Empfohlen

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Poster Presentation 07_08 (2)
Ähnlich wie Poster Presentation 07_08 (2) (20)
Poster Presentation 07_08 (2)
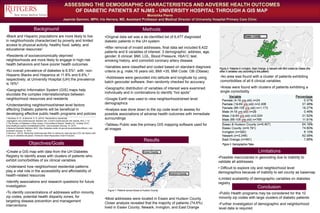
- 1. ASSESSING THE DEMOGRAPHIC CHARACTERISTICS AND ADVERSE HEALTH OUTCOMES OF DIABETIC PATIENTS AT NJMS - UNIVERSITY HOSPITAL THROUGH A GIS MAP Monishka Pierre Jeannie Garmon, MPH; Iris Herrera, MD, Assistant Professor and Medical Director of University Hospital Primary Care Clinic Background •Create a GIS map with data from the UH Diabetes Registry to identify areas with clusters of patients who exhibit comorbidities of six clinical variables •Understand how neighborhood residential patterns play a vital role in the accessibility and affordability of health-related resources •Identify associations and research questions for future investigation •To identify concentrations of addresses within minority zip codes, potential health disparity zones, for targeting disease prevention and management interventions Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.*Statistics are for 2000-2004, age-adjusted to the 2000 U.S. standard million population, and represent the number of new cases of invasive cancer and deaths per year per 100,000 women.* •Black and Hispanic populations are more likely to live in neighborhoods characterized by poverty and limited access to physical activity, healthy food, safety, and educational resources1 •Residents of socioeconomically deprived neighborhoods are more likely to engage in high-risk health behaviors and have poorer health outcomes •NJ overall prevalence of diabetes is 6.5%2, with non- Hispanic Blacks and Hispanics at 11.8% and 6.6%,3 respectively; at University Hospital (UH) the prevalence is 16%4 •Geographic Information System (GIS) maps help elucidate the complex interrelationships between neighborhood resources and residents •Understanding neighborhood/street level factors affecting Diabetic patients will be beneficial in developing effective public health programs and policies _____________________________________________________________________________________________________________________________________________ 1.Kershaw, K. N., & Albrecht, S. S. (2015). Racial/ethnic residential segregation and cardiovascular disease risk. Current cardiovascular risk reports, 9(3), 1-12. 2.The Burden of Diabetes in New Jersey: A Surveillance Report. Healthy NJ. October 2010. www.healthynj.org/dis-con/diabetes/nj.html. Last accessed January 14, 2010. 3.National Diabetes Statistics 2007. http://diabetes.niddk.nih.gov/dm/pubs/statistics/#race. Last accessed January 14, 2010. 4.Herrera,I. (2012). Reducing Cardiovascular Risk in Latinos by reducing key CVD risk factors with a focus on diabetes education. American Heart Association Grant Proposal. •Original data set was a de-identified list of 6,477 diagnosed diabetic patients in the UH system •After removal of invalid addresses, final data set included 6,422 patients and 9 variables of interest: 3 demographic: address, age, gender; 6 clinical: BMI, LDL, Blood Pressure, HbA1C test, smoking history, and comorbid coronary artery disease •Variables were classified and coded based on standard diagnosis criteria (e.g. male,16 years old, BMI =35, BMI Code: OB (Obese) •Addresses were geocoded into latitude and longitude by using batch geocoder software, then randomly checked for accuracy •Geographic distribution of variables of interest were examined individually and in combinations to identify “hot spots” •Google Earth was used to view neighborhood/street level demographics •Analysis was done down to the zip code level to assess for possible associations of adverse health outcomes with immediate surroundings •Tableau Public was the primary GIS mapping software used for all images . •No area was found with a cluster of patients exhibiting comorbidities of all 6 clinical variables •Areas were found with clusters of patients exhibiting a single comorbidity •Public Health programs may be considered for the 10 minority zip codes with large clusters of diabetic patients •Further investigation of demographic and neighborhood level data is required •Most addresses were located in Essex and Hudson County. Closer analysis revealed that the majority of patients (74.6%) lived in Essex County; Newark, Irvington, and East Orange •Possible inaccuracies in geocoding due to inability to validate all addresses • Difficult to explore city and neighborhood level demographics because of inability to set county as basemap •Limited availability of demographic variables on diabetes registry Objectives/Goals Methods Results Limitations Conclusion