Tachyarrhythmias questions. by st jude. arranged by prof. samir rafla
•
1 like•567 views

Teaching tachyarrhythmia diagnosis.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Tachyarrhythmias questions. by st jude. arranged by prof. samir rafla
Similar to Tachyarrhythmias questions. by st jude. arranged by prof. samir rafla (20)
More from Alexandria University, Egypt
More from Alexandria University, Egypt (20)
Recently uploaded
Recently uploaded (20)
Tachyarrhythmias questions. by st jude. arranged by prof. samir rafla
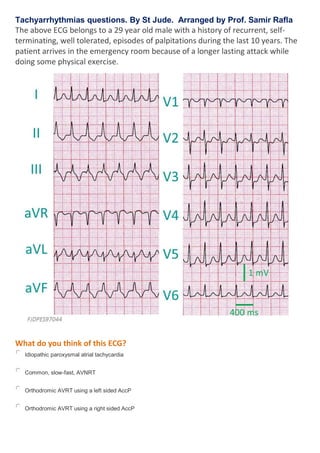
- 1. Tachyarrhythmias questions. By St Jude. Arranged by Prof. Samir Rafla The above ECG belongs to a 29 year old male with a history of recurrent, self- terminating, well tolerated, episodes of palpitations during the last 10 years. The patient arrives in the emergency room because of a longer lasting attack while doing some physical exercise. What do you think of this ECG? Idiopathic paroxysmal atrial tachycardia Common, slow-fast, AVNRT Orthodromic AVRT using a left sided AccP Orthodromic AVRT using a right sided AccP
- 2. This is an example of AVRT using a right sided accessory pathway. The ECG of this patient shows a regular, narrow QRS-complex, supraventricular tachycardia. The first step trying to determine the mechanism and pathway of this tachycardia should be to identify ‘P-waves’. The steps to follow are summarized below. In narrow QRS-complex regular SVT sometimes it is difficult to identify with certainty the presence of P-waves. Our patient is one of such cases. As shown below in the inferior leads we suspect the presence of negative P-waves some 80 ms after the end of the QRS complex. In V1, there seems to be a negative, bimodal, P-wave, also some 80 ms after the end of each QRS complex. We understand that there is a certain degree of insecurity about the above identification of P-waves during tachycardia, and we must say that some experience is needed to suspect the presence of P-waves during certain episodes of narrow QRS-complex regular tachycardia. This requirement, a critical level of expertise, is not usually acknowledged in the teaching algorithms used to guide in the diagnosis of narrow QRS-complex regular tachycardia. This is the reason why we have included in the above algorithm the scenario of ‘P-waves not identified but present’. We have discussed this case in our teaching sessions, and many of the attendees thought that a P-wave was not visible during this tachycardia. If the referred waveforms are P-waves we would be dealing with a 1:1 AV ratio during tachycardia and then we would identify the tachycardia as one in which RP interval is shorter than the PR time. AVRT using an accessory pathway as retrograde limb of the junctional reentry mechanism, direction or the so-called
- 3. ‘slow-slow’ form of AVNRT can result in this pattern of SVT with RP<PR. Atrial tachycardia would very exceptionally result in this P-to-QRS relationship and only when there is concomitant AV nodal disease of use of drugs severely depressing AV nodal conduction. A suspected negative P-wave in the inferior leads during a SVT with RP<PR is compatible with AVRT and AVNRT. However, a negative, bimodal P-wave in V1, 80 ms after the end of the QRS complex (with an RP<PR), is not compatible with any form of AV nodal reentry tachycardia. AVNRT produces positive P-waves in lead V1. This negative, bimodal, configuration of the P-wave during AVRT was described by García-Civera and coworkers, as very suggestive for the utilization of a right sided, AV accessory pathway as retrograde link of the reentry circuit (Eur Heart J. 1980 Apr; 1(2): 137-45). Left sided accessory pathways produce positive P-waves in V1.
- 4. In summary, this is a narrow QRS complex tachycardia at a rate of 170 bpm (cycle length of 350 ms) in which identification of P-waves is difficult but there seems to be negative P-waves superimposed on negative T-waves in leads III and aVF, as well as negative, bimodal, P-waves in V1, both of them recorded some 80 ms after the end of the QRS complex during tachycardia this SVT with an RP<PR and negative bimodal P-waves in V1 after the QRS complex cannot be an AVRT using a left sided accessory pathway or a slow- slow AVNRT because in both instances the retrograde P-wave could not be negative and bimodal in lead V1 the presence of negative bimodal P-waves after the QRS complex with an RP<PR is consistent with and AVRT using a right sided accessory pathway The tachycardia was interrupted by IV verapamil and see how was the ECG in sinus rhythm.
- 5. What do you think of this ECG? Complete LBBB Complete LBBB and inferior wall myocardial infarction Accessory pathway with Mahaim physiology None of the above What do you think of this ECG? If your reply is one of the following Complete LBBB Complete LBBB and inferior wall myocardial infarction Accessory pathway with Mahaim physiology This is not correct. Go to the next screen.
- 6. Some comments on this ECG This is the typical ECG of a WPW syndrome For those of you that have said LBBB, it is of interest to remember that the title of the paper by Wolff, Parkinson, and White published in 1930 was: ‘Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia’ [Am Heart J 1930; 5: 685] o The ECG pattern of ventricular preexcitation has in common with that of a bundle branch block, the existence of a wide QRS complex o In BBB the PR interval is normal and in ventricular preexcitation it is usually, but not always, short o In our case, the QRS complex was 130 ms in duration and the PR interval measured 110 ms In accessory pathways with a ‘Mahaim’ physiology, the ECG in sinus rhythm is different: either preexcitation is not evident or it is less evident than in this case, and the PR interval is not short
- 7. This is an example of ventricular preexcitation due to a normal type of accessory atrioventricular pathway with short conduction times Where is the accessory AV pathway located? Right superior (formerly right anterior) Right anterior (formerly right lateral) Right inferior (formerly right posterior) Right inferior paraseptal Right septal (midseptal) Right superior paraseptal (anteroseptal) Where is the accessory AV pathway located? Right inferior (formerly right posterior) Traditionally, the terms used to name the locations of the accessory AV pathways derived from the terminology introduced during the late 1970’s and the 1980’s
- 8. to pinpoint accessory pathways in the surgically exposed heart. The above illustration summarizes such ‘surgically-oriented’ nomenclature: anteroseptal region was considered to extend from the central fibrous body to the epicardial reflection of the most superior area of the right ventricle, this being the extension of the supraventricular crest into the free wall of the ventricle right-sided free wall extended from the anteroseptal region to the inferior hinge of the septal leaflet of the tricuspid valve; the right-sided free-wall was further subdivided into a right anterior, right lateral, and right posterior areas posteroseptal region included the pyramidal space, interposed between the central fibrous body and the hinges of the facing leaflets of the mitral and tricuspid valves, to the epicardial confluence of the right and left ventricles in the postero-inferior AV groove left-sided free-wall region comprised the arc of the left AV groove from the point of continuity between the leaflets of the aortic and mitral valves to the ventricular septum; the left free-wall was also segmented into left posterior, left lateral, and left anterior territories intermediate septal region was a concept introduced by John Gallagher, while at Duke University, to designate accessory pathways that had an anterograde exit in the anteroseptal region, but a retrograde breakthrough close to the coronary sinus, as for posteroseptal pathways (details of these accessory pathways were presented at the Scientific Sessions of the American Heart Association of 1986, but never published as a full paper); the same terminology was subsequently used by used by Epstein et al, from Birmingham, Alabama, to name 3 accessory pathways located in the middle of the triangle of Koch and an additional bypass found in the peri- Hisian region midseptal region was a term used by Jackman et al, from Oklahoma for accessory pathways located in the triangle of Koch, behind the His bundle, and anterior to the mouth of the coronary sinus; the midseptal concept applied to the 3 cases in the middle of the triangle of Koch named as the intermediate septal by Epstein but most likely cannot be assimilated to the cases of Gallagher Gallagher JJ, Selle JG, Sealy WC, Fedor JM, Svenson RH, Zimmern SH. Intermediate septal accessory pathways (IS-AP): a subset of preexcitation at risk for complete heart block/failure during WPW surgery (abstract). Circulation 1986; 74 (suppl II): II-387.
- 9. Epstein AE, Kirklin JK, Holman WL, Plumb VJ, Kay GN. Intermediate septal accessory pathways: electrocardiographic characteristics, electrophysiologic observations and their surgical implications. J Am Coll Cardiol. 1991; 17: 1570-8. Jackman WM, Friday KJ, Fitzgerald DM, Bowman AJ, Yeung-Lai-Wai JA, Lazzara R. Localization of left free- wall and posteroseptal accessory atrioventricular pathways by direct recording of accessory pathway activation. Pacing Clin Electrophysiol. 1989; 12: 204-14. In 1999, the Working Group of Arrhythmias of the European Society of Cardiology, and of the Task Force on Cardiac Nomenclature from North American Society of Pacing and Electrophysiology, endorsed the use of a new nomenclature that was named ‘anatomically correct’. It is probably more correct to refer to this new terminology as ‘attitudinally-oriented nomenclature’, as suggested by McAlpine in 1995 because any reference to structures within the human body should be described relative to the subject as seen in an upright position. As shown in the above illustration, the left anterior oblique (LAO) projection enables us to see the tricuspid AV junction almost parallel to our plane of observation enabling us to define 5 sectors in the right junction: right superior (RS) right superoanterior (SA) right anterior (A) right anteroinferior (AI), and right inferior (RI) Note that positions that, in the traditional nomenclature, were considered as anterior are, in fact, superior and that accessory pathways previously referred to as being right lateral are right and anterior. The LAO projection is again almost parallel to the plane of the mitral AV junction, and this permits us to define 5 sectors in its free-wall: left inferior (LI) left infero-posterior (IP) left posterior (P) left postero-superior (PS), and left superior (LS) Note also that positions traditionally labelled as left lateral are, in fact, left posterior. The septal region was not well defined in the publication introducing the new nomenclature:
- 10. superior paraseptal (SPS): includes the area initially considered to be anteroseptal Septal (S): includes pathways traditionally considered to be midseptal right inferior paraseptal (RIPS), left inferior paraseptal (LIPS), and inferior paraseptal (IPS): these terms refer to accessory pathways formerly grouped together as being posteroseptal Right inferior paraseptal pathways connect the caudal right atrial myocardium with the right ventricular aspect of the ventricular septum, running outside the coronary sinus. The inferior paraseptal accessory pathways are those that are ablated within the coronary sinus or its tributaries, usually the middle cardiac vein. We will review some aspects of the septal accessory pathway in a specific essay. For a detailed introduction on this matter consult Farré et al. Cosio FG, Anderson RH, Kuck KH, Becker A, Borggrefe M, Campbell RW, Gaita F, Guiraudon GM, Haissaguerre M, Rufilanchas JJ, Thiene G, Wellens HJ, Langberg J, Benditt DG, Bharati S, Klein G, Marchlinski F, Saksena S. Living anatomy of the atrioventricular junctions. A guide to electrophysiologic mapping. A Consensus Statement from the Cardiac Nomenclature Study Group, Working Group of Arrhythmias, European Society of Cardiology, and the Task Force on Cardiac Nomenclature from NASPE. Circulation. 1999; 100: e31-e7
- 11. In the above illustration we present the RAO and LAO fluorographic projections displaying the position of the ablation catheter at the site of the application of radiofrequency current that permanently blocked the accessory pathway. On the right we present two anatomic slices obtained with a RAO and LAO tilt similar to that of the fluoroscopic images. The accessory pathway had a right inferior location or anteroinferior location. These two anatomical slices, and other similar sections in various projections have been obtained using theVisible Human Slice and Surface Server, an open-access, web-based, software developed by Hersch and co-workers from the Geneva Hospitals and WDS Technologies SA using data sets of the Visible Human Male and Female Project of the National Library of Medicine, USA. The Visible Human Slice and Surface Server is available at a web-server, and any registered client can obtain slices with the desired orientation from a male and a female body. End of ECG exercise 'tachyarrhythmias III