Hope on the Horizon for Hidradenitis Suppurativa: Leveraging Emerging Biologics to Improve Quality of Life
•
0 gefällt mir•101 views

Chair & Presenter, Vivian Y. Shi, MD, FAAD, and Jennifer Hsiao, MD, prepared useful Practice Aids pertaining to hidradenitis suppurativa for this CME activity titled “Hope on the Horizon for Hidradenitis Suppurativa: Leveraging Emerging Biologics to Improve Quality of Life.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/3c2uXCE. CME credit will be available until December 5, 2023.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie Hope on the Horizon for Hidradenitis Suppurativa: Leveraging Emerging Biologics to Improve Quality of Life
Ähnlich wie Hope on the Horizon for Hidradenitis Suppurativa: Leveraging Emerging Biologics to Improve Quality of Life (20)
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Hope on the Horizon for Hidradenitis Suppurativa: Leveraging Emerging Biologics to Improve Quality of Life
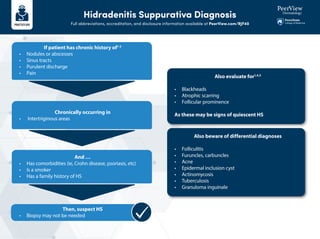
- 1. Hidradenitis Suppurativa Diagnosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 If patient has chronic history of1-3 • Nodules or abscesses • Sinus tracts • Purulent discharge • Pain Also evaluate for1,4,5 • Blackheads • Atrophic scarring • Follicular prominence As these may be signs of quiescent HS Also beware of differential diagnoses • Folliculitis • Furuncles, carbuncles • Acne • Epidermal inclusion cyst • Actinomycosis • Tuberculosis • Granuloma inguinale And … • Has comorbidities (ie, Crohn disease, psoriasis, etc) • Is a smoker • Has a family history of HS Chronically occurring in • Intertriginous areas Then, suspect HS • Biopsy may not be needed
- 2. Hidradenitis Suppurativa Diagnosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 Hidradenitis Suppurativa Diagnosis1,4,5 Chronicity; relapsing/remitting Inquire about • Length of symptoms • Prior diagnoses • Pain • Discharge • Smoking status • Weight • Family history of HS • Comorbidities (ie, Crohn disease, psoriasis, etc) Commonly appears in axillae, anogenital, inframammary areas, but can appear elsewhere Abscesses or nodules Sinus tracts Quiescent disease • Blackheads • Atrophic scarring • Follicular prominence Purulent discharge
- 3. Hidradenitis Suppurativa Diagnosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 Differential Diagnosis5,6,7 Early-Stage Hidradenitis Suppurativa Late-Stage Hidradenitis Suppurativa • Folliculitis • Furuncles, carbuncles • Acne • Epidermal inclusion cyst • Pilonidal cyst • Perirectal abscess • Erysipelas • Actinomycosis • Granuloma inguinale • Lymphogranuloma venereum • Cat scratch disease • Cutaneous Crohn disease • Pilonidal disease • Tuberculosis 1. https://www.aad.org/public/diseases/a-z/hidradenitis-suppurativa-symptoms. 2. Lee EY et al. Can Fam Physician. 2017;63:114-120. 3. Scuderi N et al. Skin Appendage Dis. 2017;3:95-110.4. Čagalj AM et al. Int J Mol Sci. 2022;23:3753. 5. Micheletti R. Semin Cutan Med Surg. 2014:33:S51-S53. 6. Dufour DN et al. Postgrad Med J. 2014;90:216-221. 7. Alikhan A et al. J Am Acad Dermatol. 2009;60:539-561.
- 4. Hidradenitis Suppurativa Management Algorithm1,2 Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 Hurley Stage 1 Mild (nodules and abscesses) Hurley Stage 2 Moderate (nodules, abscesses, and scars or tunnels) Hurley Stage 3 Severe (nodules, abscesses, and connecting tunnels) Lifestyle Modification and General Treatment Medical Treatment Surgical and Laser Treatment • Smoking cessation • Body weight reduction • Advise wearing loose clothing to avoid friction with skin Hormonal therapies Retinoids Topical antibiotics or disinfection (eg, clindamycin [1%] twice daily for 12 wk) Intralesional steroids for short-term control of acute and recalcitrant lesions Zinc gluconate Systemic Antibiotics: Tetracyclines (eg, doxycycline 50-100 mg BID) Systemic Antibiotics: Clindamycin 300 mg BID and rifampicin 300 mg BID for 12 wk Other biologics: secukinumab, ustekinumab, anakinraa TNF-α Inhibitors: Adalimumab for 12 wk followed by assessment (wk 0 160 mg subQ, wk 2 80 mg subQ, then weekly 40 mg subQ) or infliximab 5 mg/kg IV on wk 0, 2, 6, and Q8W thereafter Local Procedures for Localized Stationary and Recurrent Nodules and for Abscesses: excision; carbon dioxide laser evaporation of diseased tissue; drainage of fluctuating abscesses Local Procedures for Sinus Tracts: deroofing of sinus tracts; sinus tract excisions; carbon dioxide laser evaporation of diseased tissue Wide local excisions with healing by secondary intention or primary closure/flap/graft Other Possible Systemic Therapies: Dapsone 25-200 mg daily; acitretin 0.2-0.5 mg/kg daily; prednisone 40-60 mg daily for 3-4 d then taper; cyclosporine 3-5 mg/kg daily • Advise antiseptic wash to keep skin clean to reduce odor (eg, triclosan) • Refer to psychosocial support as needed • Pain management a Not yet FDA-approved for HS. 1. Adapted from Jafari SMS et al. Front Med (Lausanne). 2020 Mar 4;7:68. 2. Alikhan A et al. J Amer Acad Derm. 2019;811:91-101.
- 5. Comparative Dosing, Efficacy, Safety, and MOA of Biologic and Small Molecule Therapies for Hidradenitis Suppurativaa Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 Adalimumab1,2 TNF inhibitor PIONEER I and PIONEER II • Period 1: 40 mg weekly for 12 wk • Period 2: weekly or every other wk for 24 wk Through wk 168 300 mg Q2W or Q4W through wk 16 300 mg Q2W or Q4W through wk 16 • Bimekizumab: 640 mg wk 0, 320 mg Q2W • Adalimumab: 160 mg wk 0, 80 mg wk 2, 40 mg every wk for wk 4-10 • PIONEER I: HiSCR at wk 12: 41.8% adalimumab vs 26.0% PBO • PIONEER 2: HiSCR at wk 12: 58.9% adalimumab vs 27.6% PBO • HiSCR at wk 16 (Q2W): 45.0% secukinumab vs 33.7% PBO • Q4W: 41.8% secukinumab • HiSCR at wk 16 (Q2W): 45.0% secukinumab vs 31.2% PBO • Q4W: 41.8% secukinumab • HiSCR all responders at wk 12: 60% bimekizumab and adalimumab vs 22% PBO • HiSCR90 responders: 30% bimekizumab vs 18% adalimumab vs 0% PBO • HiSCR at wk 168: 52% adalimumab and 57% responders + partial responders Phase 3 RCT 307, 327 No differences between groups No differences between groups No new safety signals No new safety signals TEAEs similar among groups 151 >500 >500 84 Phase 3 OLE; uncontrolled Phase 2 RCT vs adalimumab and PBO Phase 3 RCT Phase 3 RCT PIONEER III SUNSHINE SUNRISE N/A IL-17A inhibitor IL-17A/17F inhibitor Secukinumab3,4 Bimekizumab5 Agent Class/MOA Trial Name Trial Type N Dosing Efficacy Safety
- 6. Comparative Dosing, Efficacy, Safety, and MOA of Biologic and Small Molecule Therapies for Hidradenitis Suppurativaa Full abbreviations, accreditation, and disclosure information available at PeerView.com/RJF40 a Only adalimumab is FDA-approved for HS. 1. Kimball AB et al. N Engl J Med. 2016;375:422-434. 2. Zouboulis CC et al. J Amer Acad Derm. 2019;80:60-69. 3. Kimball AB et al EADV 2022. Abstract LB-3549. 4. https://www.emjreviews.com/dermatology/abstract/secukinumab-in-moderate-to-severe-hidradenitis-suppurativa-primary- endpoint-analysis-from-the-sunshine-and-sunrise-phase-iii-trials-j0301225. 5. Glatt S et al. JAMA Dermatol. 2021;157:1279-1288. 6. Gottlieb A et al. J Invest Dermatol. 2020;140:1538-1545. 7. https://clinicaltrials.gov/ct2/show/NCT04988308. 8. Grant A et al. J Am Acad Dermatol. 2010;62:205-217. 9. Tzanetakou V et al. JAMA Dermatol. 2016;152:52-59. 10. Blok JL et al. Br J Dermatol. 2016;174:839-846. Agent Bermekimab6,7 Infliximab8 Anakinra9 Ustekinumab10 Il-1α inhibitor TNF inhibitor IL-1 antagonist IL-12/23 inhibitor Phase 2 (open-label): anti-TNF–naïve vs failed; no PBO Phase 2 Phase 2 Phase 2 (open-label) Injection-site reactions 30% decrease in lesion count in naïve group vs 60% in failed group; HiSCR at wk 12 ~60% both groups _ _ _ _ 42 38 20 12 400 mg weekly • Wk 0, 2, 6: 5 mg/kg • Wk 8: crossover; Q8W through wk 22 • Wk 22 and 30: maintenance regimen 26.7% of infliximab patients had ≥50% decrease in HSSI vs 5% with PBO Infusion-site reactions; infections Injection-site pain; mild infections Upper respiratory tract infections Disease activity score decreased in 67% in anakinra patients vs 20% with PBO 47% achieved HiSCR50 at wk 40 100 mg subQ once daily for 12 wk 45mg subQ if <90kg and 90mg if >90kg at wk 0, 4, 16, and 28 Class/MOA Trial Name Trial Type N Dosing Efficacy Safety