liver or spleen.
- 4. Classification Congenital diaphragmatic herniation can be classified into two basic types on location: Bochdalek hernia most common fetal congenital diaphragmatic hernia commoner on the left: 75-90% posterolateral large and associated with poorer outcome presents earlier mnemonic: BBBBB Morgagni hernia less common anterior presents later
- 5. Associations While a CDH can occur as an isolated condition, associated anomalies are relatively common and include: pulmonary hypoplasia: also a complication bronchopulmonary sequestration aneuploidy: can be present in up to 50% of cases trisomy 13 trisomy 18 trisomy 21 Turner syndrome: monosomy X Pallister-Killian syndrome: tetrasomy 12p Fryns syndrome Cornelia de Lange syndrome congenital cardiac anomalies neural tube defects anencephaly Spina bifida
- 6. Hiatus hernias (HH) occur when there is herniation of abdominal contents through the esophageal hiatus of the diaphragm into the thoracic cavity. Epidemiology The prevalence of HH increases with age, with a slight female predilection. Clinical presentation Many patients with HH are asymptomatic and it is an incidental finding. However, symptoms may include epigastric or chest pain, postprandial fullness, nausea and vomiting. Sometimes HH are considered synonymous with gastro-esophageal reflux disease (GORD) but there is a poor correlation between the two conditions. Pathology The most common contents of a HH is the stomach. Congenital hiatal hernia: very rare. . in most cases contains stomach. . it's mainly associated with the congenital short esophagus, where the stomach presents a non-reducible intrathoracic position. . it's located postero-centrally (esophageal hiatus).
- 7. Acquired hernias The most common diaphragmatic hernia, hiatal hernia being responsible for about 90% of cases. Hiatal hernia passage into the chest cavity of abdominal contents through the esophageal hiatus. contains more often stomach. According to the herniated content may be classified into four types: Type I - or sliding hernia, results from cephalic migration of the gastroesophageal junction through a generally wider esophageal hiatus. Is the most common type of hiatal hernia (≈ 90%) and patients are often asymptomatic. Type II - or paraesophageal hernia, results from herniation of a portion of the stomach into the chest cavity, with the gastroesophageal junction in its normal position. It is the second most common type of hiatal hernia (≈ 10% of cases). Type III - or mixed type (among type I and II), it's uncommon and results from cephalic migration of the gastroesophageal junction and herniation of a portion of the stomach. Type IV - it's rare, and can result from two situations: herniation of stomach together with other abdominal viscera or herniation of most of the stomach, except cardia and pylorus - the "upside down" stomach.
- 8. Traumatic hernia Uncommon most frequently results from blunt trauma and ≈ 90% from traffic accidents generally young males affects more often the left hemidiaphragm (3:1) the diaphragmatic defect tends to be more irregular than the congenital ones; when it results from blunt trauma tends to be bigger (> 10 cm) than those resulting from penetrating injury (1-2 cm). > 50% associated with other life-threatening organ damage – emergencies early diagnosis is difficult and depends on high degree of suspicion occasionally can be diagnosed later, clinically ranging from chronic symptoms to surgical emergencies.
- 9. Radiographic features Ultrasound Indirect sonographic findings that should prompt a search for CDH include: polyhydramnios cardiomediastinal shift +/- abnormal cardiac axis inability to demonstrate the normal stomach bubble The study should be performed in the true transverse plane. Sonographic diagnosis of CDH can be made from the following findings: absent bowel loops in the abdomen intra-thoracic herniation of the liver; noted in up to 85% of cases and is associated with a worse prognosis Left-sided CDH stomach and small bowel (echo-free) at the same transverse level as the heart on four-chamber view: this makes left sided hernias comparatively easier to detect on ultrasound (as opposed to herniation of echogenic liver on the right side) stomach and small bowel superior to the inferior margin of the scapula leftward displacement of the gallbladder
- 10. Right-sided CDH color Doppler study leftward bowing of the umbilical segment of the portal vein portal branches to the lateral segment of the left hepatic lobe coursing towards or above the diaphragm gallbladder present above diaphragm echodense space between the left heart border and stomach representing the left hepatic lobe Although classically considered a cystic echogenic lung mass, there are reports of CDH appearing initially as a solid echogenic lung mass that evolves in appearance with advancing gestation. The observed-to-expected lung-to-head ratio (O/E LHR) may be calculated, and correlates with the degree of pulmonary hypoplasia. Studies suggest that the degree of lung hypoplasia can used to predict survival rates and the numbers from the Antenatal-CDH-Registry group that apply to isolated left-sided CDH and liver herniation are shown below: O/E LHR < 15% (extreme pulmonary hypoplasia): virtually no chance of survival O/E LHR 15-25% (severe pulmonary hypoplasia): predicted survival ≈ 15% O/E LHR 26-45% (moderate pulmonary hypoplasia): predicted survival 30-75% O/E LHR > 45% (mild pulmonary hypoplasia): very likely to survive
- 11. Plain radiograph indistinct diaphragm with opacification of part of or all the hemithorax (typically left sided) scaphoid abdomen deviation of lines endotracheal tube nasogastic tube umbilical arterial and venous catheters MRI Fetal MRI may be helpful in further assessing the hernia and any associated pulmonary hypoplasia. Sequences typically performed for assessment of CDH include: T2-weighted three-plane single shot fast spin echo (SSFSE) Fluid filled stomach and small bowel appear hyperintense T2-weightedbalanced steady state free precession (bSSFP) flowing blood appears hyperintense: portal vessels may be seen extending toward or above diaphragm T1-weighted fast field echo (FFE) liver appears moderately hyperintense T2-weighted half-fourier acquisition single-shot turbo spin echo (HASTE) lungs appear hyperintense (composed primarily of water) while heart, mediastinum and liver appear hypointense
- 12. CT In adults with congenital diaphragmatic hernia, previously undiagnosed Bochdalek hernias are most frequently identified when patients undergo computed tomography (CT) scanning for reasons that appear to be unrelated to the hernia. These Bochdalek hernias usually contain retroperitoneal fat or a kidney. focal fat collection in middle mediastinum. Hiatus hernia, omentum herniates through phrenicoesophageal ligament may see increase in fat surrounding distal esophagus paraesophageal hernia through widened esophageal hiatus visualise contents, size, orientation of herniated stomach within lower thorax herniated contents lie adjacent to esophagus widening of esophageal hiatus dehiscence of diaphragmatic crura (>15 mm): increased distance between crura and esophageal wall
- 13. Anteroposterior (AP) chest radiograph of a right-sided congenital diaphragmatic hernia (CDH) shows a mediastinal shift and lung compression caused by herniation of the liver and multiple bowel loops.
- 14. Anteroposterior (AP) chest radiograph of a right-sided congenital diaphragmatic hernia (CDH) shows herniation of the liver and bowel loops into the right hemithorax, with a shift of the heart and mediastinum to the left side.
- 15. Anteroposterior (AP) view of the abdomen in a patient with a congenital diaphragmatic hernia (CDH) shows a gasless pattern caused by herniation of bowel loops into the right hemithorax.
- 16. Anteroposterior (AP) view of the chest in a patient with a congenital diaphragmatic hernia (CDH) shows a left-sided Bochdalek hernia.
- 17. Anteroposterior (AP) view of the chest in a patient with a congenital diaphragmatic hernia (CDH) shows herniation of bowel loops into the left hemithorax, with a shift of the heart and mediastinum to the right side.
- 18. Left CDH
- 19. Fetal retrosternal mediastinal hernia. Coronal (a) and axial (b) SSFSE T2-weighted MR images obtained at 30 weeks 3 days gestation show a herniated liver (solid arrows) ventral to the dorsally displaced heart (open arrow) on both sides of the chest.
- 20. Ultrasonogram of a right-sided congenital diaphragmatic hernia shows the liver herniating through the defect.
- 21. Neonatal Bochdalek hernia. a A 1-day-old boy with left Bochdalek hernia. Chest radiograph shows deviation of the endotracheal tube and esophageal portion of the nasogastric tube to the right. Intrathoracic displacement of the nasogastric tube tip, bowel and stomach confirm the diagnosis of diaphragmatic hernia. b A 2-day-old girl with right Bochdalek hernia. Chest radiograph shows deviation of the nasogastric tube and umbilical venous catheter (arrow) to the left.
- 22. Serial chest radiographs in a newborn with left Bochdalek hernia show gradual resorption of large left pneumothorax, progressive expansion of hypoplastic left lung, accumulation of fluid into the left chest cavity and shift of mediastinal structures to a more normal position by postoperative day 7. Note coiled epidural catheter (arrows). a Post repair day 1. b Post repair day 3. c Post repair day 7
- 23. A 4-day-old infant with a Bochdalek defect and herniation of solid viscera presenting with mild respiratory distress. a Chest radiograph shows bowel in the left hemithorax and a soft-tissue retrocardiac mass (arrows). b Coronal reconstructed, contrast-enhanced CT image shows intrathoracic herniation of the spleen and left kidney through a large Bochdalek hernia
- 24. 7-year-old boy with neonatal patch repair of a Bochdalek hernia and recurrent defect. a Upper abdominal radiograph shows bowel loops in the left chest. b, c Coronal (b) and sagittal (c) contrast-enhanced CT reconstructions show a recurrent herniation of colon and mesentery through the medial and anterior lip of the patch repair
- 25. Bochdalek hernia- chest x-ray without diaphragmatic hernia signs. CT showed a small posterior and left sided diaphragmatic defect (interrupted red line) through which passes abdominal fat (green shade).
- 26. Bochdalek hernia. Chest X-ray showed a supradiaphragmatic opacity in the lower half of the left hemithorax, where one can view a hollow viscera air camera. CT showed a large diaphragmatic defect (interrupted red line), through which passes the left kidney, spleen and colonic segment (brown shade).
- 27. Bochdalek hernia- Chest X-ray showed an opacity with colic air camera on the left lateral costophrenic angle. CT showed a small diaphragmatic defect (red line), between the left posterior leaflet and the central tendon, through which passes abdominal fat and colic segment. Patient underwent urgent laparoscopic repair. (C-colon)
- 28. A 2-week-old boy with Morgagni defect presenting with respiratory difficulty. Anteroposterior (a) and lateral (b) chest radiographs show intrathoracic bowel herniating through an anterior foramen of Morgagni defect
- 29. Morgagni Hernia.
- 30. 7-day-old boy with a Morgagni hernia. a, b Anteroposterior (a) and lateral (b) chest radiographs show a poorly defined right chest mass and right upper lung atelectasis. c Sagittal color Doppler sonogram of the right chest obtained on the same day shows herniation of the liver (L) through an anterior foramen of Morgagni hernia (arrows). Note the abnormal course of the hepatic vein and the difference in echotexture of the intrathoracic (T) and intraabdominal (A) portions of the liver. d, e Sagittal (d) and coronal (e) contrast- enhanced CT reconstructions obtained the same day confirm anterior liver (L) herniation
- 31. Morgagni hernia – case 2. 49 y/o female with dyspnea and no traumatic history. Chest x-rays showed an inferior- anterior opacity on the right hemithorax (green shade), containing intestinal loops. CT showed an anterior-right diaphragmatic defect (interrupted red line), through which passes fat, colon segments and blood vessels to the chest, with focal stenosis of the herniated contents on the diaphragmatic defect – collar sign (green line). Patient underwent open surgery, where it carried out reduction and suture of the diaphragmatic defect. (C-colon)
- 32. Morgagni hernia – On chest radiography an opacity was incidentally detected occupying the right cardiophrenic angle. MR showed an anterior-right diaphragmatic defect (interrupted red line), through which epiploic fat migrated into the thorax, with clear focal stenosis of the fat on the diaphragmatic defect – collar sign (green line).
- 33. Morgagni hernia – Chest x-rays showed an inferior-anterior opacity on the right hemithorax (green shade), containing intestinal loops. CT showed an anterior-right diaphragmatic defect (interrupted red line), through which passes fat, colon segments and blood vessels to the chest, with focal stenosis of the herniated contents on the diaphragmatic defect – collar sign (green line). Patient underwent open surgery, where it carried out reduction and suture of the diaphragmatic defect. (C-colon)
- 34. Diaphragmatic tear in a 10-year-old child who was involved in a motor vehicle accident.
- 35. Central, retrosternal hernia (pentalogy of Cantrell) in a 5-month-old with a large omphalocele repaired as a newborn. Sagittal (a), anterior coronal (b), and axial (c) contrast-enhanced CT images of the chest show anterior herniation of the heart, liver (L) and bowel through an anterior thoracoabdominal defect. Note the hypoplastic sternal ossification centers (arrow)
- 36. A 4-month-old girl with a paraesophageal hernia who presented with vomiting. a Chest radiograph obtained during an upper gastrointestinal series shows intrathoracic herniation and organoaxial volvulus of the stomach into a paraesophageal hernia. b Delayed radiograph of the upper abdomen shows herniation of the transverse colon
- 37. Newborn with a congenital short esophagus presenting with respiratory distress and gagging. a Chest radiograph shows a large cystic structure in the right hemithorax within which is coiled a nasogastric tube. Note a lens-shape density overlying the right lower chest (arrows) b Radiograph obtained after administration of water-soluble contrast material via the nasogastric tube confirms a short esophagus with a fixed intrathoracic stomach. Note the malfixated small bowel in the abdomen. c Sagittal T2-W MR image through the right chest shows a small additional posterolateral (Bochdalek) hernia with liver herniation (arrow)
- 38. Hiatal hernia.
- 39. Hiatal hernia type I or sliding hernia - on chest X-ray. CT incidentally shows a small hiatal hernia that results from cephalic migration of the gastroesophageal junction through a wider esophageal hiatus. Targeted therapy was not required. Note the clear focal stenosis of the herniated contents through the hiatus – collar sign (green line).
- 40. Hiatal hernia type II or paraesophageal hernia - This is the case of a 73 y/o male with solids dysphagia and transient chest pain. CT showed herniation of gastric fundus with normal topography of the gastroesophageal junction. Note the clear focal stenosis of the herniated contents through the hiatus – collar sign (green line). Legend: Esoph.-esophagus; GE-gastroesophageal junction.
- 41. Hiatal hernia type III or mixed - This is the case of 82 y/o female, with a posterior mediastinal opacity on chest X-ray. CT showed a detachment from the columns of the right crus resulting in widening of the esophageal hiatus, allowing cephalic migration of the gastroesophageal junction and herniation of almost the whole stomach to the thoracic cavity, with the pylorus at the level of esophageal hiatus. Note the clear focal stenosis of the herniated contents through the hiatus – collar sign (green line).
- 42. Hiatal hernia type IV - This is the case of an 83 y/o female with abdominal pain and dyspnea. Chest X- ray showed a widened lower mediastinum and images of hollow viscus in the chest. CT showed detachment from the columns of the right crus resulting in widening of the esophageal hiatus, allowing cephalic migration of stomach and colon to the thoracic cavity. Note the clear focal stenosis of the herniated contents through the hiatus – collar sign (green line). Legend: S-stomach; C-colon
- 43. Hiatal hernia type IV or "upside down" stomach - This is the case of a 75 y/o female with a basal opacity of the left hemithorax and air-fluid levels on chest X-ray. Upper gastrointestinal series revealed herniation and gastric volvulus, with both cardia and pylorus at the level of esophageal hiatus. CT showed a detachment from the columns of the right crus resulting in widening of esophageal hiatus, allowing complete migration of the stomach to the thoracic cavity, with a discrete cephalic migration of the pylorus and cardia.
- 44. Traumatic diaphragmatic hernia – case 1. 35 y/o female victim of a car accident. Chest X-ray showed the classic sign of a nasogastric tube loop in the stomach above the diaphragm (pink line). On CT it was difficult to define the diaphragm at the left side, without marked collar signal of the herniated contents, typical findings of traumatic diaphragmatic rupture. Note the herniated content fallen to a dependent position against the posterior left ribs - dependent viscera sign (yellow arrow). This patient had associated splenic injury and underwent emergent surgery.
- 45. Traumatic diaphragmatic hernia – case 2. 65 y/o male, with history of car accident 10 years ago. Chest X-ray revealed opacity of the lower third of the right hemithorax, which displays a hollow viscera air camera. MR showed an anterior-right diaphragmatic defect (interrupted red line), through which migrated epiploic fat, stomach, colon, and liver, with clear focal stenosis of the contents on the diaphragmatic defect – collar sign (green line). Note the unusual right sided hernia and the more irregular layout of the diaphragmatic defect. Legend: L-liver; S-stomach; C-colon.
- 46. A 66-year-old man with previous history of car accident 13 years ago complained of increasing shortness of breath. A. Chest radiograph: apparent elevation of the right hemidiaphragm. B. Coronal T1-weighted MRI: discontinuity of the right diaphragm (black arrows) and bowel herniation. C. Barium enema and UGI: herniation of the colon and a portion of stomach through the tear.
- 47. A 35-year-old man with previous history of aortic surgery for isthmic pseudoaneurysm after a car accident 2 years ago complained of severe chest pain and dyspnea for 3 days. Chest radiograph at emergency room shows an opacification of the left hemithorax. A. Contrast-enhanced multi-detecter row CT scan: lack of visualization of the left hemidiaphragm and dependant viscera sign. B. Sagittal and C. Coronal reformatted image: severe constriction of the stomach at the site of herniation (collar sign). D. Coronal volume-rendered CT image shows well the herniated constricted stomach (long arrow), dilated esophagus, and pleural effusion and collapsed left lung. Note also the normal position of the nasogastric tube (small arrows) in the non herniated portion of the stomach. At surgery, gastric strangulation was found.
- 48. Complete eventration of a hemidiaphragm is more common in males and typically occurs on the left side
- 49. Coronal CT following esophagectomy shows left diaphragmatic hernia with herniation of colon (arrow) into left hemithorax.
- 50. Thank You.