
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Parotidectomy
Similar to Parotidectomy (20)
Recently uploaded
Recently uploaded (20)
Parotidectomy
- 2. INTRODUCTION • A parotidectomy is the surgical excision (removal) of the parotid gland, the major and largest of the salivary glands. • The procedure is most typically performed due to benign or malignant tumors. • The majority of parotid gland tumors are benign, however 20% of parotid tumors are found to be malignant.
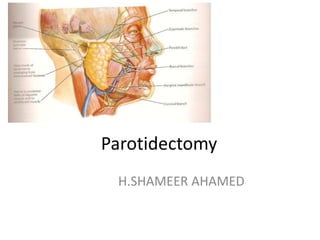
- 4. Parotid gland is divided by the facial nerve into i. a superficial lobe ii. a deep lobe
- 6. Relevant surgical relations • Posterior: Cartilage of external auditory meatus; tympanic bone, mastoid process, sternocleidomastoid muscle • Deep: Styloid process, stylomandibular tunnel, parapharyngeal space, posterior belly of digastric, sternocleidomastoid muscle • Superior: Zygomatic arch, temporomandibular joint
- 7. TYPES
- 8. • Partial parotidectomy: Resection of parotid pathology with a margin of normal parotid tissue. This is the standard operation for benign pathology and low grade malignancies • Superficial parotidectomy: Resection of the entire superficial lobe of parotid and is generally used for metastases to parotid lymph nodes e.g. from skin cancers, and for high grade malignant parotid tumors.
- 9. • Total parotidectomy: This involves resection of the entire parotid gland, usually with preservation of the facial nerve • Extended Total Parotidectomy: Removal of the superficial and deep parotid gland also may be extended to involve adjacent structures such as the overlying skin, the underlying mandible, the temporal bone and external auditory canal, or the deep musculature of the parapharyngeal space.
- 10. CONSENT • Scar • Anaesthesia –greater auricular region • Facial nerve weakness • Facial contour • Frey's syndrome • Prominence of auricle • Salivary fistula
- 11. PREPARATION Intraoperative facial nerve monitoring. • for patients with large and/or malignant tumours, • undergoing revision surgery, • retrograde dissection of the facial nerve, • less experienced surgeons. The facial nerve monitor should be applied and testing prior to prepping and draping the patient.
- 12. ANAESTHESIA • General anaesthesia • Short acting muscle relaxant for intubation only if nerve monitoring planned
- 13. POSITION AND INFILTRATION • Supine • Hyper extend the head and turn to opposite side • Infiltrate along planned skin incision • Keep corner of eye and mouth exposed so as to be able to see facial movement
- 14. Superficial Parotidectomy • The most common indications are: 1. Benign or low grade tumor of the superficial lobe of the parotid gland 2. metastases to parotid lymph nodes from adjacent sites of skin cancer or melanoma, or from cancer of the external auditory meatus. 3. Access to the deep lobe of the gland or other structures deep to the facial nerve. 4. Chronic inflammation of parotid gland, resistant to conservative treatment.
- 15. INCISION Modified Blair incision • An incision should be carefully marked out extending from • the preauricular region, around the lobule of the ear towards the mastoid tip, and then curving back down to join a neck crease, well below the angle of the mandible. • If a preauricular crease is present, this should be used.
- 16. ALTERNATIVE INCISION • Face lift incision : here the pre auricular portion of the incision passes on or just inside the tragal margin. The incision is then carried below the lobule of the ear , turned posteriorly over the mastoid, and extended within the hairline. • Unlike Blair's incision which has cervical extension the facelift incision extends posteriorly and inferiorly along the hairline. • Less conspicuous and hence offers better cosmesis.
- 17. FLAPS In the face, • The anterior skin flap should be raised superficial to the parotid fascia, leaving subcutaneous fat on the flap. • very easy to buttonhole this flap. • If the surgeon sees hair follicles, he is probably getting too superficial.
- 18. In the neck, • the flap may be raised either superficial or immediately deep to the platysma. • A 'white line' which defines the plane the surgeon needs to be in is usually apparent between these facial and neck planes. • When raising the flap, it is of utmost importance that the surgeon keeps palpating the tumour.
- 19. Posteriorly, in the neck The incision should be deepened to the sternomastoid muscle. The greater auricular nerve can be seen. This is usually sacrificed. The anterior border of the sternomastoid should be defined and followed up to the mastoid tip. The fascia should be raised anteriorly off the sternomastoid muscle. Stay behind any posterior extension of the parotid gland or the tumour. Be aware of the proximity of the accessory nerve while dissecting on the medial surface of the sternomastoid muscle. The deep cervical fascia should then be incised to display the posterior belly of the digastric muscle, which is an important landmark.
- 20. In the region of the ear, • The incision should be deepened along the cartilage of the external auditory canal, taking care not to damage this cartilage. • As long as the surgeon stays right on the external auditory canal, the incision can be safely deepened all the way to the bony-cartilaginous junction. • The surgeon should look out for the 'tragal pointer', which is another useful landmark for the facial nerve.
- 21. At this point, • Divide the tissue anterior to the mastoid process in order to join the dissection in the region of the external auditory canal to that in the region of the sternomastoid muscle. • The depth of this should remain superficial to the digastric muscle. • There are many blood vessels around the mastoid.
- 22. LOCATING THE FACIAL NERVE • The facial nerve emerges from the stylomastoid foramen just superior to the posterior belly of the digastric muscle, at the same depth as this muscle. • The tragal pointer is 1 cm superficial and above this point. • The styloid process is medial to the facial nerve.
- 23. • Open a broad plane of dissection, do not work down a narrow 'hole'. • This may be opened gently in a direction parallel to the nerve to avoid causing inadvertent damage. • There are usually many fibrous strands in the region of the nerve which will need to be divided in order to find the nerve.
- 24. • In addition, there are usually some blood vessels just superficial to the nerve. • It is best-to divide these blood vessels after cauterizing them using bipolar diathermy. • Be certain that the- facial nerve is not cauterized. • Once the facial nerve is found, it should be followed to its bifurcation, prior to division of any parotid tissue.
- 25. FOLLOWING THE BRANCHES • The branches should be followed in sequence, starting either superiorly or inferiorly. • A clamp should be inserted along the nerve, then lifted away from the nerve and opened. • The surgeon should remember that as the branches are traced distally, they become more superficial, particularly the upper branches.
- 26. • The dissection should commence over a branch which is clear of the tumour, and then proceed to the successive branches. • In so doing, parotid tissue should be divided clear of the tumour. • The surgeon may come towards the tumour both superiorly and inferiorly, so the superficial lobe is well mobilized by the time the tumour is approached.
- 27. • For tumours located in either the upper or lower pole of the gland, it is not necessary to remove the whole of the superficial lobe. • It may be possible to remove the tumour with an adequate cuff while following only either the upper or lower division branches. • If the deep part of the tumour capsule is applied directly onto the branches of the facial nerve, the surgeon should carefully separate the tumour from the nerve, taking great care not to rupture the capsule.
- 28. CLOSURE • Prior to closure, a drain should always be placed, as otherwise the wound will inevitably accumulate saliva and serous fluid. • The drain should be ideally left for at least 48 hours. • Closure is then performed according to surgeon's preference.
- 29. DEEP LOBE TUMOURS – TOTAL PAROTIDECTOMY • INDICATIONS: 1. Metastasis to a superficial parotid node from a primary parotid tumor or an extraparotid malignancy 2. Parotid malignancy that indicates metastasis by involvement of cervical lymph nodes 3. High-grade parotid malignancy with a high risk of metastasis. 4. Primary parotid malignancies originating in the deep lobe and for primary malignancies that extend outside the parotid gland. 5. Multifocal tumors, such as oncocytomas, to ensure complete removal.
- 30. • The operation begins with a standard superficial parotidectomy. • The branches of the facial nerve overlying the tumour are now easily visible and are then separated from the tumour and mobilized. • The tumour is then removed between two of the mobilized facial nerve branches. • It may be necessary to sacrifice some of the minor communicating branches, although this should, if possible, be avoided. • The underlying tumour is then mobilized and separated from the deep tissue.
- 32. REVISION CASES • It will be necessary to resect the previous scar. should be prepared to reconstruct the defect. • If the previous surgery comprised a formal superficial parotidectomy, then the branches of the facial nerve will be just beneath the skin flap, without any intervening parotid fascia, and so will be vulnerable to injury while raising the skin flap. • Extending the previous incision, and identifying the correct plane in virgin tissue, may be a useful manoeuvre. • Identification of the main trunk of the facial nerve may be difficult or impossible due to scarring. • In such cases, it may be necessary to identify the branches of the facial nerve in the neck and/or face and perform retrograde dissection.
- 33. • The retromandibular vein, if still present, is a useful landmark as the marginal mandibular and cervical branches pass directly over it. • If this vein has been previously ligated, then the marginal mandibular nerve may be identified beneath the angle of the mandible, or crossing the facial artery at the mandibular notch on the inferior border of the mandible. • The cervical branch is a variable distance below the marginal mandibular branch. • The temporal branch crosses the zygomatic arch 1 cm anterior to the ear, and courses superficial to the deep temporal fascia, within 1.5 cm of the lateral border of the eye. • The zygomatic branch crosses the zygomatic arch further forward. • The upper buccal branch runs forward roughly 1 cm below the zygomatic arch • the lower buccal branch runs towards the corner of the mouth. • These nerves are superficial to the masseter muscle. • Retrograde dissection of the branches of the facial nerve may lead to a higher incidence of neuropraxia than traditional prograde dissection.
- 34. Complications of parotid surgery • Early – Anaesthesia – Haemorrhage – Trauma to adjacent structures • Intermediate – hematoma – Facial palsy • Late – Salivary fistula – Gustatory sweating – cosmesis
- 35. FACIAL NERVE INJURY • Facial nerve injury is usually the biggest concern in parotid surgery. • Postoperative weakness may be temporary, if the injury is a neuropraxia. • more common - between 10 and 50 per cent • The precise cause of neuropraxia is not known, but probably results from a combination of trauma while dissecting right on the nerve, traction injury to the nerve, heat injury secondary to the use of cautery, and prolonged operating time. • The lower division branches, in particular, the marginal mandibular branch
- 36. • Permanent, due to transection of, or cautery injury to, the main trunk of the facial nerve, or, more commonly, one of the terminal branches. • More commonly in difficult cases, i.e. large tumours, tumours located in the deep lobe, malignant cases and revision surgery. • The incidence of permanent facial nerve injury is generally reported as 0-5 percent
- 37. HAEMATOMA • up to 5 percent. • Small haematomas should be evacuated promptly, as their presence leads to compromise of the skin flap with possible necrosis.
- 38. SEROMA/SAIIVOMA/SALIVARY FISTULA • After superficial parotidectomy, leakage of serous fluid and saliva from the transected parotid tissue is expected • This usually lasts for a few days. • Thus, a drainshould always be placed after parotid surgery and left in place for at least 2-3 days. • At this stage, the skin flap should have begun to adhere to the parotid bed, so obliterating the dead space in which fluid can accumulate.
- 39. • If, after removing the drain, patients develop swelling underneath the wound, this should be aspirated. • Seromas usually resolve within a few days of serial aspiration.
- 40. • Drainage of saliva out of the drain site or through the wound when the patient is eating is not uncommon. • A pressure dressing, similar to the type used after otoplasty, may also be useful to speed resolution.
- 41. FREY'S SYNDROME/ gustatory sweating • Is a phenomenon seen after parotid surgery where the patient develops sweating on the side of the face while eating.
- 42. • Due to transection of cholinergic secretomotor fibres to the secretory units of the parotid gland, which subsequently sprout new axons and come to innervate sweat glands in the skin flap, which are also responsive to acetylcholine. • Around 10 per cent of patients who undergo parotidectomy will complain of gustatory sweating.
- 43. • Objective demonstration is possible using Minor's starch- iodine test. • This is performed by covering the affected skin with iodine solution. Once this has dried, it is dusted with starch powder, and the patient given a lemon sweet. As a result of absorption of the wet iodine by starch, the affected area will turn deep blue purple.
- 44. • These include raising a thick skin flap, rotation of a superficial temporal artery-based temporoparietal vascular flap, rotation of the superficial musculoaponeurotic system (SMAS), and rotation of sternomastoid muscle flaps. • Topical anticholinergics may be useful, but have variable efficacy and may lead to anticholinergic side effects. • For persistent cases, the most effective treatment would appear to be injection of botulinum tvpe A toxin. This inhibits neurotransmitter release and gives long lasting relief, and may be repeated if recurrent symptoms develop. • Antiperspirants : Glycopyrrolate 1% lotion • Tympanic neurectomy
- 45. OTHER • Ear numbness is an expected outcome from parotid surgery. It results from transection of the greater auricular nerve. Patients are usually very aware of sensory change immediately after the surgery. Over the course of several months, the area of numbness diminishes, but patients are usually left with an area of persistent numbness around the ear lobe. Patients who wear earrings will not be able to insert them without looking in a mirror. • Duskiness of the postauricular skin flap may occur if the flap is too large or the blade of the knife was bevelled while making the skin incision. This usually settles spontaneously.
- 46. • Necrosis of the skin tip can occur; this will usually heal by secondary intention. • In patients with bulky parotids, a sizeable 'hollow' may be left on the side of the head after surgery, particularly after more extensive resections.
- 47. REFERENCES • STELL AND MARAN • SCOTT BROWN 7TH EDITION • Salivary Gland Disorders: Eugene N. Myers, Robert L. Ferris; Springer. • Otolaryngology clinics of north america; Management of neck in salivary gland cancers: 38(2005) 99-105 • Cumming’s text book of Otolaryngology & head and neck surgery • Internet