1. Time from Surgery to First Adjuvant Chemotherapy: Experiences at an Inner City Canadian Hospital
C. Marchand1*, M. Hassan1, L. Sevick1, N. Baxter1, J. Ebrahim1, A. Bookwala1, A. Ansari1, A. Wong1, S. Hogeveen1, R. Nisenbaum2, D. Topic3, C. Brezden-Masley1.
1Medical Oncology, St. Michael’s Hospital, Toronto, Canada
2Centre for Research on Inner City Health, St. Michael’s Hospital, Toronto Canada
3Medical Oncology, Sindi Ahluwalia Hawkins Centre for the Southern Interior (BCCA), Kelowna, Canada
ABSTRACT
Background: Cancer Care Ontario (CCO) guidelines advise that colorectal cancer (CRC) patients
receive their first adjuvant chemotherapy (AC) no later than 8 weeks after surgical resection, with
new data suggesting optimal treatment to commence between 4 and 6 weeks. This retrospective
study was performed to determine treatment timelines and identify barriers at St. Michael’s
Hospital (SMH).
Methods: Of the 507 patients diagnosed with CRC between January 1, 2005 and May 1, 2012 at
SMH, 304 patients had stage II or III CRC. Our sample population of 159 patients received both
surgical resection and AC at SMH. Data collected included: time between surgery and first AC,
patient demographics, systemic/clinical barriers and recurrence-free survival. Data was analyzed
using SAS statistical software assuming p-values <0.05 as significant.
Results: Of our 159 patients, mean age was 61.3 years (range 28 – 91); 54% male and 70% had
stage III disease; colon cancer (64%) and mean follow-up was 2.2 years (range 0.1 – 5.7). Mean
time from surgery to first AC was 50.4 days (SD = 15.8) or 7.2 weeks (range 3-17). Medical
complications affected 21.4% of patients. The presence of a complication was associated with delay
in AC (9.5 days, p=0.001). Moreover, 11.1% of patients were excluded from sample, since
complications exceeded treatment past 12 weeks, equating to no AC. Referral from surgeon
averaged 21 days (SD=12.0), 10 days awaiting pathology. Medical Oncology consult to first AC
averaged 19 days (SD=12.7), 12 days awaiting port-a-cath insertion. Each part of the referral
process was correlated with delay to AC. Only 18.9% of patients recurred. While trends were
identified, association between delay and recurrence was weak (p=0.146). Medical complication
correlated strongly with recurrence (p=0.047). Patients with complications had a higher rate of
recurrence (32.4% vs 15.2%).
Conclusions: Compliance to current CCO guidelines can be optimized in CRC patients at SMH.
Barriers to timely treatment include patient age, timely referral and presence of a medical
complication. Quality improvement rapid cycling of confounding barriers will be used
prospectively to lower variance and achieve greater consistency in treatment.
BACKGROUND
• The initiation of systemic adjuvant
chemotherapy (AC) in stage II and III
colorectal cancer (CRC) patients has
become a point of significant importance
in the successful treatment of patients
• A meta-analysis of previous studies,
determined that optimal survival benefits
come to patients who receive AC 4-6
weeks after surgery (Biagi et al, 2005)
• In this study, the primary focus is
whether a delay in the initiation of AC
affects disease free survival (DFS) or
overall survival (OS) (delay defined as >
four weeks from surgical resection of
primary tumour.)
METHODS
• This study received REB
approval from SMH
• Potentially eligible patients
were reviewed retrospectively
• Eligible patients were
identified through Medical
Oncologist new patient
records at SMH
• Table 1 shows the patient
selection criteria
RESULTS
We would like to thank Rob Grandy and Sanofi Aventis Canada Inc for
their unrestricted educational grant in support of this project.
We would also like to acknowledge all the surgeons that operated on
the included patients. Specifically we would like to thank: Dr. Ahmed,
Dr. Baxter, Dr. Burnstein, Dr. George, Dr. Grantcharov, Dr. Lawless,
Dr. Mustard, Dr. Nathans, and Dr. Rotstein.
TABLE 2: Patient Demographics
Patient Demographic Results/Data Collected
Age Mean age : 61.3 years Range: 28-91 years
Gender Male: 54% Female: 46%
Stage of Disease Stage II: 30% Stage III: 70%
Type of Cancer Colon cancer: 64% LARC: 36%
Medical Complications With: 21% Without: 79%
Recurrence Yes: 18.9% No: 81.1%
TIMELINE
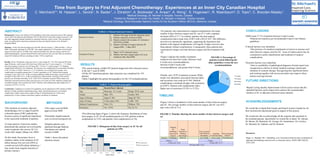
• The following figure (Figure 1) shows the frequency distribution of time
from surgery to AC for all included patients (n=159), patients without
complication (n=125), and patients with complications (n=34)
CONCLUSIONS
• SMH treats 37.1% of patients between 4 and 6 weeks.
• Patients are treated as per recommended Cancer Care Ontario
guidelines.
• Clinical barriers were identified.
• The presence of a medical complication is known to increase wait
times between surgery and first AC. Areas of improvement may be
considered in earlier identification and treatment of surgical
complications.
• Systemic barriers were identified.
• Time to availability of pathological diagnosis (formal report) was
recognized as a barrier to timely medical oncology referral and
initiation of systemic therapy. Recognizing this significant barrier
and working together with service providers may improve these
barriers moving forward.
TABLE 1: Patient Selection Criteria
Inclusion Criteria:
i. Patients with stage II and III colorectal cancer.
ii. Patients surgically resected at SMH.
iii. Patients treated with systemic AC (Xeloda or
FOLFOX) at SMH.
iv. Patients with date of surgery between 29-
August-2005 – 1-May-2012
Exclusion Criteria:
i. Stage I or IV colorectal cancer.
ii. Patients who have surgery and/or AC at an
institution other than SMH.
• Figure 3 shows a breakdown of the mean number of days between surgery
and AC. The average number of days between surgery and AC was 50.4
days with a SD of 15.8.
FIGURE 3: Timeline showing the mean number of days between surgery and
AC
Waiting
for
pathology
report post
surgery
From
Surgeon to
Medical
Oncologist
First Consult
with Medical
Oncologist
Awaiting
CVAD insertion
First treatment
with AC
Surgery Pathology Referral 1st Consult Port-a-cath Chemotherapy
10 days 12 days
21 days (sd: 12.0) 19 days (SD: 12.7)
50.4 days (SD: 15.8)
Resources:
Biagi, J.J., Raphael, M.J., Mackillop, et al. Association between time to initiation of
adjuvant chemotherapy and survival in colorectal cancer. JAMA 2005 305(22):
2335-2342.
FUTURE DIRECTIONS
• Rapid Cycling Quality Improvement will be used to ensure that the
identified barriers can be improved to achieve the recommended
timeline of AC in adjuvant colorectal cancer patients.
0
10
20
30
40
50
60
21-34 35-46 47-58 59-70 71-82 83-94 95-106 107-118
NumberofPatients
Number of Days
FIGURE 1: Histogram of time from surgery to AC for all
patients (n=159)
With Complications
Without Complications
ACKNOWLEDGEMENTS
• The search strategy yielded 507 patients diagnosed with colorectal cancer
in the last 7 years at SMH
• Of the 507 identified patients, data extraction was completed for 159
patients
• Table 2 highlights the patient demographics for the 159 included patients
• For patients who experienced no surgical complications, the mean
number of days between surgery and AC was 47.5 with a standard
deviation (SD) of 13.7. In contrast, patients who had surgical
complications had a mean time of 60.9 with a SD of 18.4. This difference
proved to be statistically significant, supporting the hypothesis that
patients with surgical complications will require a longer recovery time
than patients without complications. Consequently, these patients also
experienced a longer wait time between surgery and first treatment with
AC.
5%
26%
38%
31%
FIGURE 2: Percentage of
patients treated following the
older guidelines versus the new
recommendations
<4 weeks
4-6 weeks
6-8 weeks
>8 weeks
• Figure 2 depicts the number of patients
treated at less than four weeks, between 4 and
6 weeks (new recommendations,
between 6 and 8 weeks (old
recommendations), and greater than 8 weeks.
• Finally, only 18.9% of patients recurred. While
trends were identified, association between delay
and recurrence was weak (p=0.146). Medical
complications correlated strongly with recurrence
(p=0.047). Patients with complications had a
higher rate of recurrence (32.4% vs 15.2%).