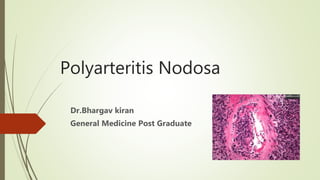
3. Classic polyarteritis nodosa
It is a systemic vasculitis characterized by necrotizing
inflammatory lesions that affect medium-sized and
small muscular arteries.
Preferentially at vessel bifurcations, resulting in
microaneurysm formation, aneurysmal rupture with
hemorrhage, thrombosis, and, consequently, organ
ischemia or infarction.
4. History
Kussmaul and Maier first described PAN in 1866. The
autopsy of a patient with fever, weight loss,
abdominal pain, and polyneuropathy revealed areas
of focal inflammatory exudations that gave rise to
palpable nodules along the course of medium-sized
arteries
5. Epidemiology
Polyarteritis nodosa (PAN) is a rare disease
with an incidence of about 3-4.5 cases per 100,000 population annually
Sex- and age-related demographics
PAN affects men more frequently than women (male-to-female ratio 1.6-2:1).
it is predominantly observed in individuals aged approximately 45-65 years.
6. Pathophysiology
Vascular lesions in medium-sized muscular arteries occur mainly at
bifurcations and branch points.
Inflammation may start in the vessel intima and progress to include
the entire arterial wall, destroying the internal and external elastic
lamina, resulting in fibrinoid necrosis.
Aneurysms develop in the weakened vessel, carrying a subsequent risk
for rupture and hemorrhage.
Thrombi may develop at the site of the lesions
As lesions progress, proliferation of the intima or media may result in
obstruction and subsequent tissue ischemia or infarction.
It spares large vessels (the aorta and its major branches), the smallest
vessels (capillaries and small arterioles), and the venous system.
7. Etiology
Hepatitis B and PAN
The pathogenesis of polyarteritis nodosa (PAN) is unknown,
Hepatitis B virus (HBV) infection is strongly linked with PAN. Evidence for immune
complex–induced disease is confined to HBV-related PAN; the role of immune
complexes in non-HBV-related PAN remains unclear.
Impaired function of endothelial cells may be part of idiopathic PAN or a consequence
of it; in HBV-PAN, virus replication may directly injure the vessel wall.
Endothelial dysfunction can perpetuate the inflammation through cytokine and
adhesion molecule production.
HBV was once the cause of up to 30% of PAN cases.
Widespread use of the hepatitis B vaccine has significantly decreased the incidence of HBV-
PAN, which is now estimated to account for less than 8% of all PAN cases
8. Genetic associations
Loss-of-function mutations in CECR1, the gene that encodes
adenosine deaminase 2 (ADA2), have been associated with a
spectrum of vascular and inflammatory phenotypes that
includes polyarteritis nodosa
Possible roles of ADA2 include regulation of the proliferation
of activated T cells and macrophages and the differentiation
of monocytes to macrophages. Reduction in ADA2
activity may affect the adenosine inflammatory-response
pathway
10. OTHER
the potential association of hepatitis C virus (HCV) with PAN.
INFECTIOUS organisms include varicella-zoster virus,
parvovirus B-19,
cytomegalovirus,
human T-cell leukemia virus,
Streptococcal
species, Klebsiella species, Pseudomonas species, Yersinia species, Toxoplasma
gondii, Rickettsiae, trichinosis, and sarcosporidiosis
Recently, reports of associations with PAN and human immunodeficiency virus and
cutaneous PAN and tuberculosised to cutaneous PAN, a benign, limited form of PAN
Rheumatoid arthritis and Sjögren syndrome have been associated with PAN.
Hematologic malignancies, such as hairy cell leukemia and, in one case,
angioimmunoblastic T cell lymphoma, have been associated with PAN-like vasculitides
11. CLINICAL FEAUTURES
Polyarteritis nodosa (PAN) is an acute multisystem disease with a relatively short prodrome (ie,
weeks to months).
The spectrum of disease ranges from single-organ involvement to fulminant polyvisceral failure.
Pertinent and common historical features of PAN include the following:
Constitutional and musculoskeletal symptoms of PAN include the following:
Fever
Malaise
Fatigue
Anorexia and weight loss
Myalgia
Arthralgia in large joints or, less commonly, arthritis
12. Renal symptoms
About 60% of patients with PAN have renal involvement.
Flank pain may be present.
Ischemic changes in the glomeruli and renal artery vasculitis can cause renal failure,
hypertension, or both.
A small percentage of patients may require dialysis.
Renal symptoms include the following:
Hypertension
Costophrenic tenderness
Retroperitoneal or intraperitoneal hemorrhage
Renal failure
13. Cutaneous symptoms
Dermatologic symptoms are very common in PAN, and about 40% of patients
manifest with skin lesions including
rash,
Purpura
Gangrene
Nodules
cutaneous infarcts
livido reticularis
Raynaud phenomenon.
Skin involvement, which can be painful, occurs most frequently on the legs
14. Cutaneous symptoms in PAN include the
following
Livedo reticularis that does not blanch with active pressure
Ulcerations - Especially on the lower extremities, near the malleoli and on the calf
Digital ischemia - May be accompanied by splinter hemorrhages and, sometimes,
gangrene
Nodules - Usually on the lower extremities (like ulcers); nodules are the least
common skin manifestation of PAN
15. Central nervous system symptoms
Transient symptoms of cerebral ischemia, including typical spells of transient monocular
blindness, are the most common presenting CNS deficits of PAN.
Cerebral arteritis usually presents late in the course of the disease, usually in the second to
third year of the vasculitis.
Cerebral arteritis may cause arterial thrombosis with cerebral ischemia or intraparenchymal
or subarachnoid hemorrhage.
Global CNS dysfunction with encephalopathy and seizures results from metabolic
derangements secondary to multiple organ failure
Acute or subacute myelopathy with paraparesis can occur at any cord level.
Myelopathy may result, although rarely, from cord compression by an extramedullary
hematoma secondary to a ruptured spinal aneurysm.
16. Neurologic symptoms in PAN include the
following:
Sensory and/or motor neuropathies - When these occur, they are usually
asymmetrical
Mononeuritis multiplex (multiple mononeuropathy) - This is the successive
ischemia or infarction of "named nerves" (eg, ulnar, radial, peroneal, sural).
Although nerve involvement is initially asymmetrical, the development of additional
nerve lesions can cause the clinical picture to resemble symmetrical
polyneuropathy.
CNS involvement - Although rare (≤10% of cases), encephalopathy, focal deficits,
strokes, seizures, and, sometimes, brain hemorrhages can occur
17. Peripheral nervous system symptoms
Peripheral neuropathy develops in as many as 60% of patients.
Vasculitic neuropathy is often asymmetrical and presents as
(1) mononeuritis multiplex
(2) distal polyneuropathy
(3) cutaneous neuropathy.
It can take the form of a pure motor, pure sensory, or mixed sensorimotor
polyneuropathy.
18. Gastrointestinal symptoms
GI involvement usually presents as nonspecific symptoms and signs such as
abdominal pain (which may be postprandial)
nausea and vomiting, with or without obvious GI bleeding.
Rare and more serious complications of PAN include
Bowel infarction and perforation
Cholecystitis
Hepatic infarction
Pancreatic infarction
19. Less common symptoms reported in PAN
include the following:
Genitourinary - Patients may develop pain over the testicular or ovarian area. In
rare cases, testicular infarction may occur; testicular pain is usually unilateral
Cardiac - Chest pain, dyspnea, palpitations, pericarditis, myocardial infarction, and
congestive heart failure; cardiac disease affects 35% of patients with PAN, but most
affected patients are asymptomatic
Ophthalmologic - Blurred vision
Neuropsychiatric - Headache, psychosis, and depression
20. Cardiac symptoms include the following:
Hypertension
Tachycardia out of proportion to fever
Pericardial friction rub
Arrhythmias
Congestive heart failure
Ophthalmologic symptoms of PAN include the following:
Retinal vasculitis
Retinal detachment
Cotton-wool spots
22. Diagnosis
Laboratory findings in PAN are nonspecific but can help to establish the systemic
nature of the disease. Findings include the following:
Elevated erythrocyte sedimentation rate (ESR) and/or C-reactive protein - These
markers may be useful in evaluating some patients for active disease but do not
correlate with activity in all patients
Leukocytosis, normochromic anemia, or thrombocytosis
Hepatitis B surface antigen and hepatitic C serologies
Elevated creatinine level
Mild proteinuria
Elevated levels of liver enzymes
Hypergammaglobulinemia - Found in 30% of patients with PAN
Cryoglobulins, circulating immune complexes, and decreased levels of serum
complement (ie, C3, C4) may be observed in patients with HBV-related PAN but are
otherwise uncharacteristic of idiopathic PAN.
23. Arthritis Rheum. 1990;33:1088
ACR Criteria (3 of 10)
Wt loss > 4 kg
Livedo reticularis
Testicular pain
Myalgias, weakness or leg
tenderness
Mononeuropathy or
polyneuropathy
Diastolic BP > 90
BUN or Creatinine
Hepatitis B virus
Arteriographic abnormality
Biopsy of small or medium
artery containing PAN
24. Treatment
Immunosuppression continues to be the standard therapy for polyarteritis nodosa
(PAN).
Corticosteroids plus cyclophosphamide (in the case of steroid-refractory disease
or major organ involvement) can prolong survival for patients with idiopathic PAN.
In contrast, for hepatitis B–related PAN, treatment consists of corticosteroids for
early, initial control followed by plasmapheresis and antiviral agents.
Stronger immunosuppression using a combinations of steroids and
cyclophosphamide is typically avoided in these cases as it can enhance viral
replication
25. Prognosis
Idiopathic (non–HBV-related) PAN
Traditionally, it has been taught that relapses of polyarteritis nodosa (PAN) are rare in
individuals who completely recover
Recovery from neurologic deficits due to PAN can take up to 18 months. Central
nervous system (CNS) involvement carries a worse prognosis than does peripheral nerve
involvement.
The prognosis is markedly worse in patients with acute abdominal syndromes
characterized by extensive bowel involvement.
Multiple perforations may be found, relapses are common, and the postoperative course is
complicated by infections and delayed healing.
The prognosis is better in patients with cutaneous PAN without systemic involvement. This disease
is benign but tends to relapse
26. HBV-related PAN
Patients who seroconvert usually recover.
Once HBV-PAN goes into remission, the risk of recurrence is very low
HCV-related PAN
One study found that in patients with HCV-related vasculitis, HCV-PAN exhibits a
more severe clinical presentation but a higher rate of clinical remission.