Presentation1, radiological film reading of elbow joint.
•Download as PPTX, PDF•
25 likes•2,009 views

Health &Medicine.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological film reading of elbow joint.
Similar to Presentation1, radiological film reading of elbow joint. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological film reading of elbow joint.
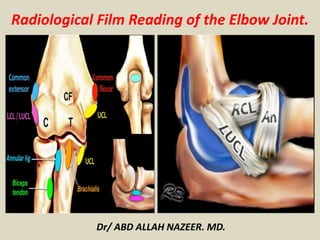
- 1. Dr/ ABD ALLAH NAZEER. MD. Radiological Film Reading of the Elbow Joint.
- 2. Normal anatomy of medial collateral ligament complex A. 3- dimensional schema demonstrates medial collateral ligament complex, composed of anterior (dashed arrow), posterior (arrow), and oblique (transverse, arrow head) bands. B. On T1- weighted coronal MR image, anterior bands of medial collateral ligament is identified.
- 3. Normal anatomy of lateral collateral ligament complex A- D. 3- dimensional schema (A) and T1- weighted coronal (B, C), axial (D) MR images demonstrate four components of lateral collateral ligament (LCL) complex, which are the lateral ulnar collateral (arrow heads), annular (dotted arrow), and radial collateral ligaments (arrow).
- 4. The lateral muscle compartment includes four superficial extensor muscles in the forearm (extensor carpi ulnaris, extensor digiti minimi, extensor digitorum, and extensor carpi radialis brevis) which share a common tendinous attachment to the lateral epicondyle of the humerus. Extension of all joints crossed by the tendons. Extensor carpi radialis longus (ECRL), Extensor carpi radialis brevis (ECRB), Extensor digitorum (ED), Extensor carpi ulnaris (ECU). B, C-E. The medial muscle compartment includes the pronator teres and the four superficial flexors: the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis. Flexor digitorum superficialis (FDS), Flexor carpi ulnaris (FCU), Pronator teres (PT), Flexor carpi radialis (FCR).
- 5. A. 3- dimensional schema demonstrates the anterior muscle compartment, comprised of the brachialis (asterisk) and biceps muscles (tendon, arrow), which flex the elbow. B. 3- dimensional schema shows the posterior muscle compartment, composed of the triceps, anconeus, and variably present anconeus epitrochlearis muscles. Tendon of triceps brachii is a powerful extensor of the elbow. The olecranon bursa lies between the olecranon and skin. C-E. T1-weighted sagittal and axial images show brachialis (asterisk), tendon of biceps muscles (arrow) and tendon of triceps brachii (arrowhead).
- 7. Medial collateral ligament tear. STIR coronal MR images revealed discontinuity with focal hypersignal intensity at the humeral attachment site of medial collateral ligament (arrow). Lateral collateral ligament (arrowheads) are intact. Collateral ligament pathology.
- 9. Coronal proton density-weighted fat-saturated MRI shows full-thickness tear (white arrow) of proximal humeral attachment of anterior bundle of ulnar collateral ligament (UCL) and edema (black arrow) within surrounding muscle fibers. Axial proton density- weighted fat-saturated MRI shows UCL posterior bundle disruption (long white arrow), with fluid surrounding ulnar nerve (short white arrow). High-grade tear of flexor digitorum superficialis (long arrow) and fluid surrounding median nerve (short arrow).
- 11. Coronal proton density-weighted fat-saturated MRI (left) and coronal proton density-weighted nonfat-saturated MRI (right) show anterior bundle UCL mid-substance tear (arrows).
- 13. A, B. Proton density-weighted coronal MR images of right elbow show non- visualization of radial collateral ligament with widening of radiocapitellar joint space, indicating a complete tear. A small intra-articular body is seen. Medial collateral ligament (arrowheads) are intact. C. On STIR coronal MR image, bone marrow edema is prominent in the radial head and lateral epicondyle of the humerus.
- 15. Medial collateral ligament injury in two different patients. Coronal fat-suppressed proton density-weighted MR images. Left image: partial tear (solid arrow). Right image: the anterior bundle of the UCL presents diffuse increase in signal intensity and thickening reflecting fibrosis and chronic pathology (open arrow).
- 17. Ulnar collateral ligament injury. (a) Coronal fat-saturated T2-weighted image demonstrates complete tear of the ulnar collateral ligament, with fluid-filled gap between ligament fibers (arrow). (b) Coronal proton density–weighted image in a baseball pitcher demonstrates marked thickening with chronic tear of the ulnar collateral ligament (arrow). Note the associated osseous reactive change (arrowhead). (c) Coronal gradient echo image in a different baseball pitcher demonstrates avulsion of the sublime tubercle (arrow).
- 19. T sign” of ulnar collateral ligament partial tear. Coronal fat-saturated T1-weighted image from a magnetic resonance arthrogram demonstrates contrast extending along the medial aspect of the sublime tubercle with disruption of the distal fibers of the ulnar collateral ligament (arrow).
- 21. A partial tear is seen creating a 'T-sign'.
- 23. Acute, complete proximal tear of the anterior bundle of the ulnar collateral ligament, with an associated flexor-pronator muscle strain.
- 25. Ulnar collateral ligament complete tear.
- 27. 22-year-old baseball pitcher with acute onset of medial elbow pain who had a surgically confirmed tear of the proximal and distal attachments of the ulnar collateral ligament. a) Coronal fat-suppressed intermediate-weighted fast spin-echo image and b) corresponding coronal fat-suppressed T2-weighted fast spin-echo image of the elbow shows disruption of the proximal (small arrows) and distal (large arrows) attachments of the anterior bundle of the ulnar collateral ligament. Also note the high signal intensity edema surrounding the torn ligament (small arrowhead) and within the bone marrow of the medial and lateral humeral condyles (large arrowheads).
- 35. Coronal short-tau inversion recovery (STIR) images demonstrate a partial tear of the radial collateral ligament.
- 37. Radiograph of elbow shows avulsion fracture (arrow) of lateral epicondyle. Right: Coronal proton density-weighted fat-saturated MRI shows radial collateral ligament avulsion (short solid arrow). Note edema of lateral epicondyle at site of avulsion (open arrow), complete tear of proximal UCL, and superficial common flexor tendon (long solid arrow).
- 39. Left: Coronal proton density-weighted fat-saturated MRI shows high-grade tear of lateral UCL (LUCL) humeral attachment (short arrow). Distal attachment of LUCL at supinator crest of ulna (arrowheads) is intact. Complete tear of UCL humeral attachment and common flexor attachment (long arrow) is seen. Right: Axial proton density-weighted fat-saturated MRI shows avulsion fracture of lateral epicondyle (long arrow). Extensive high-grade muscle tear of anterior and medial muscular compartments (short arrow) also is shown.
- 41. LCL injury. Coronal fat-suppressed proton density-weighted MR images. Upper left image shows a normal LCL (solid white arrow). Upper right image shows a full-thickness tear of the ulnar bundle of the LCL (solid blue arrow), as well as injury to the adjacent common extensor tendon (solid yellow arrow). Bottom left image shows bone marrow edema in the medial epicondyle and trochlea (*), as well a complete tear of the LCL (open blue arrow) and common extensor tendon (open yellow arrow). Bottom right image shows thickening of the LCL, indicative of a chronically torn and remodeled ligament
- 43. 19-year-old American football player with acute onset of lateral elbow pain following varus extension injury who had a surgically confirmed tear of the proximal attachment of the lateral collateral ligament. Coronal fat-suppressed T2-weighted fast spin-echo image of the elbow shows complete disruption of the proximal attachment of the ulnar band of the lateral collateral ligament (large arrow) and partial disruption of the overlying common extensor tendon origin (small arrow). Also note the high signal intensity edema within the musculature of the elbow (arrowheads).
- 45. Coronal intermediate-weighted fat-saturated image from MR arthrography demonstrates disruption of the RCL and LUCL, with marked contrast material accumulation around the lateral humeral condyle (arrow). Disruption of the LUCL has been associated with PLRI.
- 47. Coronal short inversion time inversion-recovery (a) and gradient-echo (b) MR images obtained after reduction for posterior dislocation depict a bone marrow contusion (arrow in a) in the lateral capitellum and lateral epicondyle, an injury produced by impact of the radial head. Full- thickness tears of the MCL (arrow in b) and LUCL complex (arrowhead in b) also are seen.
- 49. Sagittal T2-weighted (a) and coronal short inversion time inversion-recovery (b) MR images obtained after reduction for posterolateral dislocation of the radius show an intraarticular fracture of the radial head (arrow in a) and subcortical capitellar edema representing a bone marrow contusion at the site of radial head impact (white arrowhead). A partial- thickness tear of the MCL (white arrow in b), complete tear of the RCL (black arrow in b), and partial-thickness tear of the common extensor tendon (black arrowhead in b) also are seen. Note the diffuse soft-tissue edema within the elbow joint.
- 51. STIR coronal image demonstrates a thickened LUCL with intrinsic increased signal (arrowhead) of the proximal LUCL compatible with partial tear and severe degeneration.
- 53. Lateral epicondylitis. Fat suppressed proton density-weighted coronal images revealed focal irregular hypersignal intensity lesion in the humeral attachment site of common extensor tendon (arrow).
- 55. Lateral epicondylitis. Coronal fat-suppressed proton density-weighted MR images. On the left image, a complete tear of the common extensor tendon at its origin from the lateral epicondyle of the humerus is observed (white arrow). On the right image, the common extensor tendon is torn (yellow arrow). Note the presence of an avulsed osseous fragment from the lateral epicondyle (blue arrow).
- 57. Coronal fat-saturated T2-weighted image demonstrates tendinopathy and tear of the common extensor tendon (white arrow) as well as tear of the proximal lateral ulnar collateral ligament (black arrow). Note associated bone marrow edema of the lateral epicondyle (star).
- 59. Common extensor tendon injury. (a) Coronal fat-saturated T2-weighted image demonstrates tendinopathy and partial tear of common extensor origin (arrow). (b) Coronal proton density– weighted image demonstrates partial tear of common extensor origin (arrow).
- 61. Coronal fat-saturated T1-weighted image from a magnetic resonance arthrogram demonstrates partial tear of common extensor origin and proximal lateral ulnar collateral ligament (arrow).
- 63. Lateral epicondylitis, evaluated prior to extensor tendon release . STIR coronal and axial images demonstrate complete tear of the RCL and LUCL from its origin (red line). Fluid fills the defect (asterisk) created by torn and retracted RCL and LUCL (arrowhead) and partial tear of the overlying extensor tendon (arrow).
- 65. A coronal STIR image demonstrates a complete tear of the common extensor tendon and subjacent LUCL(arrow) from the lateral epicondyle. The origin of the extensor tendon (red asterisk) is more proximal on the lateral epicondyle compared to the origin of the LUCL (blue asterisk). The annular ligament (arrowheads) is lax and slightly distally retracted due to loss of stabilization by the RCL.
- 67. 46-year-old tennis player with chronic lateral elbow pain and a clinical diagnosis of lateral epicondylitis. Coronal fat-suppressed intermediate-weighted fast spin-echo image of the elbow shows thickening and high signal intensity within the common extensor tendon origin (small arrows). Note that the underlying proximal attachment of the ulnar band of the lateral collateral ligament (large arrow) is intact but is thickened and irregular.
- 69. Partial-thickness tear of the common flexor tendon origin.
- 71. Partial-thickness tears of the ulnar collateral ligament and pronator strain
- 73. A partial tear of the ulnar collateral ligament.
- 75. 55-year-old golfer with chronic medial elbow pain and a clinical diagnosis of medial epicondylitis. Coronal fat-suppressed intermediate-weighted fast spin-echo image of the elbow shows thinning and high signal intensity within the common flexor tendon origin (small arrow). Note the intact underlying proximal attachment of the anterior bundle of the ulnar collateral ligament (large arrow).
- 77. Medial epicondylitis . Gd-enhanced axial and coronal images show ill-defined enhancement at the humeral epicondyle insertion site of common flexor tendon (arrow) .
- 79. Medial epicondylitis. Coronal fat-suppressed proton density-weighted MR images . On the left image, a partial tear of the common flexor tendon (white arrow) is observed. On the right image, the common flexor tendon origin is usually thickened and shows increased signal intensity (yellow arrow).Note the presence of subtle bone marrow edema in the medial epicondyle (blue arrow).
- 81. Common flexor tendon injuries. (a) Coronal fat-saturated T2-weighted image demonstrates fluid signal within the common flexor tendon origin, consistent with partial tear (arrow). Coronal (b) and axial (c) fat-saturated T2-weighted images from a magnetic resonance arthrogram demonstrate full-thickness tear of the common flexor tendon from the medial epicondyle with tendon retraction and fluid signal in the expected location of the tendon (arrow).
- 83. Tennis Elbow.
- 85. The injury pattern begins with avulsion of the common extensor tendon and LUCL (yellow line). The LUCL (arrowheads) demonstrates laxity to the site of attachment at the tubercle of the supinator crest of the ulna. Sprain of the anterior band of the ulnar collateral ligament is demonstrated by intrinsic increased signal and loss of definition (arrow). Edema reflecting contusion of the overlying flexor digitorum muscle is seen as mildly increased T2 signal (asterisk).
- 86. Tendons.
- 87. Sagittal fat-saturated T2-weighted image demonstrates biceps tendon rupture with tendon retraction. Note abnormal signal and thickening of retracted tendon (arrow). In some cases, it may be necessary to extend the field of view to include the retracted biceps tendon. Tendons.
- 89. Rupture of distal biceps tendon. Non-visualization of distal tendon with tendon retraction on T1- weighted sagittal and axial images (between the two pink lines in A), suggesting complete rupture of the distal biceps tendon.
- 91. Complete tear at the musculotendinous junction of the distal biceps tendon. Note the presence of hematoma (white arrows) adjacent to the ruptured distal biceps tendon (yellow arrows), which is retracted proximally into the arm.
- 93. Complete tear of the distal biceps and injury to the bicipital aponeurosis. Images obtained with the patient in the FABS position shows a thickened and retracted proximal part of the tendon (white arrows). Note the presence of fluid (yellow arrows) filling the gap and extending to the radial tuberosity.
- 95. Bifurcated distal biceps brachii tendon. Partial tear of the long head (yellow arrows) and complete rupture and proximal retraction of short head of biceps brachii tendon (blue arrows). A strain is also observed at the musculotendinous junction of the short head (white arrow). Note the presence of fluid signal filling the tendinous gaps. Findings are far more conspicuous in the FABS position
- 97. Tendinopathy of the triceps tendon in two different patients. Upper row: subtle findings of triceps tendinosis, whit slight hyperintensity at the insertion of the triceps tendon and musculotendinous junction (white arrows). Bottom arrow: severe triceps tendinosis and enthesitis, with dystrophic calcification of the tendon (yellow arrow), soft tissue edema (solid blue arrow) and bone marrow edema in the olecranon (open blue arrow). Subtle ulnar neuritis is also observed (circle).
- 99. Axial T1- and sagittal T2-weighted fat-saturated images show a sprain of the triceps muscle and tendinosis.
- 103. Sagittal fat-saturated T2-weighted image demonstrates triceps rupture with tendon retraction (arrow) and surrounding fluid/hemorrhage.
- 105. Triceps tendon tear and olecranon avulsion fractures.
- 106. Ulnar neuropathy in a 38- year-old man presented numbness on the left 4th and 5th fingers. Coronal T2-weighted images show mild swelling and increased signal of the ulnar nerve (A, arrow). Gd-enhanced coronal and axial T1- weighted images (B, C) show enhancement of the ulnar nerve is seen. On electromyogram and nerve conduction studies, ulnar neuropathy at the elbow level was confirmed. Nerves.
- 108. Ulnar neuropathy. In the upper row, thickening and hyperintensity of the ulnar nerve along its course in the cubital tunnel is observed (white arrows). No cause was identified and it was though to be secondary to hypermobility of the ulnar nerve and possible subluxation or dislocation. The patient underwent surgery, and postoperative MR was performed (bottom row). Ulnar nerve transposition is observed, now lying anterior and lateral to the cubital tunnel (yellow arrows) . High signal intensity within the nerve is still depicted.
- 110. Ulnar neuropathy. In the upper row, thickening and hyperintensity of the ulnar nerve along its course in the cubital tunnel is observed (white arrows). No cause was identified and it was though to be secondary to hypermobility of the ulnar nerve and possible subluxation or dislocation. The patient underwent surgery, and postoperative MR was performed (bottom row). Ulnar nerve transposition is observed, now lying anterior and lateral to the cubital tunnel (yellow arrows) . High signal intensity within the nerve is still depicted.
- 112. Axial fat-saturated T2-weighted image demonstrates enlargement and increased signal of the ulnar nerve in the cubital tunnel (arrow), consistent with ulnar neuritis.
- 114. Ulnar neuritis.
- 116. Radial neuropathy in a 38-year-old woman who had right wrist weakness. Axial T2-weighted images show high signal intensity at the brachialis (B), extensor carpi radialis (ECR), and extensor (Ex) muscles.
- 118. Axial proton density–weighted image demonstrates a ganglion (arrow) adjacent to the posterior interosseous nerve (arrowhead).
- 120. Posterior interosseous neuropathy in a 29-year-old man presented right forearm weakness. T2 and contrast enhanced fat suppressed T1-weighted axial images reveal abnormal high signal intensity and mild enhancement of supinator (S), and extensor (Ex) muscles. Accompanied muscle atrophy is also noted.
- 121. Bursitis.
- 122. Bicipitoradial bursitis in a 76-year-old woman presented a painful soft tissue mass in the anterior aspect of the right forearm during 1 month. T2-weighted axial (A) and Gd-enhanced T1-weighted axial and sagittal images (B, C) show fluid collection (arrow head) around the biceps tendon (arrow) with rim enhancement. Mild swelling of the biceps tendon is also noted. Bursitis.
- 124. Bicipitoradial bursitis. Axial (a) and sagittal (b) fat-saturated T2-weighted images demonstrate fluid (white arrow) surrounding the distal biceps tendon (black arrow), consistent with bicipitoradial bursitis. This should not be mistaken for a distal biceps tear.
- 130. Olecranon bursitis in a 37-year-old man with painful swelling of the posterior elbow. He had a history of soft tissue scratch in the posterior aspect of the elbow 10 days ago. On T2-weighted axial images and contrast enhanced T1-weighted axial and sagittal images a loculated fluid collection in the overlying soft tissue of the ulnar olecranon is seen with rim enhancement. Adjacent soft tissue swelling is associated.
- 132. Olecranon bursitis in three different patients. Left image: mild superficial olecranon bursitis (white arrow) . Middle and right images: More severe olecranon bursitis in another patient (yellow arrows), with a fluid-filled bursa with peripheral enhancement and inflammatory changes in adjacent soft tissues, along with bone marrow edema in the olecranon (blue arrow).
- 134. Axial T2-weighted image demonstrates marked enlargement of the olecranon bursa (arrow) with internal debris, consistent with olecranon bursitis.
- 136. Olecranon bursitis.
- 144. Osteochondral injury affecting the posterior and medial aspect of the capitellar articular surface (white arrows). Note the presence of a loose body in the coronoid fossa (blue arrows). There is a superb correlation of CT and MR images.
- 146. Osteochondral injuries in two different patients. Upper row: stable osteochondral injury in the anterior and lateral aspect of the capitellum (white arrows), along with little synovial fluid. Bottom row: Unstable osteochondral injury in the anterior aspect of the capitellum (blue arrows), which shows linear high signal on T2-weighted images along the interface between the fragment and the capitellum.
- 148. Coronal (left), sagittal (middle), and axial (right) proton density-weighted fat-saturated MRI examinations show osteochondral injury of capitellum (arrows). In contrast to posterior capitellar impaction resulting from acute dislocation, radial head shows no fracture or edema. Findings are in keeping with isolated chronic osteochondral injury.
- 150. 25-year-old baseball pitcher with acute onset of posterior elbow pain. Sagittal fat-suppressed T2-weighted fast spin-echo image of the elbow shows extensive high signal intensity bone marrow edema within the olecranon process (arrows) consistent with a severe stress injury.
- 152. Calcified loose body in the coronoid fossa (arrows). It presents low signal intensity in both T1 and fat-suppressed PD sequences. No osteochondral lesion was found.
- 154. Synovial osteochondromatosis. Several intra-articular loose bodies (yellow arrows) are shown, particularly affecting the coronoid fossa. Moderate joint fluid is also present (white arrow). Degeneration of articular cartilage (blue arrow) and development of marginal osteophytes (not shown) were also found. These findings are typical for secondary osteochondromatosis.
- 158. Olecranon tophaceous gout. Note the presence of a distended superficial olecranon bursa, filled with a mass-like lesion isointense to muscle on T1WI (flechas blancas) and heterogeneous on T2WI (yellow arrows). Images obtained after administration of contrast material show enhancement of the thickened synovium (blue arrows).
- 160. Phlegmonous tricipital myositis (white arrows). Note the presence of bone marrow edema in the olecranon (yellow arrow), inflammatory changes in adjacent soft tissues, synovitis in the ulnohumeral joint (solid blue arrows) and mild olecranon bursitis (open blue arrow).
- 162. Elbow lipoma. Images show a well demarcated soft tissue mass located just lateral and superior to the medial epicondyle, posterior to the brachioradialis muscle and anterior to the triceps muscle. It is isointense to subcutaneous fat in both T1 WI (yellow arrows) and fat-suppressed T2 WI (blue arrow).
- 164. Intramuscular hemangioma. Note the presence of a lobulated mass in the brachioradialis muscle (arrows). The mass presents low signal on T1 WI , high signal on T2 WI and a progressive enhancement at contrast-enhanced MR imaging.
- 166. Subcutaneous AVM of the elbow. Note the presence of a vascular mass in the subcutaneous fat of the posterior aspect of the elbow, close to the olecranon (arrows). MR angiography (bottom arrow) shows the feeding arteries (originating from the superior and inferior ulnar collateral arteries) and venous drainage through the basilic vein.
- 168. Peripheral nerve sheath tumor. Note the presence of a small nodule within the lateral head of the triceps muscle. The lesion is well delineated, slightly hyperintense to muscle on T1 WI (white arrow), present cystic foci on T2WI (yellow arrow) and presents enhancement of the solid component (blue arrow).
- 170. Elbow leiomyosarcoma. A large ovoid and lobulated mass in observed in the subcutaneous fat of the medial aspect of the elbow. The mass presents heterogeneous high signal intensity foci on T1WI, related to hemorrhagic contents (white arrows), and heterogenous high signal intensity on T2WI (yellow arrows). Irregular enhancement of the mass is observed (solid blue arrows). Note the presence of intravascular invasion , as the lesion extends into the basilic vein (open blue arrow).
- 172. Synovial sarcoma.
- 176. Lipoma arborescens of the elbow.
- 178. Non-traumatic myositis ossificans circumscripta at elbow joint.
- 180. Coronal (a) and sagittal (b) fat-saturated T2-weighted images in a boy with Panner disease demonstrate bone marrow edema of the capitellar epiphysis (arrows). Bone marrow edema involves the entire capitellum with no discrete osteochondral defects identified.
- 182. Sublime tubercle avulsive stress injury.
- 184. Abnormal marrow edema compatible with a stress reaction (arrows) is identified within and deep to the medial epicondylar apophysis on both the proton density weighted (2a) coronal and (2b) axial images of the elbow. On the coronal image, the anterior band of the ulnar collateral ligament appears mildly edematous and demonstrates subtle laxity at its proximal aspect (arrowhead). Diagnosis: Little League Elbow
- 186. Little league elbow
- 190. Coronal short-tau inversion recovery (STIR) images demonstrate osteochondritis dissecans with adjoining marrow edema in the capitulum.
- 192. Hemophilia in a 20-year-old man. Posterior coronal fat-saturated T2-weighted (a) and axial proton density–weighted (b) images demonstrate extensive synovial proliferation (white arrows), predominately low signal intensity, consistent with blood products. Note associated large erosions (black arrows). (c) Coronal localizer gradient echo image demonstrates “blooming” artifact from hemosiderin (white arrows).
- 193. Thank You.