

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Anticancer drugs 3 antimetabolites
Ähnlich wie Anticancer drugs 3 antimetabolites (20)
Mehr von Subramani Parasuraman
Mehr von Subramani Parasuraman (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Anticancer drugs 3 antimetabolites
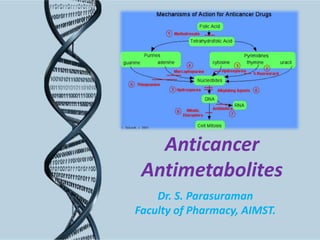
- 1. Anticancer Antimetabolites Dr. S. Parasuraman Faculty of Pharmacy, AIMST.
- 2. Antimetabolites Folate antagonist: Methotrexate (Mtx). Purine antagonist: 6-Mercaptopurine (6-MP), 6-Thioguanine (6-TG), Azathioprine, Fludarabine. Pyrimidine antagonist: 5-Fluorouracil (5-FU), Capecitabine Cytarabine (cytosine arabinoside).
- 3. Antimetabolites • Antimetabolites are structurally compounds that exist within the cell. related to normal • Antimetabolites generally interfere with the availability of normal purine or pyrimidine nucleotide precursors, either by inhibiting their synthesis or by competing with them in DNA or RNA synthesis. • Their maximal cytotoxic effects are in S-phase (and are, therefore, cell-cycle specific).
- 5. Folate antagonist: Methotrexate Mechanism of action: • Folic acid is an essential dietary factor. It is converted by enzymatic reduction to a series of tetrahydrofolate cofactors that provide carbon groups for the synthesis of precursors of DNA (thymidylate and purines) and RNA (purines). • Methotrexate inhibits the enzyme dihydrofolate reductase (DHFR). Inhibition of DHFR leads to partial depletion of the tetrahydrofolate cofactors (5, 10-methylene tetrahydrofolic acid and N10-formyl tetrahydrofolic acid) required for the respective synthesis of thymidylate and purines. • In addition, methotrexate undergoes conversion to a series of polyglutamates (MTX-PGs) in both normal and tumor cells and inhibits the thymidylate synthase (TS).
- 6. Folate antagonist: Methotrexate • The inhibition of DHFR can only be reversed by a thousand fold excess of the natural substrate, dihydrofolate, or by administration of leucovorin. Folinic acid, Thymidine also counteracts MTX toxicity. Resistance • Non-proliferating cells are resistant to MTX. Resistance in neoplastic cells can be due to amplification (production of additional copies) of the gene that codes for DHFR, resulting in increased levels of this enzyme.
- 7. Folate antagonist: Methotrexate Therapeutic uses: • MTX, usually in combination with other drugs, is effective against acute lymphocytic leukemia, choriocarcinoma, Burkitt lymphoma in children, breast cancer, and head and neck carcinomas. In addition, low-dose MTX is effective as a single agent against certain inflammatory diseases, such as severe psoriasis and rheumatoid arthritis as well as Crohn disease.
- 8. Folate antagonist: Methotrexate Pharmacokinetics: • Oral, intramuscular, intravenous intrathecal routes of administration. (IV), and • MTX is metabolized to polyglutamate derivatives. High doses of MTX undergo hydroxylation at the 7 position and become 7-hyroxymethotrexate. • It is less water soluble • MTX is less water soluble and may lead to crystalluria (Therefore, it is important to keep the urine alkaline and the patient well hydrated to avoid renal toxicity). • Excretion of the parent drug and the 7-OH metabolite occurs primarily via urine.
- 9. Folate antagonist: Methotrexate Adverse effects: • MTX causes stomatitis, myelosuppression, erythema, rash, urticaria, and alopecia. • Most frequent toxicities: nausea, vomiting, and diarrhea. • Adverse effects can be prevented or reversed by administering leucovorin. • Hepatic function: Long-term use of MTX may lead to cirrhosis. • Renal function: Variable • Neurologic toxicities: subacute meningeal irritation, stiff neck, headache, and fever. Rarely, seizures, encephalopathy or paraplegia occur. • Contraindications: Because MTX is teratogenic in experimental animals and is an abortifacient, it should be avoided in pregnancy.
- 11. Purine antagonist: 6-Mercaptopurine • These are highly effective antineoplastic drugs. • 6-Mercaptopurine is the thiol analog of hypoxanthine. 6-MP and 6-thioguanine were the first purine analogs to prove beneficial for treating neoplastic disease (Azathioprine, an immunosuppressant, exerts its cytotoxic effects after conversion to 6-MP). • Purine antagonist used for the treatment of malignant diseases (mercaptopurine, thioguanine), but also for immunosuppression (azathioprine) and antiviral chemotherapy (acyclovir, ganciclovir, vidarabine, and zidovudine)
- 12. Purine antagonist: 6-Mercaptopurine • Mechanism of action: • 6-MP inhibit the conversion of inosine monophosphate to adenine and guanine nucleotides that are building blocks for RNA and DNA. – Nucleotide formation: 6-MP converted to the nucleotide analog, 6-MPribose phosphate (6-thioinosinic acid, or TIMP) – Inhibition of purine synthesis: TIMP can inhibit the first step of de novo purine-ring biosynthesis – Incorporation into nucleic acids: TIMP is converted to thioguanine monophosphate (TGMP), which after phosphorylation to di- and triphosphates can be incorporated into RNA. The deoxy-ribonucleotide analogs that are also formed are incorporated into DNA. This results in nonfunctional RNA and DNA.
- 13. Purine antagonist: 6-Mercaptopurine Pharmacokinetics: • Oral administration, well distributed except for the cerebrospinal fluid. • Metabolized in the liver, 6-MP is converted to the 6-ethylmercaptopurine derivative or to thiouric acid. • The parent drug and its metabolites are excreted by the kidney. Adverse effects: • Bone marrow depression is the principal toxicity. Side effects also include anorexia, nausea, vomiting, and diarrhea. Occurrence of hepatotoxicity in the form of jaundice has been reported in about one third of adult patients. • Dose: 2.5 mg/kg/day
- 14. Purine antagonist: Azathioprine • This antipurine acts by getting converted to 6-MP, and has more immunosuppressant action. • Inhibits the nucleic acid synthesis and suppresses cell mediated immunity. Because of this effect azathiaprine is used mainly in autoimmune disease (rheumatoid arthritis, ulcerative colitis) and organ transplantation. • Dose: 3-5 mg/kg/day • The main toxic effect of antipurines is bone marrow depression, which develops slowly.
- 15. Purine antagonist: 6-Thioguanine • 6-Thioguanine is purine analog, is primarily used in the treatment of acute nonlymphocytic leukemia in combination with daunorubicin and cytarabine. • MOA: Like 6-MP, 6-TG is converted intracellularly to TGMP (6-thioguanylic acid) by the enzyme Hypoxanthineguanine phosphoribosyltransferase (HGPRT) TGMP is further converted to the di- and triphosphates, thioguanosine diphosphate and thioguanosine triphosphate which inhibits the biosynthesis of purines and also the phosphorylation of GMP to guanosine diphosphate
- 16. Purine antagonist: 6-Thioguanine • Pharmacokinetics: Similar to 6-MP. • Adverse effects: Bone marrow depression is the dose-related adverse effect. 6-TG is not recommended for maintenance therapy or continuous long-term treatments due to the risk of liver toxicity.
- 17. Purine antagonist: Fludarabine • It is a prodrug, useful in the treatment of chronic lymphocytic leukemia. Fludarabine is also effective against hairy cell leukemia and indolent non-Hodgkin lymphoma. • Phosphorylated intracellularly to the active triphosphate form which inhibits DNA polymerase dysfunctional DNA. • Prominent adverse effects are chills, fever and vomiting after injection, myelosuppression and opportunistic infections.
- 19. Pyrimidine antagonist: 5-Fluorouracil • In system, 5-fluorouracil is converted in to 5-fluoro-2deoxyuridine monophosphate (5-FdUMP), which inhibits thymidylate synthase (form covalent ternary complex with methyl-THFA and thymidylate synthase irreversible inhibition of TS) and blocks the conversion of deoxyuridilic acid to deoxythymidylic acid. • 5-FU incorporated into RNA, interferes with RNA synthesis and causing cytotoxic effect. • 5-FU produces the anticancer effect in the S phase of the cell cycle. • 5-FU is employed primarily in the treatment of slowly growing solid tumors (for example, colorectal, breast, ovarian, pancreatic, and gastric carcinomas).
- 20. Pyrimidine antagonist: 5-Fluorouracil • Pharmacokinetics: Because of its severe toxicity to the GI tract, 5-FU is given IV or, in the case of skin cancer, topically. • Adverse effects: Nausea, vomiting, diarrhea, and alopecia, severe ulceration of the oral and GI mucosa, bone marrow depression (with bolus injection), and anorexia are frequently encountered. • 5-FU causes “hand-foot syndrome” is seen after extended infusions
- 21. Pyrimidine antagonist: Capecitabine • It is a oral fluoropyrimidine carbamate, approved for the treatment of resistant metastatic breast cancer (2nd line treatment of metastatic breast cancer along with taxanes). • It is a orally active prodrug of 5-FU. • After absorption it will convert into the deoxy-5-fluorouridine in the liver. • Adverse effects: These are similar to those with 5-FU.
- 22. Pyrimidine antagonist: Cytarabine • This is a cytidine (nucleoside molecule formed when cytosine is attached to a ribose ring) analogue. • It is phosphorylated in the body to the corresponding nucleotide which inhibits DNA synthesis. • The triphosphate of cytarabine is an inhibitor of DNA polymerase and blocks generation of cytidilic acid. • Cytarabine is cell cycle specific and act primarily during ‘S’ phase. • Its main use is to induce remission in acute leukaemia in children, also in adults. Other uses are-Hodgkin's disease and non-Hodgkin lymphoma.
- 23. Pyrimidine antagonist: Cytarabine • Pharmacokinetics: not effective when given orally; IV • Adverse effects: Nausea, vomiting, diarrhea, and severe myelosuppression (primarily granulocytopenia) are the major toxicities associated with cytarabine. Hepatic dysfunction is also occasionally encountered. • At high doses or with intrathecal injection, cytarabine may cause leukoencephalopathy or paralysis.
- 24. Thank you
Hinweis der Redaktion
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine
- Trimethoprim; pyrimethamine