Hitting the BCMA Target in Multiple Myeloma: Insights on CAR-T Therapy and Innovative Antibody Options
•
0 likes•75 views

This document summarizes BCMA antibody and CAR-T cell therapies for multiple myeloma. It provides regulatory status, dosing details, and safety considerations for four BCMA antibody therapies - elranatamab, linvoseltamab, teclistamab, and ABBV-383. It also reviews dosing ranges and general safety principles for the two FDA-approved CAR-T cell therapies ciltacabtagene autoleucel and idecabtagene vicleucel. Both CAR-T therapies require administration through a Risk Evaluation and Mitigation Strategy program due to risks of cytokine release syndrome and neurologic toxicities.

Recommended
Recommended
More Related Content
Similar to Hitting the BCMA Target in Multiple Myeloma: Insights on CAR-T Therapy and Innovative Antibody Options
Similar to Hitting the BCMA Target in Multiple Myeloma: Insights on CAR-T Therapy and Innovative Antibody Options (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Hitting the BCMA Target in Multiple Myeloma: Insights on CAR-T Therapy and Innovative Antibody Options
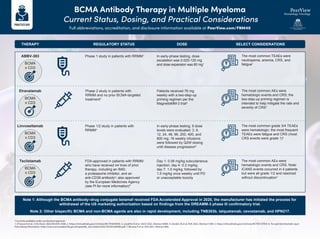
- 1. BCMA Antibody Therapy in Multiple Myeloma Current Status, Dosing, and Practical Considerations Full abbreviations, accreditation, and disclosure information available at PeerView.com/FNM40 a Currently available under accelerated approval. 1. D'Souza A et al. J Clin Oncol. 2022;40:3576-3586. 2. https://clinicaltrials.gov/ct2/show/NCT04649359. 3. Lesokhin A et al. ASCO 2022. Abstract 8006. 4. Zonder JA et al. EHA 2022. Abstract S189. 5. https://clinicaltrials.gov/ct2/show/NCT05137054. 6. Tecvayli (teclistamab-cqyv) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761291s000lbl.pdf. 7. Moreau P et al. ASH 2021. Abstract 896. REGULATORY STATUS Phase 2 study in patients with RRMM and no prior BCMA-targeted treatment2 Phase 1/2 study in patients with RRMM4 FDA-approved in patients with RRMM who have received ≥4 lines of prior therapy, including an IMiD, a proteasome inhibitor, and an anti-CD38 antibodya ; also approved by the European Medicines Agency (see PI for more information)6 Phase 1 study in patients with RRMM1 DOSE Patients received 76 mg weekly with a two-step-up priming regimen per the MagnetisMM-3 trial3 In early-phase testing, 9 dose levels were evaluated: 3, 6, 12, 24, 48, 96, 200, 400, and 800 mg; 16 weekly infusions were followed by Q2W dosing until disease progression5 Day 1: 0.06 mg/kg subcutaneous injection; day 4: 0.3 mg/kg; day 7: 1.5 mg/kg; followed by 1.5 mg/kg once weekly until PD or unacceptable toxicity In early-phase testing, dose escalation was 0.025-120 mg and dose expansion was 60 mg1 SELECT CONSIDERATIONS The most common AEs were hematologic events and CRS; the two-step-up priming regimen is intended to help mitigate the rate and severity of CRS3 The most common grade 3/4 TEAEs were hematologic; the most frequent TEAEs were fatigue and CRS (most CRS events were grade 1)4 The most common AEs were hematologic events and CRS. Note: ICANS events occurred in 4 patients but were all grade 1/2 and resolved without discontinuation7 The most common TEAEs were neutropenia, anemia, CRS, and fatigue1 THERAPY Elranatamab BCMA x CD3 Linvoseltamab BCMA x CD3 Teclistamab BCMA x CD3 ABBV-383 BCMA x CD3 Note 1: Although the BCMA antibody–drug conjugate belamaf received FDA Accelerated Approval in 2020, the manufacturer has initiated the process for withdrawal of the US marketing authorization based on findings from the DREAMM-3 phase III confirmatory trial. Note 2: Other bispecific BCMA and non-BCMA agents are also in rapid development, including TNB383b, talquetamab, cevostamab, and HPN217.
- 2. CAR-T Cell Therapy in Multiple Myeloma Current Status, Dosing, and Practical Considerations Full abbreviations, accreditation, and disclosure information available at PeerView.com/FNM40 1. Carvykti (ciltacabtagene autoleucel) Prescribing Information. https://www.fda.gov/media/156560/download. 2. Abecma (idecabtagene vicleucel) Prescribing Information. https://www.fda.gov/media/147055/download. REMS Cilta-Cel1 Approved in RRMM after ≥4 prior therapies, including an anti-CD38 mAb, a proteasome inhibitor, and an IMiD Recommended Dose Range 0.5-1.0 × 106 CAR-positive viable T cells (maximum dose of 1.0 × 108 CAR-positive viable T cells per single-dose infusion) Recommended Dose Range 300-460 × 106 CAR-positive viable T cells Ide-Cel2 Approved in RRMM after ≥4 prior therapies, including an anti-CD38 mAb, a proteasome inhibitor, and an IMiD General Principles for CAR-T Therapy Referral to a certified healthcare facility is required for collection of patient’s cells and administration of CAR-T therapy Avoid prophylactic use of dexamethasone or other systemic corticosteroids Premedicate with acetaminophen and an H1 antihistamine Monitor for CRS and ICANS and confirm tocilizumab availability before infusion Ide-cel and cilta-cel are available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) Monitor for neurologic events, hemophagocytic lymphohistiocytosis/ macrophage activation syndrome, and cytopenias Administer a lymphodepleting chemotherapy regimen of cyclophosphamide and fludarabine before CAR-T infusion Do not use a leukodepleting filter when administering