A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies
•
2 gefällt mir•206 views

Jonathan Corren, MD, and Monica Kraft, MD, prepared useful practice aids pertaining to severe asthma for this CME activity titled "A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2yC6zBd. CME credit will be available until November 6, 2019.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies
Ähnlich wie A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies (20)
Mehr von PVI, PeerView Institute for Medical Education
Mehr von PVI, PeerView Institute for Medical Education (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies
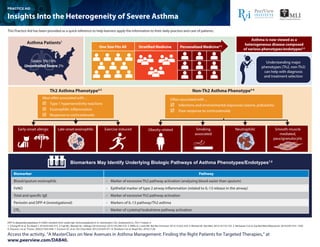
- 1. DPP-4: dipeptidyl peptidase-4; FeNO: exhaled nitric oxide; IgE: immunoglobulin E; IL: interleukin; LTE4: leukotriene E4; Th2: T helper 2. 1. Chung KF et al. Eur Respir J. 2014;43:343-373. 2. Fajt ML, Wenzel SE. J Allergy Clin Immunol. 2015;135:299-310. 3. Willis JC, Lord GM. Nat Rev Immunol. 2015;15:323-329. 4. Wenzel SE. Nat Med. 2012;18:716-725. 5. Mohanan S et al. Exp Biol Med (Maywood). 2014;239:1531-1540. 6. Douwes J et al. Thorax. 2002;57:643-648. 7. Erzurum SC et al. Clin Chest Med. 2012;33:459‐471. 8. Shiobara S et al. Respir Res. 2016;17:28. Access the activity, “A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies,” at www.peerview.com/DAB40. Th2 Asthma Phenotype4,5 Non-Th2 Asthma Phenotype4-6 Smoking associated Obesity relatedEarly-onset allergic Late-onset eosinophilic Exercise induced Neutrophilic Smooth-muscle mediated, paucigranulocytic Biomarkers May Identify Underlying Biologic Pathways of Asthma Phenotypes/Endotypes7,8 Asthma Patients1 One Size Fits All Stratified Medicine Personalized Medicine2,3 Most often associated with ... Type 1 hypersensitivity reactions Eosinophilic inflammation Response to corticosteroids Often associated with ... Infections and environmental exposures (ozone, pollutants) Poor response to corticosteroids Severe 5%-10% UncontrolledSevere 2% Asthma is now viewed as a heterogeneous disease composed of various phenotypes/endotypes2,4 Understanding major phenotypes (Th2, non-Th2) can help with diagnosis and treatment selection Biomarker Pathway Blood/sputum eosinophils • Marker of excessive Th2 pathway activation (analyzing blood easier than sputum) • Epithelial marker of type 2 airway inflammation (related to IL-13 release in the airway) • Marker of excessive Th2 pathway activation • Markers of IL-13 pathway/Th2 asthma • Marker of cysteinyl leukotriene pathway activation FeNO Total and specific IgE Periostin and DPP-4 (investigational) LTE4 Insights Into the Heterogeneity of Severe Asthma PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients.
- 2. CS: corticosteroid; FEV1: forced expiratory volume in 1 second; IgE: immunoglobulin E; IL: interleukin; SBM: subepithelial basement membrane; Th2: T helper 2; Th17: T helper 17. 1. Wenzel SE. Nat Med. 2012;18:716-725. 2. Mohanan S et al. Exp Biol Med (Maywood). 2014;239:1531-1540. 3. Douwes J et al. Thorax. 2002;57:643-648. Access the activity, “A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies,” at www.peerview.com/DAB40. Early-onset allergic Late-onset eosinophilic Exercise induced Smoking associated Obesity related Smooth-muscle mediated, paucigranulocytic Neutrophilic Non-Th2 Asthma Phenotype1-3 Th2 Asthma Phenotype1,2 Genetics 17q12; Th2-related genes Response to Therapy CS-responsive; Th2-targeted Responsive to anti–IL-5 therapy and cysteinyl leukotriene modifiers; CS-refractory Responsive to cysteinyl leukotriene modifiers, β agonists, and antibody to IL-9 Responsive to weight loss, antioxidants, and possibly hormonal therapy Possibly responsive to macrolide antibiotics Pathobiology and Biomarkers Specific IgE; Th2 cytokines; thick SBM CS-refractory eosinophilia; IL-5 Mast-cell activation; Th2 cytokines; cysteinyl leukotrienes Lack of Th2 biomarkers; oxidative stress No Th2 inflammation Sputum neutrophilia; Th17 pathways; IL-8 Clinical and Physiological Features Allergic symptoms and other diseases Possible asthma- COPD overlap syndrome Sinusitis; less allergic Mild; intermittent with exercise Low FEV1 ; more air trapping Primarily affects women; very symptomatic; airway hyper-responsiveness less clear Natural History Early onset (~3-10 y); mild to severe Adult onset; often severe Adult onset This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Features of Th2 and Non-Th2 Asthma Phenotypes PRACTICE AID
- 3. CRTh2: chemoattractant receptor-homologous molecule expressed on T-helper 2 cells; IgE: immunoglobulin E; IL-#R: interleukin-# receptor; TSLP: thymic stromal lymphopoietin. 1. Xolair (omalizumab) Prescribing Information. https://www.gene.com/download/pdf/xolair_prescribing.pdf. Accessed September 21, 2018. 2. Nucala (mepolizumab) Prescribing Information. http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125526Orig1s000Lbl.pdf. Accessed September 21, 2018. 3. Cinqair (reslizumab) Prescribing Information. http://cinqair.com/pdf/ PrescribingInformation.pdf. Accessed September 21, 2018. 4. Fasenra (benralizumab) Prescribing Information. https://www.azpicentral.com/fasenra/fasenra_pi.pdf#page=1. Accessed September 21, 2018. 5. Dupixent (dupilumab) Prescribing Information. https://www.regeneron.com/sites/default/files/Dupixent_FPI.pdf. Accessed October 22, 2018. 6. https://www.prnewswire.com/news-releases/ tezepelumab-granted-breakthrough-therapy-designation-by-us-fda-for-the-treatment-of-patients-with-severe-asthma-without-an-eosinophilic-phenotype-300708680.html. Accessed September 21, 2018. 7. https://clinicaltrials.gov/ct2/show/NCT03347279. Accessed September 21, 2018. 8. https://clinicaltrials.gov/ct2/show/NCT03406078. Accessed September 21, 2018. 9. Corren J et al. N Engl J Med. 2017;377:936-946. 10. https://clinicaltrials.gov/ct2/show/NCT02563067. Accessed September 21, 2018. 11. https://clinicaltrials.gov/ct2/show/NCT03052517. Accessed September 21, 2018. 12. https://clinicaltrials.gov/ct2/show/NCT02555683. Accessed September 21, 2018. Access the activity, “A MasterClass on New Avenues in Asthma Management: Finding the Right Patients for Targeted Therapies,” at www.peerview.com/DAB40. Agent/Target Indication/Current Status Route/Dosing Patients ≥6 y with moderate to severe persistent allergic asthma inadequately controlled with inhaled corticosteroids Subcutaneous 75 mg to 375 mg every 2-4 weeks (dosage based on IgE level and body weight) Add-on maintenance treatment of patients ≥12 y with severe asthma and an eosinophilic phenotype Subcutaneous 100 mg every 4 weeks Add-on maintenance treatment of patients ≥18 y with severe asthma and an eosinophilic phenotype Intravenous infusion 3 mg/kg every 4 weeks over 20-50 minutes Add-on maintenance treatment of patients ≥12 y with severe asthma and an eosinophilic phenotype Subcutaneous 30 mg every 4 weeks for first 3 doses, then every 8 weeks Add-on maintenance treatment of patients ≥12 years with moderate to severe asthma with an eosinophilic phenotype or with oral corticosteroid-dependent asthma Subcutaneous Initial dose of 400 mg followed by 200 mg every 2 weeks or initial dose of 600 mg followed by 300 mg every 2 weeks Phase 3 trials; breakthrough designation for noneosinophilic phenotype Subcutaneous 70 mg and 210 mg every 4 weeks and 280 mg every 2 weeks tested in phase 2 trials Phase 3 trials Oral Dupilumab5 IL-4Rα (IL-4/IL-13) Tezepelumab6-9 TSLP Fevipiprant10-12 CRTh2 Investigational Omalizumab1 IgE Mepolizumab2 IL-5 Reslizumab3 IL-5 Benralizumab4 IL-5Rα/βc Approved This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. A Guide to Biologic Therapies for Severe, Uncontrolled Asthma PRACTICE AID